Abstract
Objectives:
Low complication rates for operative treatment of tibial spine fractures, a relatively rare injury, have been reported in the pediatric population. Previous work has shown the most common complication is arthrofibrosis, which is more common in younger patients and those with concomitant anterior cruciate ligament tears or traumatic injuries. We aimed to identify potential risk factors for unplanned return to the operating room (UP-ROR) after operative treatment of tibial spine fractures in the pediatric population. We anticipate age and concomitant injuries to be risk factors for UP-ROR.
Methods:
Patients treated operatively for tibial spine fractures at a single large pediatric hospital between 2000 and 2024 with a minimum follow-up of 3 months were enrolled. Demographics, injury mechanisms, radiographic factors, concomitant conditions, and UP-ROR details were collected. Radiographic classifications included the Modified Meyers & McKeever, and the New Fracture Classification system: nondisplaced or minimally displaced (< 2mm anterior lip), (>2mm anterior lip displacement and <2mm maximal posterior displacement), (>2mm anterior lip and posterior displacement). For continuous variables, Shapiro Wilk tests and Mann-Whitney and t-tests were used. Chi-square and Fisher’s tests were used for categorical variables.
Results:
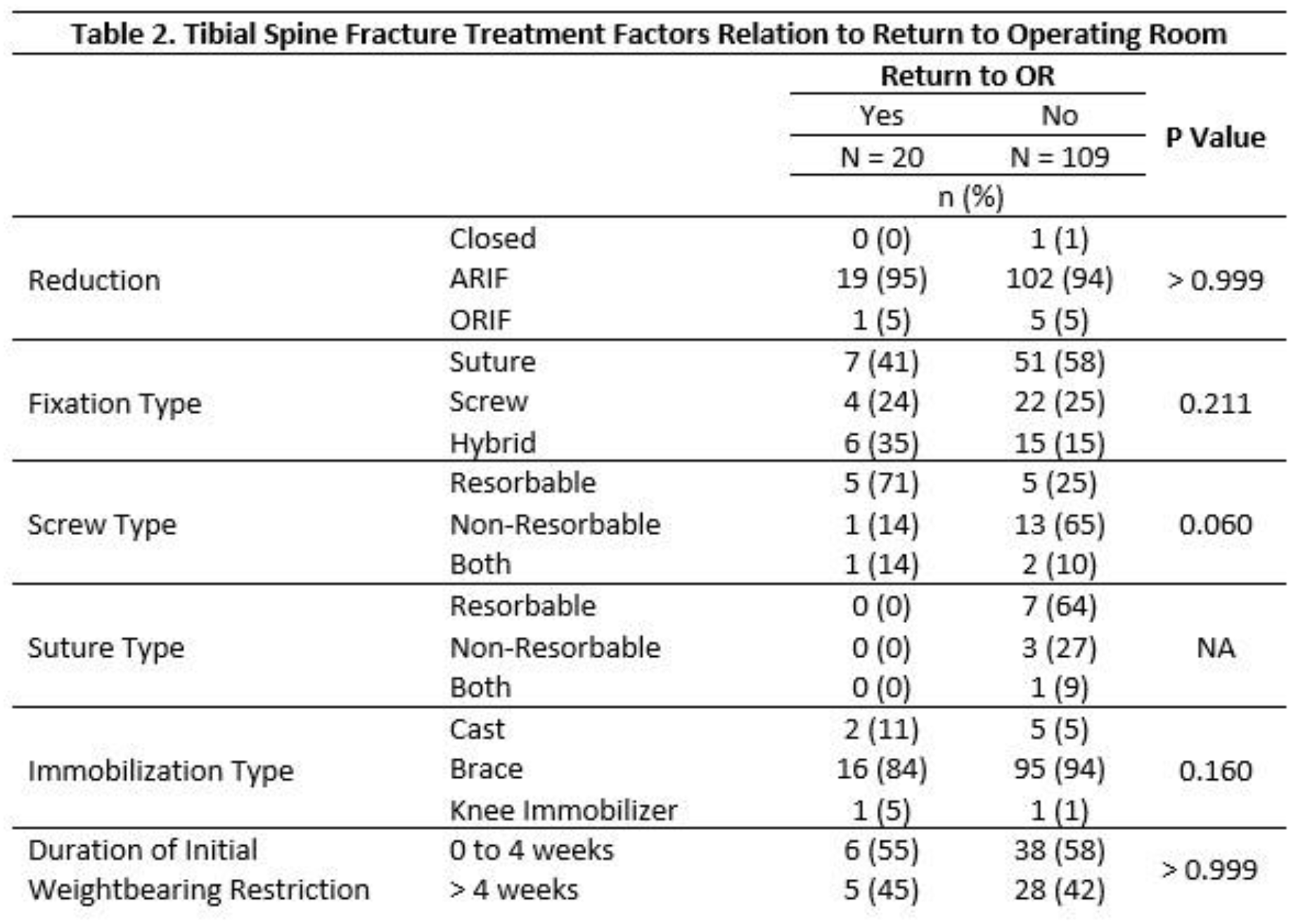
199 patients (61 female) were treated operatively for tibial spine fractures at a single hospital institution. 20 had UP-ROR at an average of 537 ± 626 days after tibial spine fracture surgery. Reasons for UP-ROR included one or a combination of lysis of adhesions and/or manipulation under anesthesia (n=14), new cartilage or meniscal injury (n=13), anterior cruciate ligament reconstruction (n=9), lateral release (n=2), tibial physis fracture (n=1), osteochondritis dissecans (n=2). Upon bivariate testing, post-op ALD (p-0.043) and screw resorbability (p=0.027) were significantly related to UP-ROR. No other patient, injury, or treatment factors were significantly correlated to the need for future operative treatment.
Conclusions:
While age and concomitant anterior cruciate ligament tear have been reported to influence initial risk for tibial spine fractures, as well as postoperative arthrofibrosis, we found that neither factor was significantly correlated with UP-ROR. Early post-op anterior lip displacement is correlated to UP-ROR, emphasizing the importance of reduction of tibial spine fractures. Operative factors, including type of reduction, fixation, and postoperative management were not correlated with UP-ROR. Overall, different operative management techniques of tibial spine fractures in the pediatric population result in similar rates of UP-ROR.