Abstract
Objectives:
Distal femoral varus osteotomy (DFVO) is a well-described treatment option for patients with valgus malalignment associated with a broad range of knee disorders. Biomechanical studies have confirmed the role of DFVO in unloading the lateral compartment and correcting the mechanical axis of the lower limb. Previous studies reported that medial closing wedge (MCW)-DFVO may be a useful concomitant procedure in young patients with focal chondral defects and osteoarthritis in lateral compartment and/or patellofemoral (PF) instability. MCW-DFVO reduces the Q angle and unloads the PF compartment laterally and may improve patellar tracking, thereby decreasing PF pain and instability in select patients. However, how the distribution of actual stress within each compartment changes after DFVO remains unclear. No in vivo studies have been conducted to clarify the stress distribution pattern of the femorotibial (FT) and PF joints after DFVO. The distribution of the subchondral bone mineral density is thought to be correlated with the distribution of stress over the joint surface. Computed tomography (CT) osteoabsorptiometry is an analytical method to assess long-term stress distribution over individual joints in living participants by measuring subchondral bone density. Our previous studies using this method have evaluated stress distribution at each joint under various loading conditions. The purpose of this study was to evaluate change in the pattern of subchondral bone density distribution of the PF joints in patients with valgus knee before and after MCW-DFVO.
Methods:
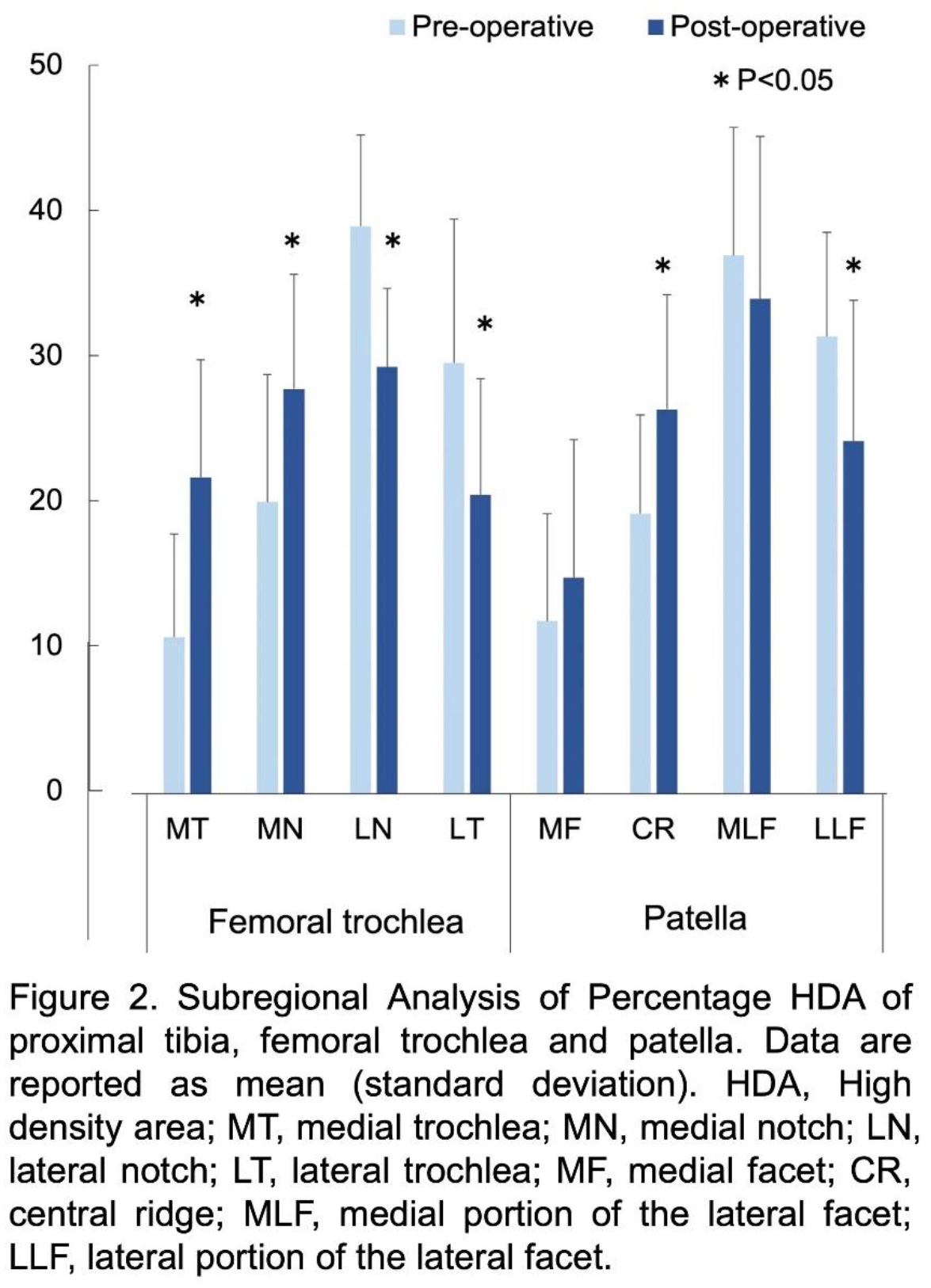
This study design had been accepted by the institutional review board clearance in our hospital. Thirteen patients (14 knees) who underwent MCW-DFVO for lateral compartment osteoarthritis and spontaneous necrosis of the knee with valgus deformity from June 2016 to May 2021 were enrolled prospectively in this study. There were 2 men and 11 women with a mean age of 43.5 years (range; 22 to 73 years) at the time of surgery. In surgical procedure, we performed a biplanar osteotomy of the distal femur. Then, the oblique osteotomy site was gradually closed. A locking plate was fixed to the medial side of the femur. After surgery, weight-bearing was permitted at 3 weeks after surgery. Clinical and radiological evaluations were performed in all cases before surgery and at the final follow-up (mean; 35.4 months, 12 to 62 months). The distribution patterns of subchondral bone density through the articular surface of proximal tibia, femoral trochlea and patella were assessed before and more than 1 year after surgery using a CT osteoabsorptiometry method. Hounsfield units (HU) of the identified subchondral bone region in each slice were measured at each coordinate point with 1-mm intervals. The quantitative analysis of the obtained mapping data focused on location of the high density area (HDA) through the articular surface. HDA was defined as the area where the HU values are in the top 30% of HU out of the total area of the medial, lateral, femoral trochlea, and patellar compartments. The %HDA in each region was defined as HDA of each divided region by HDA of entire articular surface. In the PF joint, the four divided regions of the femoral trochlea included the medial trochlea (MT), the medial notch (MN), the lateral notch (LN), and the lateral trochlea (LT) (Fig. 1A). The divided regions of the patella included the medial facet (MF), the central ridge (CR), the medial portion of the lateral facet (MLF), and the lateral portion of the lateral facet (LLF) (Fig. 1B). Statistical analysis was made using a paired t test. The significance level was set at p=0.05.
Results:
The mean postoperative functional knee score and Lysholm score significantly improved at the final follow-up (p<0.001 for each) (Table 1). Concerning radiological evaluation, the mean hip-knee-ankle angle (HKA) significantly changed from 6.3° to -1.9° (p<0.001). The mean mechanical axis significantly changed from 74.6% to 42.1% (p<0.001). Regarding the PF joint, there were no significant differences in the Caton-Deschamps ratio between pre- and post-operative periods. The mean radiological Q-angle was significantly decreased from 10.5° to 6.6° (p<0.001). The mean tilting angle was significantly decreased from 7.5° to 5.3° after surgery (p<0.001). The mean lateral shift ratio was significantly decreased from 18.4% to 13.2% (p<0.001). In CT osteoabsroptiometry evaluation, the %HDA in the femoral MT and MN were significantly increased (p<0.005) after surgery. The % HDA in the femoral LN and LT significantly decreased (p<0.015) (Fig. 2). The %HDA in the patellar CR significantly increased (p=0.043) after surgery, and the % HDA in the patellar LLF significantly decreased (p=0.046).
Conclusions:
This study demonstrated that postoperative clinical scores significantly improved after MCW-DFVO. The valgus malalignment significantly corrected to mild varus alignment. In addition, MCW-DFVO led to an altered PF joint congruity. In CT osteoabsorptiometry evaluation, MCW-DFVO shifted the HDA of the lateral compartment of the PF joint toward the medial compartment. These changes in subchondral bone density may result from the change in stress distribution after MCW-DFVO. This study suggested that stress distribution patterns of the PF joints were significantly changed by the MCW-DFVO procedure.