Abstract
Objectives:
Hip arthroscopy is a minimally invasive surgical technique that has seen a drastic increase in utilization over the last two decades. Labral tears are one of the most common indications for primary hip arthroscopy. However, up to 15.1% of patients who undergo hip arthroscopy end up requiring a subsequent surgery such as a revision hip arthroscopy. During revision hip arthroscopy, labral pathology is addressed in over 75% of cases with a goal of restoring native anatomy to preserve the hip’s suction seal. One such procedure to restore the native labrum physiology is labral reconstruction. Over the years, an increasing number of labral reconstructions have been performed. As a result, there has been a subsequent increase in the number of labral reconstructions requiring revision surgery. To our knowledge, there exists a paucity of data assessing patient outcomes following a revision labral reconstruction in the setting of a prior labral reconstruction. As a result, the aim of the present study was to report the patient reported outcomes (PROs) of patients who underwent a revision labral reconstruction in the setting of a prior labral reconstruction.
Methods:
A retrospective review of all revision labral reconstruction cases performed by the senior author between 1/1/2010-4/1/2022 was conducted. All revision labral reconstructions performed in the setting of a prior labral reconstruction were identified in the senior author’s post-operative documentation. Patients were included if they were over the age of 18 at the time of follow up, had a revision labral reconstruction in the setting of a prior labral reconstruction and were at least two years out from surgery. Patients were excluded if they had a history of avascular necrosis, Legg-Calve Perthes, or significant acetabular dysplasia (LCEA <20). Patient demographics, radiographic parameters, and patient reported outcomes (PROs)—including 12-Item Short Form Survey Physical Component Score (SF-12 PCS), 12-Item Short Form Survey Mental Component Score (SF-12 MCS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), modified Harris Hip Score (mHHS), Vail Hip Score (VHS), Hip Outcome Score – Activities of Daily Living (HOS-ADL), and Hip Outcome Score – Sport (HOS-Sport)—were collected pre- and minimum 24 months postoperatively.
Results:
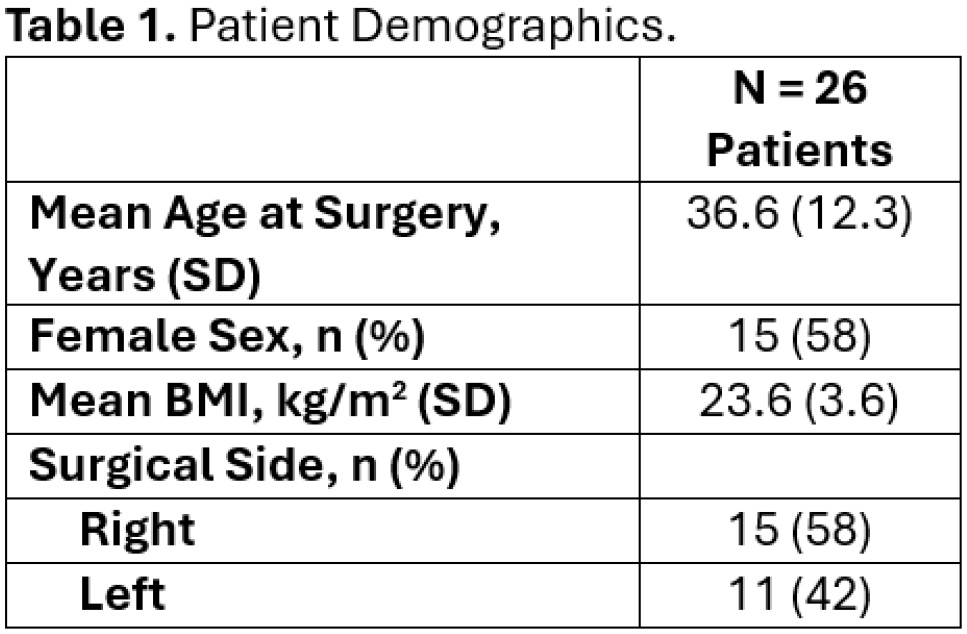
A total of 26 patients who underwent revision labral reconstruction in the setting of a prior labral reconstruction were identified and included in the study. The mean age at the time of surgery was 36.6 ± 12.3 years, and most of the patients were female (n=15, 58%), see Table 1. Twenty-one (81%) of patients completed follow up at a mean of 2.6 ± 0.6 years. Five patients had a subsequent surgery, including 4 conversions to total hip arthroplasty and 1 hip resurfacing procedure. The remaining 16 patients demonstrated significant improvement from baseline in SF-12 PCS, WOMAC Total, mHHS, VHS, HOS ADL, and HOS Sport (p<0.05), see Table 2. However, there was no significant improvement from baseline in SF-12 MCS.
Conclusions:
Patients who undergo revision labral reconstruction in the setting of a prior labral reconstruction demonstrate significant improvement in PROs post-operatively compared to baseline. To our knowledge, the present study is the first to report on outcomes in this population, and the demonstrated results suggest a revision labral reconstruction is a viable option for patients wishing to avoid conversion to total hip arthroplasty. Next steps are to match our cohort to a cohort of primary labral reconstruction patients. This will allow for optimal clinical decision making and aid surgeons in better managing patient expectations.