Abstract
Objectives:
Medial patellofemoral ligament reconstruction (MPFLR) is a standard treatment for patellofemoral instability (PFI). Concomitant lateral retinacular release (LR) or lengthening (LL) is considered for patients with a tight lateral retinaculum. The purpose of this study was to investigate associations between demographic features, exam findings, and radiologically-measured patellofemoral parameters with LR/LL in patients undergoing primary MPFLR. We hypothesized that greater patellar tilt and lower ligamentous laxity would be associated with the use of LR/LL in conjunction with MPFLR.
Methods:
The Justifying Patellar Instability Treatment by Results (JUPITER) prospective, multicenter database was queried for patients who underwent primary MPFLR from January 2017 to July 2022. Patients with congenital or syndromic instability or habitual or fixed patellar dislocation or who had received a trochleoplasty or distal femoral osteotomy were excluded. Beighton scores of ≥4 were used to denote ‘pathologic’ ligamentous laxity. Binary logistic regressions were performed for multivariable analysis of factors associated with LR/LL and were reported as odds ratios (OR) and 95% confidence intervals (CI).
Results:
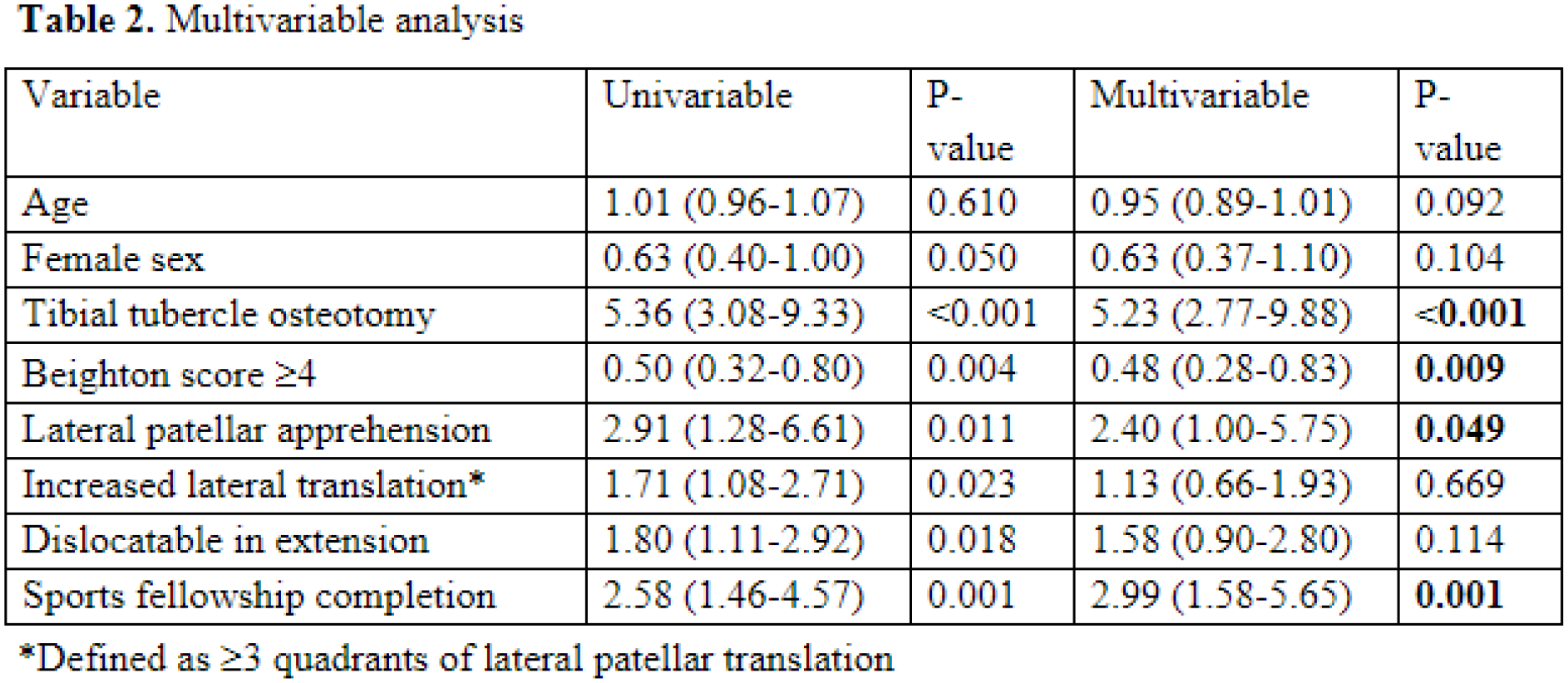
Of 428 patients (mean age: 16.7 ± 4.2 years, 64.5% female, 70.6% skeletally mature, 77.8% recurrent dislocators), 22.9% underwent LR (13.6%) or LL (9.3%). There were no differences in age, BMI, number of pre-operative instability events, or skeletal maturity between LR/LL and non-LR/LL patients. Those who underwent LR/LL were more frequently male (43.9% vs. 33.0%, P=0.049), had lower Beighton scores (2.6 ± 2.7 vs. 3.8 ± 2.9, P<0.001), and their surgeons were more likely to have completed a sports fellowship as opposed to a pediatric fellowship (82.7% vs. 64.8%, P<0.001) (Table 1). On pre-operative exam, LR/LL patients more often exhibited pathologic lateral patellar translation (62.2% vs. 49.1%, P=0.012). Intra-operatively, LR/LL patients more often dislocated in extension during examination under anesthesia (70.4% vs. 57.0%, P=0.017) and underwent a tibial tubercle osteotomy (TTO, 35.7% vs. 9.4%, P<0.001). 168 patients had available pre-operative imaging measurements, with LR/LL patients showing greater patellar tilt (24.1 ± 7.7° vs. 18.5 ± 16.7°, P<0.001). In multivariable analysis, sports fellowship training (2.99 [95% CI 1.58-5.65], P=0.001), and performing of a TTO (OR 5.23 [95% CI 2.77-9.88, P<0.001)]) were associated with LR/LL, while pathologic Beighton scores (OR 0.48 [95% CI 0.28-0.83], P=0.009) were associated with lower likelihood of LR/LL (Table 2).
Conclusions:
Approximately 23% of primary MPFLR patients from a large multicenter cohort underwent LR/LL. LR/LL was associated with less ligamentous laxity, increased patellar tilt, surgeon completion of a sports fellowship, and concomitant TTO. These data may help surgeons understand the relative factors associated with performing LR/LL in patients undergoing primary MPFLR.