Abstract
Objectives:
Operative fixation of pediatric tibial spine avulsion fractures (p-TSF) is traditionally performed using either screws (SCF) or sutures (SF). However, literature lacks comparisons with "hybrid fixations" (HF), which uses sutures and screws. Our study aims to compare these fixation strategies in a large pediatric cohort.
Methods:
A multicenter retrospective study across 10 centers was performed to evaluate operatively treated p-TSF between 2000-2019. Patients with SCF, SF and HF were included in the study with a minimum of 1-year follow-up. Functional outcomes (Range of motion and post-operative laxity) were assessed at the first (1-2 months), interim (3-4 months), and final follow-up. Additionally, complications and return to the operating room (ROR) were also assessed. Bivariate analysis was performed.
Results:
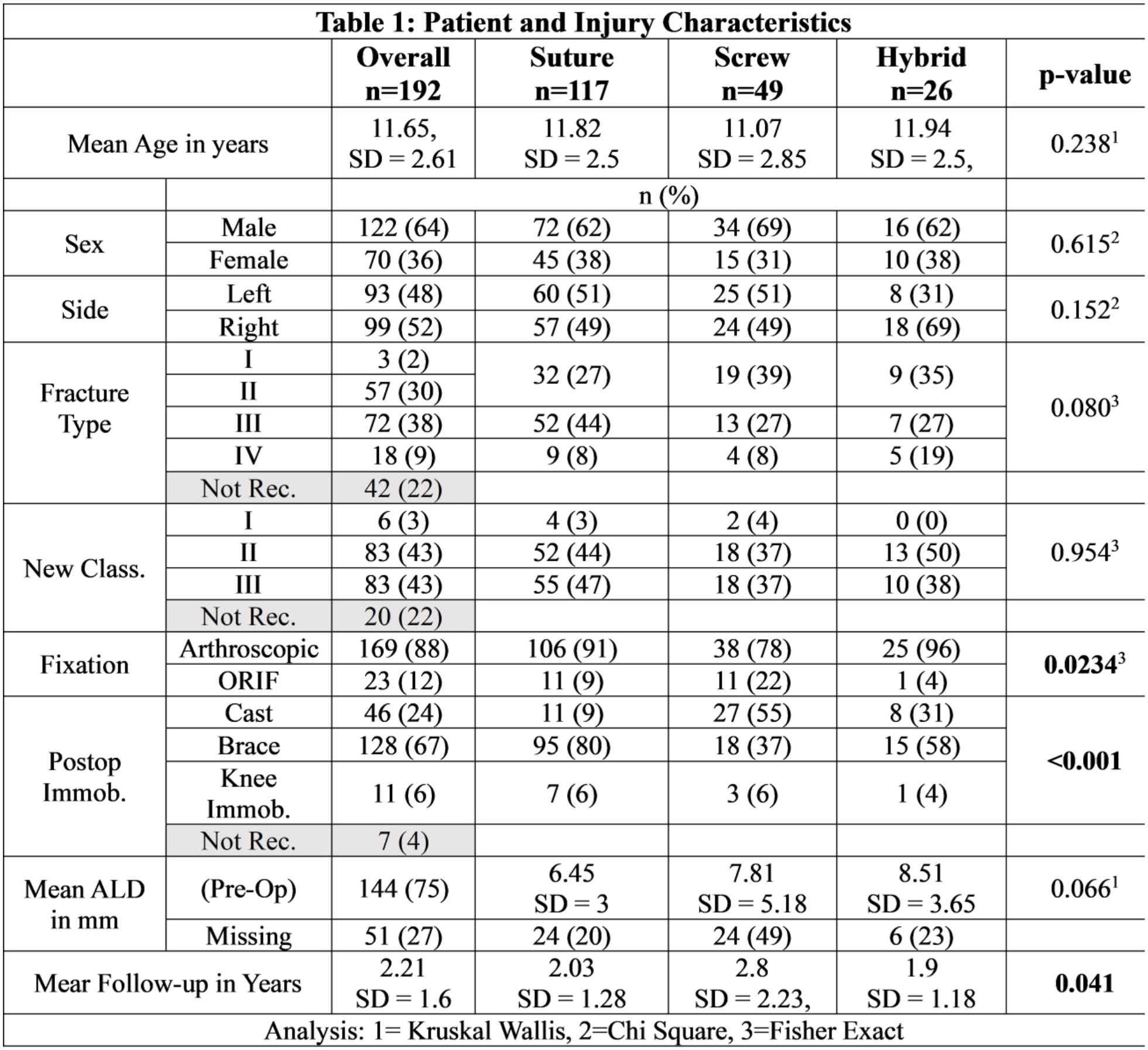
Of the 550 operative patients enrolled, 192 patients were included in the study with 117 SF (60.9%, n=117/192), 49 screw fixations (25.6%, n=49/192), and 26 HF (13.5%, n=26/117). Mean time to the first, interim, and final follow-up were 40.71 ± 12.0 days, 99.8 ± 24.3 days, and 2.21 ± 1.6 years. Groups were similar in regard to age, side, fracture type, and mean pre-op anterior lip displacement (Table 1); however, SCF versus SF and HF underwent open reduction (22% vs. 9.4% and 4%, p=0.023) and post-operative casting (55% vs. 9.4% and 30%, p<0.001) more frequently. HF (110 degrees, 75 – 125) had a greater median flexion compared to SF and SCF (95 degrees, 75 – 120; and 85 degrees, 60 – 90 respectively) at the first visit (p=0.011), while SF (135 degrees, 120 – 140) had a greater median flexion compared to HF and SCF (125 degrees, 110 - 137.5 and 120 degrees, 114.5 – 135 respectively) at the interim follow-up (p=0.017) (Table 2). However, no differences were noted in Laxity, median flexion at final follow-up and with extension at all three time points (p >0.05). The proportion of patients with functional motion was higher with SF (76%) and SCF (70.5%) than with HF (42.8%) at interim follow-up (p<0.008). ROR due to cartilage injury was higher with HF versus SF and SCF (7.6% vs. 0.8% and 0%, p=0.023). Hardware removal was performed at a higher rate with SCF and HF versus SF (40.3% and 34.6% vs 0.8%, p=0.023). Complications and other reasons for ROR were similar (p>0.05).
Conclusions:
This is the first study to examine hybrid fixations with suture and screw fixations, with post-operative outcomes found to be largely similar across all fixation strategies. However, we noted better early flexion recovery with sutures or hybrid fixations, prompting surgeons to consider the slower flexion recovery and need for hardware removal associated with screws.