Abstract
Objectives:
Traumatic lateral patellar dislocation is frequently associated with cartilage lesions, particularly of the patella and lateral femoral condyle (LFC). Multiple treatment options to address these chondral lesions including debridement, microfracture, cartilage restoration with allo- or autograft, and osteotomies can be utilized at the index patellar stabilization surgery, or in a staged fashion. However, these additional procedures are not without increased morbidity and long-term benefit has not been well elucidated. In patients with traumatic chondral lesions associated with patellofemoral instability (PFI), meniscal coverage of the lesion and intervention to eliminate further patellar instability may be all that is required for a successful outcome. Thus rendering the increased time, morbidity, and cost of chondral procedures unjustified in this setting. The purpose of this study was to assess outcomes of patients with LFC chondral lesions after traumatic patellar dislocations and whether meniscus coverage of the lesion on magnetic resonance imaging (MRI) has an impact on patient outcomes.
Methods:
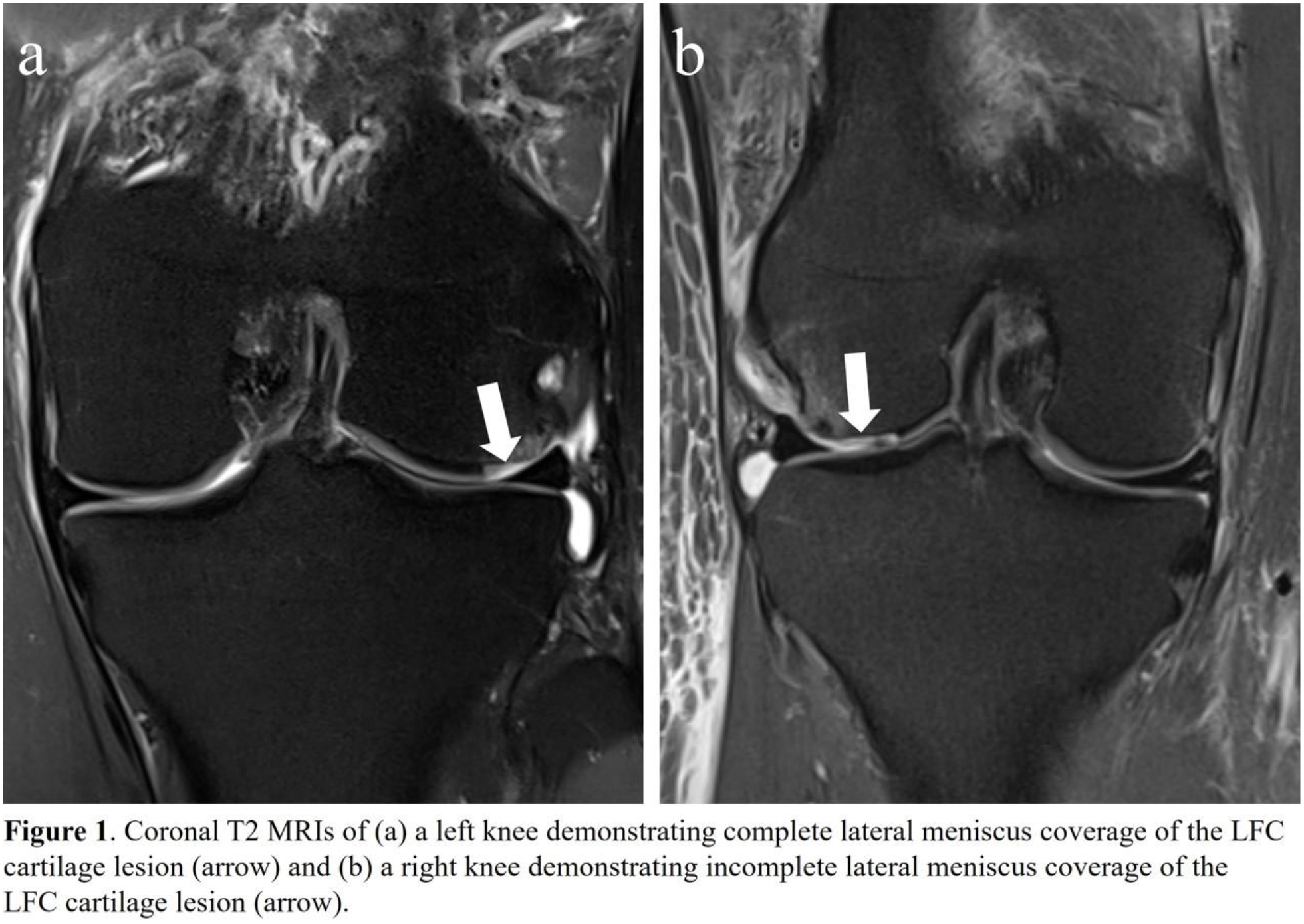
A retrospective chart review was performed to compare outcomes for patients with LFC lesions following acute patellar dislocation treated surgically at a single institution. MRI, operative reports, and intraoperative imaging were reviewed to assess for LFC lesions. Size of the LFC lesion and evaluation of meniscus coverage was measured in the coronal plane on T2 MRI sequences (Figure 1). Patient charts were reviewed to follow postoperative rehabilitation and clinical course. Patient reported outcome measures (PROMs) were obtained using the International Knee Documentation Committee (IKDC) score, Lysholm Knee score, Visual Analog Scale (VAS), and Tegner Activity score.
Results:
A total of 228 patients underwent surgical stabilization for patellar instability from 2001 to 2022, 81 of which had an LFC lesion identified on MRI and confirmed intraoperatively. Seven of these patients underwent a concomitant cartilage restoration procedure (3 internal fixation of osteochondral fragment, 2 microfracture, 1 osteochondral allograft, and 1 MACI) and they were excluded from the study leaving 74 patients. In assessing meniscus coverage of the chondral lesion, 10 of these lesions had no meniscus coverage, 8 had 1-50% coverage, and 56 had 51-100% coverage. The average size of the chondral lesion was 7.1 ± 2.9 mm and the majority were in the anterior one-third of the LFC. Average follow up from the index surgery was 7.6 years (range, 2.2-15.2 years). During this time frame, 12 patients had subsequent knee surgeries, none of which were to address the LFC lesion (Table 2). Postoperatively, nearly all patients reported improvement in their pain with an average VAS pain decrease of 3.7 points. There were no significant differences in PROMs in patients with meniscus coverage versus those without (Table 2). At the time of final follow-up, four patients had radiographic evidence of knee osteoarthritis (OA) within the lateral compartment, and one underwent a total knee arthroplasty (TKA). The patient that underwent a TKA had no meniscal coverage of their chondral lesion at the time of their index procedure.
Conclusions:
Cartilage lesions secondary to traumatic lateral patellar dislocation are common; however, appropriate management of these lesions remains unclear. The present findings suggest that not surgically addressing chondral lesions in patients with overlying meniscus coverage can allow for high functional outcomes and minimal pain after patellar stabilization procedures. Although only four patients progressed to radiographic evidence of OA, long term data will be valuable to understand whether overlying meniscus coverage is also protective against the development of OA and progression to TKA.