Abstract
Objectives:
Patient-specific instrumentation (PSI) based on three-dimensional (3D) computed tomography imaging (CT) is increasingly being used for corrective high tibial osteotomies (HTO’s) and distal femoral osteotomies (DFO’s). These PSI cutting guides are based off of measurements on a 3D CT, however plain radiographs are typically used during the pre-operative evaluation to determine the need for an osteotomy, and it is unclear how well measurements on plain radiographs correlate to those performed on 3D CT.
The purpose of this study was to evaluate the correlation between measurements of coronal alignment and posterior tibial slope (PTS) on plain radiographs and measurements by semi-automated PSI software on 3D CT. It was hypothesized that coronal and posterior tibial slope measurements on plain radiographs would significantly correlate with measurements on 3D CT by PSI software.
Methods:
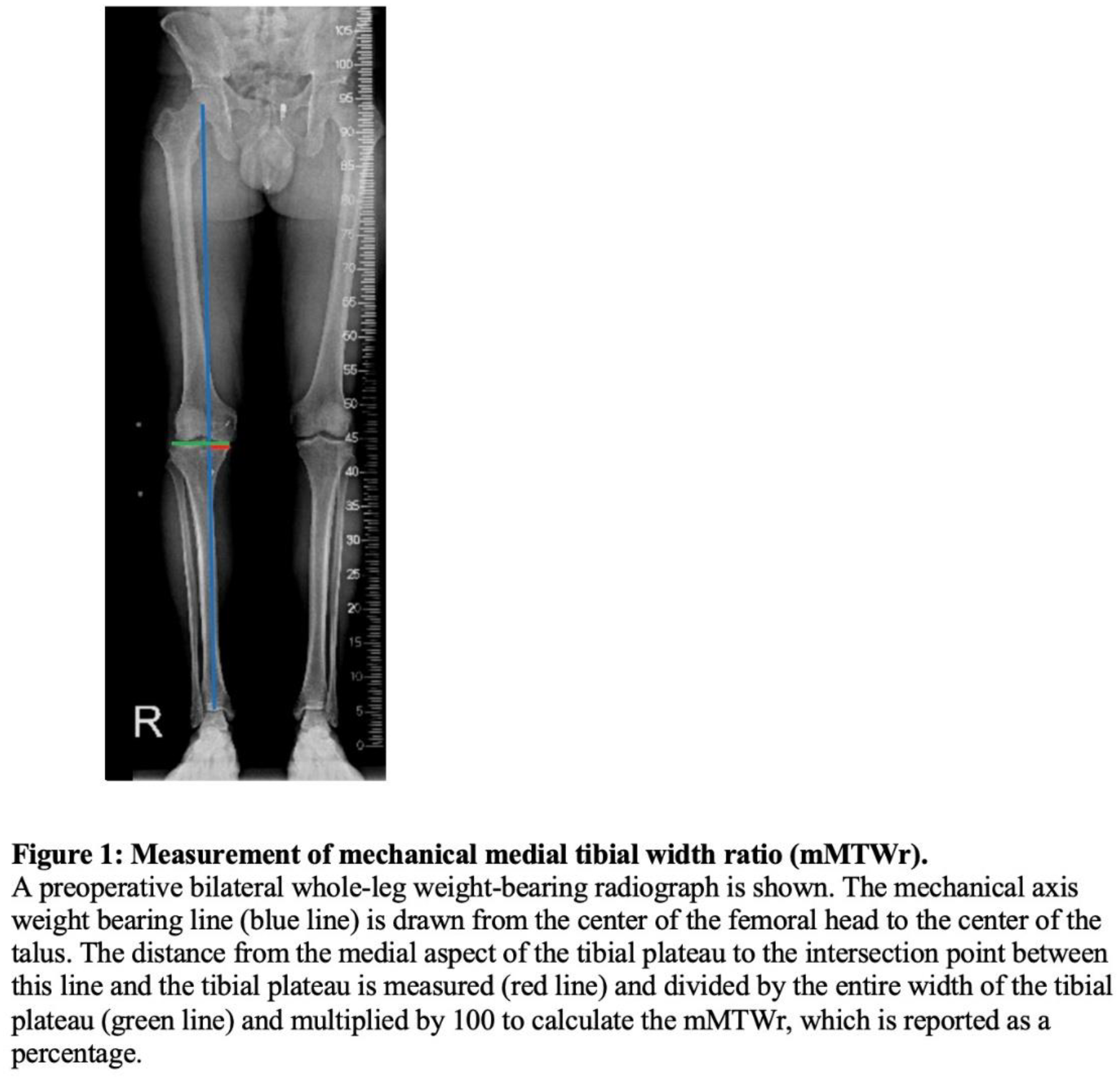
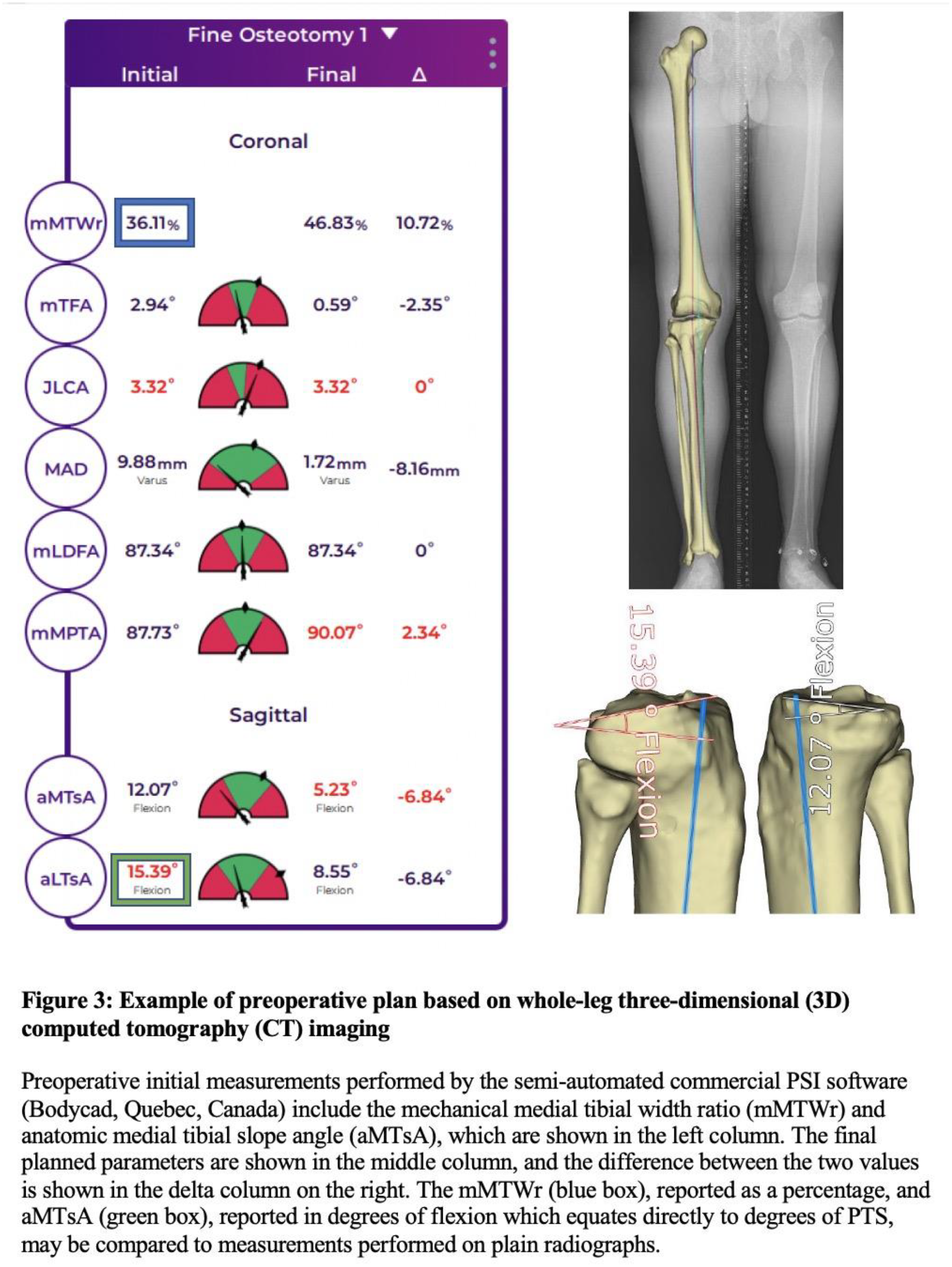
Patients who underwent hip to ankle CT as part of the pre-operative workup prior to a opening wedge (oW) or closing wedge (cW) HTO or DFO from October 2020 to November 2023 were reviewed. Mechanical medial tibial width ratio (mMTWr, Figure 1) and medial PTS (Figure 2) were evaluated pre-operatively by two independent raters, orthopaedic sports medicine fellows, on standing whole-leg radiographs and a lateral radiograph of the knee, respectively. Lateral radiographs were excluded if they were malrotated, defined as greater than 5 mm distance between the posterior aspect of the medial and lateral femoral condyles. The mMTWr and PTS using the full length tibial anatomic axis were measured on 3D CT utilizing semi-automated commercial PSI software (Bodycad, Quebec, Canada) without any surgeon involvement (Figure 3).
Intra-class correlation coefficients were calculated to determine the inter-rater reliability between raters and between the raters and the PSI software for each measurement. Pearson’s correlation coefficient and an independent t-test were respectively used to analyze for a correlation and difference between the raters’ and PSI software’s measurements. Significance was set at p<0.05.
Results:
Complete data sets were obtained for 91 cases (43 oW-HTO, 17 cW-HTO, 24 oW-DFO, 4 cW-DFO, 1 rotational HTO, 1 combined cW-HTO and oW-DFO, 1 combined cW-HTO and cW-DFO). 11 patients were excluded from PTS measurements due to malrotated lateral knee radiographs. Demographics for the cohort are shown in Table 1.
The ICC between raters for pre-operative mMTWr measurements was 0.99. The ICC between the raters’ measurements of mMTWr on whole-leg standing radiographs and the PSI measurements of mMTWr based on the 3D CT was 0.99, and these two measurements were significantly correlated (r=0.99, p<0.001). There was no difference between the raters’ (40.8% ± 23.5) and the PSI measurement of mMTWr (41.3% ± 22.1, p>0.05).
The ICC’s between raters for pre-operative PTS measurements was 0.82. The ICC between the raters’ measurements of PTS on standard lateral knee radiographs and PSI measurements of medial PTS based on the 3D CT was 0.63, and these two measurements were significantly correlated (r=0.72, p<0.001). There was a significant difference between the raters’ measurements (10.4° ± 3.4) and the PSI measurements of PTS (12.0° ± 3.2, p<0.001).
Conclusions:
This study found that coronal measurements performed on standard whole-leg radiographs and by semi-automated PSI software on 3D CT and standing whole-leg radiographs are highly correlated with near perfect agreement between modalities. PTS measurements had moderate correlation between plain radiographs and 3D CT, and PTS on lateral knee radiographs was, on average, 1.6° less than 3D CT, which utilizes the full-length tibia. Although the absolute value of slope is different between modalities, these data are important as they confirm that PTS on plain radiographs is a moderately reproducible measurement which correlates highly with 3D CT.
Altogether, these data confirm that measurements on standing whole-leg and lateral knee radiographs are reproducible and accurate for evaluating coronal alignment and PTS pre-operatively.