Abstract
Objectives:
The aim of this study was to investigate if unique patterns of knee injury are associated with distinct synovial fluid biomarker profiles at the time of surgical intervention. This knowledge may improve our understanding of underlying pathophysiologic mechanisms and provide information of diagnostic and/or therapeutic significance.
Methods:
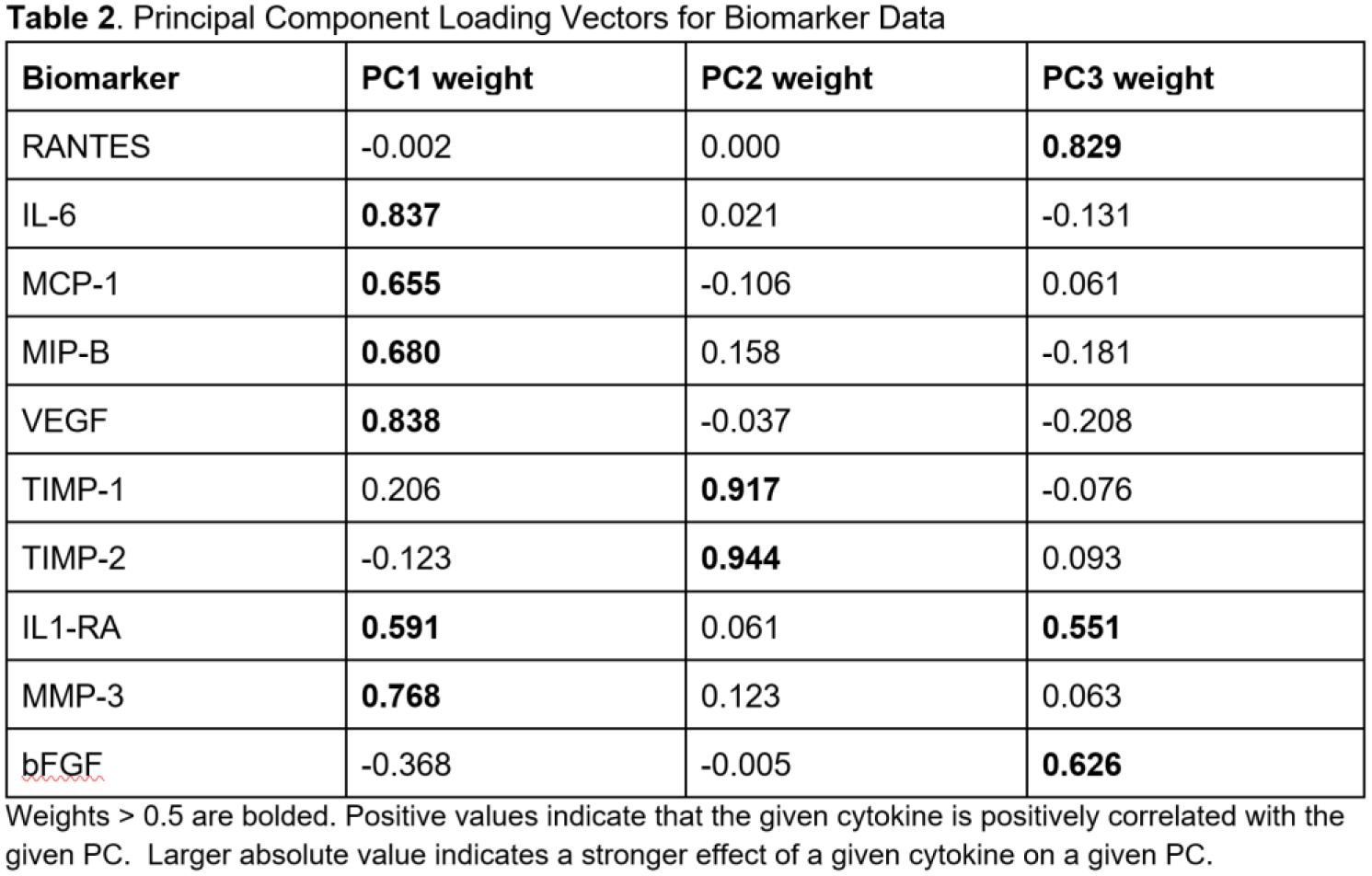
Patients undergoing arthroscopic knee surgery were prospectively enrolled. Synovial fluid was aspirated from the operative knee before surgical incision and the concentrations of 10 biomarkers of interest (RANTES, IL-6, MCP-1, MIP-B, VEGF, TIMP-1, TIMP-2,IL-1RA, MMP-3, and bFGF) were measured by immunoassay. Patients with evidence of injury to articular cartilage, meniscus, and/or ACL were identified and included for subsequent analysis. Biomarker concentrations were log-normalized and standardized by Z-score. Principal component analysis (PCA) was performed using all 10 biomarker variables to reduce dimensionality, address multicollinearity, and extract key patterns. Principal components with eigenvalue > 1 were selected. Multivariable linear regression for each resulting principal component was performed with predictors age, sex, body mass index, smoking status, and injury type.
Results:
A total of 388 patients were included in the analysis, of which 176 (45.4%) had ACL rupture, 325 (83.8%) had meniscal pathology, and 52 (13.4%) had cartilage injury. Other demographic features of the cohort are found in Table 1. PCA yielded 3 principal components (PC1, PC2, PC3) that explained 67.1% of variance in biomarker data (Table 2). PC1 was associated with high loadings (> 0.5) of VEGF, IL6, MMP-3, MIP-B, MCP-1, and IL-1RA; PC2 with TIMP1 and TIMP2; and PC3 with RANTES, bFGF, and IL-1RA. The relative effects and relationships of the PC1 and PC2 are visually represented in a PCA Biplot (Figure 1). Multivariable linear regression found ACL injury (p = 0.033, B = 0.141) and age (p = 0.039, B = 0.135) to be significantly associated with PC1, while cartilage injury alone was associated with PC2 (p < 0.001, B = 0.108). No chosen predictors were associated with PC3.
Conclusions:
ACL rupture and symptomatic cartilage lesions exhibit distinct synovial fluid inflammatory profiles at the time of arthroscopic knee surgery. While ACL injury results in a largely pro-inflammatory phenotype, cartilage injury is associated with an anti-inflammatory, chondroprotective milieu. Understanding the local response to specific knee injuries may help guide a pathology-specific treatment in the effort to prevent the development of post-traumatic osteoarthritis.