Abstract
Objectives:
The purpose of this study was to compare 10-year outcomes among patients with unstable chondral lesions (CL-noDeb) and patients without unstable chondral lesions (NoCL) found at the time of arthroscopic partial meniscectomy (APM).
Methods:
We conducted a secondary analysis of data from the Chondral Lesions and Meniscal Procedures Trial (ChAMP) level 1 trial at 10-year follow-up. One-hundred-fifteen patients had 10-year outcomes for CL-noDeb vs. NoCL groups, including the Western Ontario and McMaster Universities Arthritis Score (WOMAC), Knee Injury and Osteoarthritis Outcomes Score (KOOS), Visual Analog Scale (VAS), Short-form Health Survey (SF-36) and subsequent surgeries. A physical assessment was performed by a trained research assistant. Two surgical orthopaedic sports medicine fellows assessed joint space narrowing on weight-bearing radiographs. Our primary outcome was WOMAC Pain score. Continuous variables were compared with t-tests and linear regression and categorical variables were compared with chi-squared tests, Fisher Exact Tests, and logistic regression. Regression models obtained mean differences (MDs) with corresponding 95% confidence intervals by adjusting for weight. Statistical significance was defined as p < 0.05.
Results:
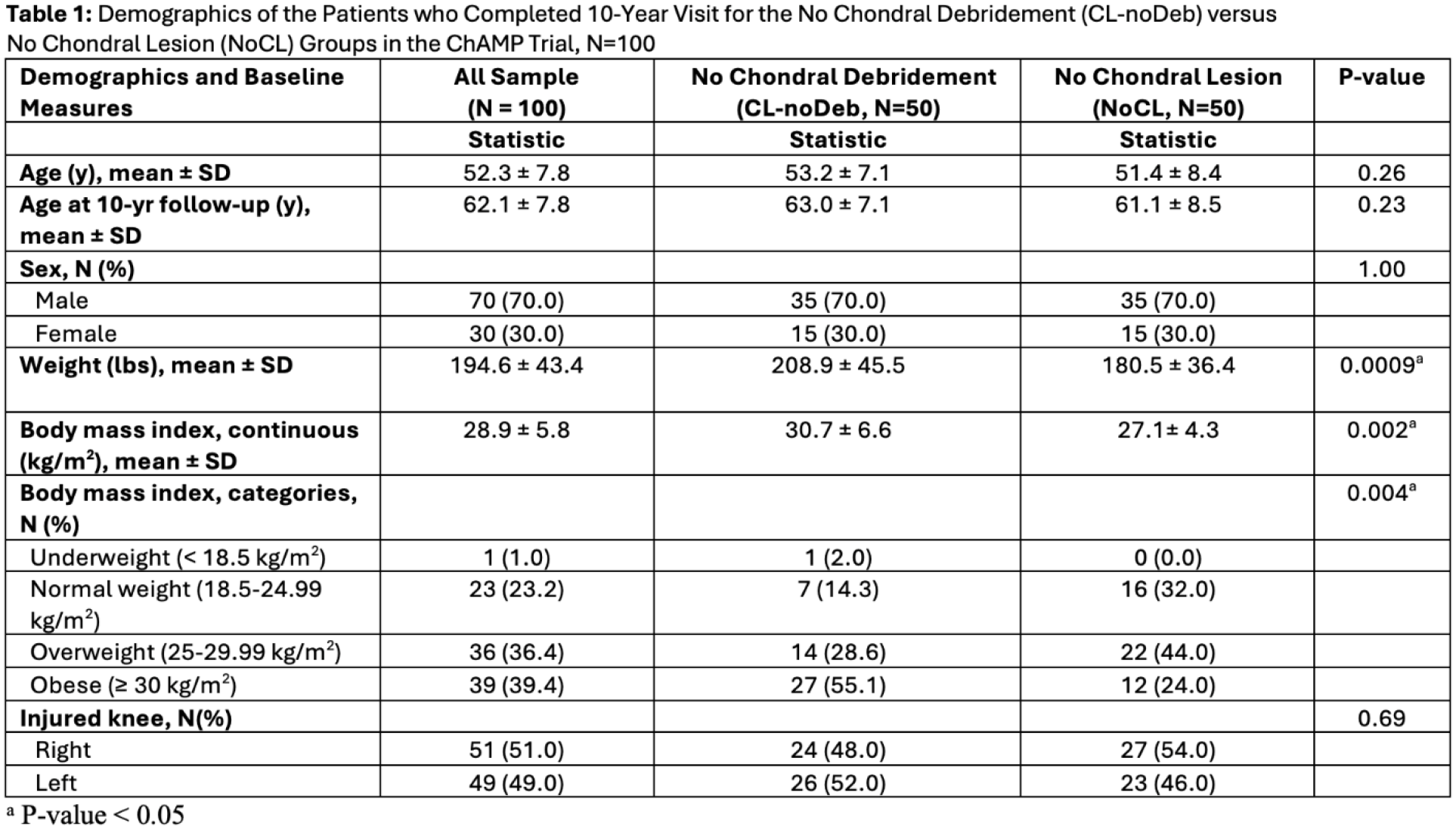
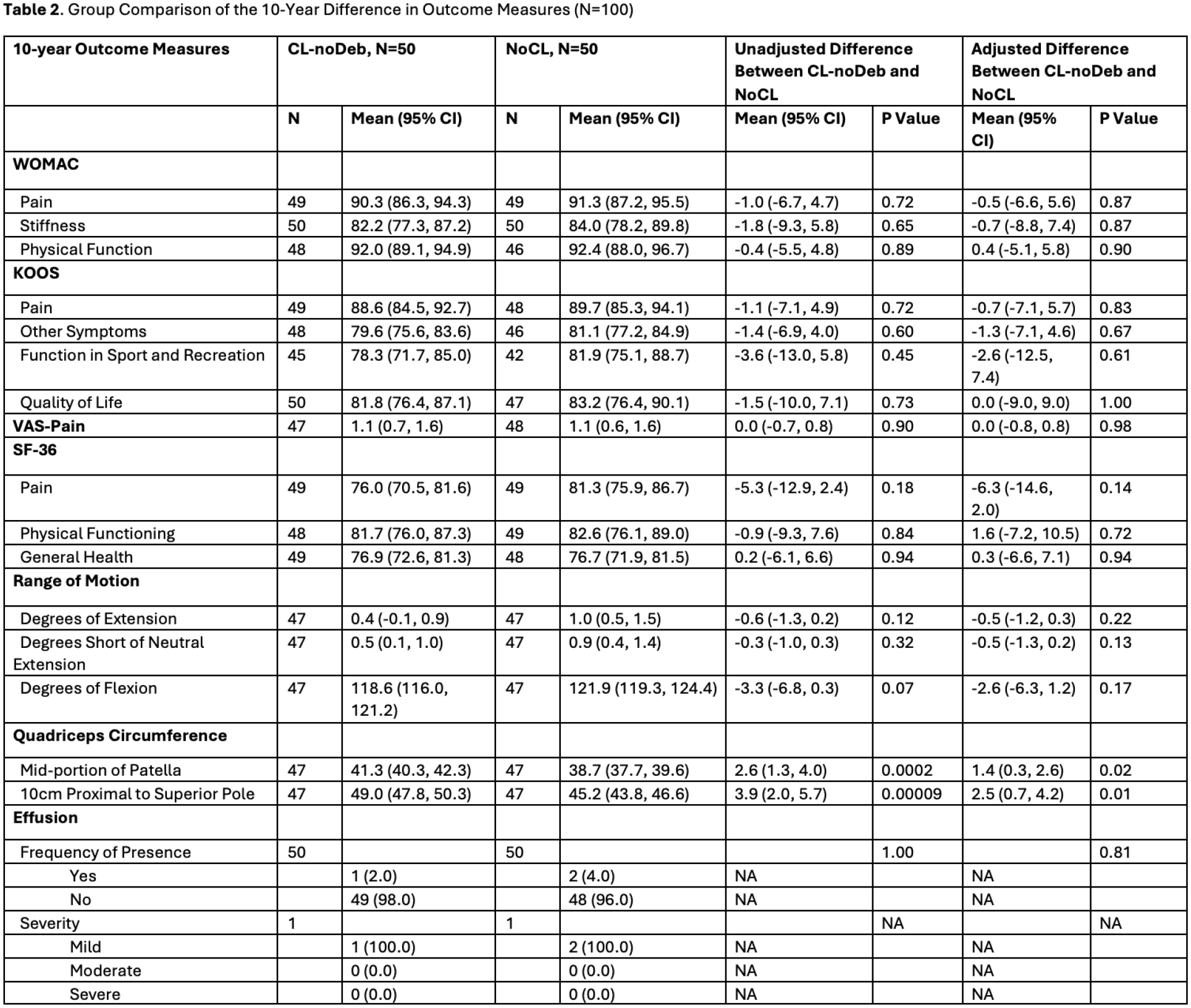
Of the original sample of 163 patients (CL-noDeb 92, NoCL 71), 115 (CL-noDeb 64 [69.6%] and NoCL 51 [71.8%], p=0.888) had outcomes. There were no significant demographic differences between the two groups, aside from preoperative weight and BMI (Table 1). Fifteen patients underwent subsequent surgery (Figure 1). Among those who did not have later surgery, there was no significant difference in the WOMAC pain between the CL-noDeb (90.3 [95% CI, 86.3-94.3]), and the NoCL group (91.3 [95% CI, 87.2-95.5]). There was also no significant difference in other patient reported outcome measures, range of motion (Table 2), or joint space narrowing. However, there was a significantly lower rate of subsequent surgery in the NoCL group compared to the CL-noDeb group for both the index and contralateral leg (Figure 2).
Conclusions:
This 10-year follow-up level 1 study of patients who underwent APM found that the presence of unstable chondral lesions was associated with a significantly higher rate of subsequent arthroplasty. Patients without unstable chondral lesions had more favorable outcomes at 10-year follow-up. Careful preoperative assessment and selection criteria for APM may help educate patients and reduce the rate of post-meniscectomy arthroplasty.