Abstract
Objectives:
Lateral hip pain may result from bursitis, tendinitis, and partial or complete abductor tendon tears. Evaluation frequently results in expensive advanced imaging, including MRI, to differentiate among these diagnoses. While advanced imaging can confirm a diagnosis, its use for all patients with lateral hip pain is expensive, logistically burdensome, and may expose patients to ionizing radiation. Consequently, reliable clinical exam maneuvers are needed to help differentiate true hip abductor tears from GTPS.
The Hip Drop Test (HDT) is a clinical hip exam maneuver which can help differentiate the etiologies of lateral hip pain. It is performed as follows: patient lies on the asymptomatic side, with the symptomatic hip oriented upwards. The examiner will instruct the patient to flex the symptomatic knee to 90o. Then, the examiner will place the patient’s hip in 10o of extension and 20o of abduction. From that position, the examiner will maximally internally rotate the hip. After achieving maximum internal rotation, the patient will be instructed to retain this position as the examiner releases the extremity. Inability to retain that position, as well as a depression of the foot by
The aim of our study was (1) to assess the diagnostic utility of the HDT to correctly identify MRI-confirmed gluteus medius/minimus tears, and (2) assess the HDT’s ability to predict the likelihood of future surgery. We hypothesized that the HDT will have high sensitivity and specificity for diagnosis with lower utility for predicting future surgery.
Methods:
We retrospectively reviewed a single institution’s electronic medical record database from 2020-2024, comprised of a single fellowship-trained sports surgeon’s patients. Patients ≥18 years old with clinically suspected hip abductor tears that were examined with the HDT and received a subsequent hip MRI were included. Documented clinical exam results were compared to MRI reports dictated by fellowship-trained musculoskeletal radiologists. The presence of a positive HDT and full or partial MRI-confirmed hip abductor tendon tear was further evaluated for surgical intervention. Statistical evaluation was performed by the Study Design and Biostatistics Center at the University of Utah.
Results:
Our initial retrospective review yielded 366 patients. Of those, 345 were negative for the HDT while 17 were positive. 8 of the HDT positive patients underwent surgery, and 75 of the HDT negative patients underwent surgery. The HDT was significantly correlated with increased age (p < 0.001), a lower initial SANE score (p = 0.007), the need for future surgical intervention (p = 0.034), the presence of an HA tear on MRI (p < 0.001), and presence of a full thickness tear (p < 0.001).
HDT and MRI:
Sensitivity was calculated to be 87.5% (95% CI: 64.0%-96.5%). Specificity was calculated to be 87.1% (95% Confidence Interval [CI]: 82.4%-90.7%). Positive predictive value (PPV) and negative predictive value (NPV) were calculated to be 30.4%; (95% CI: 19.1%-44.8%) and 99.1% (95% CI: 96.7%-99.7%) respectively. Logistic regression analysis demonstrated multiple factors associated with true hip abductor tears.
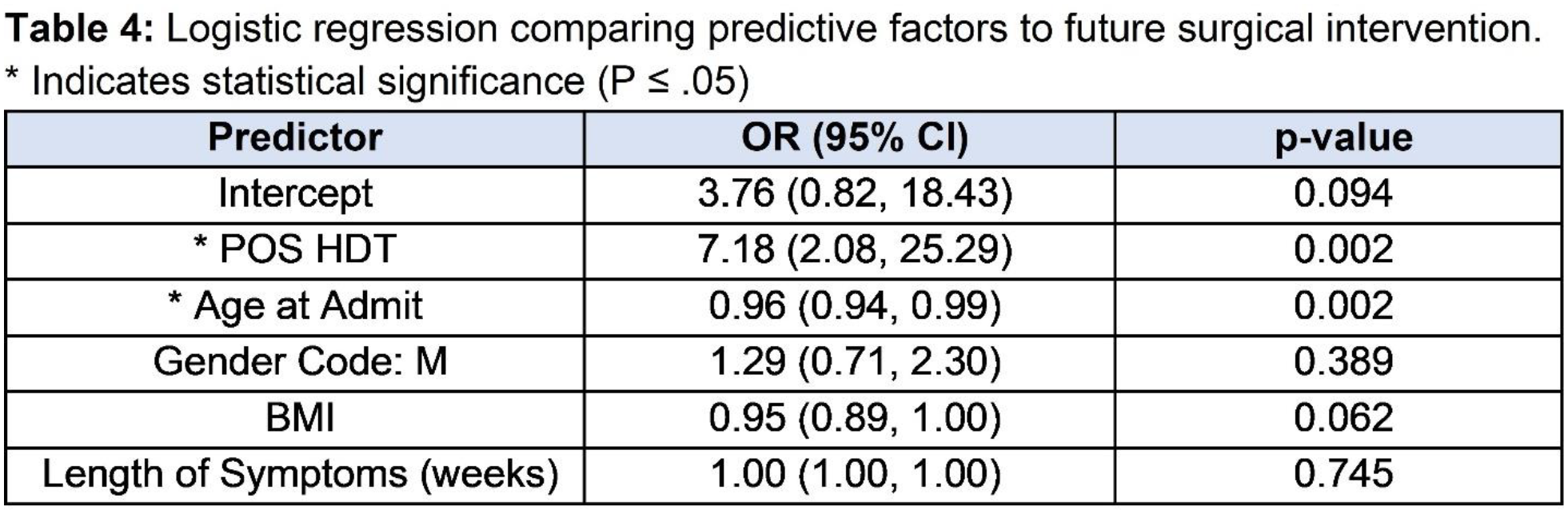
HDT and Surgery:
The sensitivity and specificity of the HDT with regard to later surgery was 47.1% (95% CI: 26.2%-69.0%) and 77.7% (95% CI: 73%-81.9%) respectively. The PPV and NPV were calculated to be 9.6% (95% CI: 5%-17.9% and 96.7% (95% CI: 93.8%-98.2%), respectively. Regarding surgical intervention, logistic regression predicts that positive HDT (OR: 7.18; 95% CI: 2.08-25.29); (p = 0.002) and increased age (OR: 0.96; 95% CI: 0.94-0.99); (p = 0.002) as significant.
Conclusions:
We hypothesized that the HDT would have an adequate level of sensitivity, specificity, PPV, and NPV in identifying MRI-confirmed tears of hip abductors with more limited ability to predict future surgical intervention. Our results demonstrate the HDT has relatively high sensitivity (87.5%) and specificity (87.1%), a low PPV (30.4%), and a remarkably high NPV (99.1%) for diagnosing hip abductor tears. The sensitivity, specificity, and PPV of the hip drop sign relative to predicting surgery are lower; however, the NPV remains remarkably high at 96.7%. A positive HDT was positively correlated with increased age, lower initial SANE score, need for future surgical intervention, presence of an abductor tear, and full-thickness tears. There were no significant differences between the HDT positive group and the HDT negative groups based on height, weight, BMI, gender, laterality, length of symptoms, final SANE score, or the use of MRI imaging. Our study was somewhat limited in that it was a retrospective analysis from a single hip preservation surgeon at a large urban referral center, which may limit control of biases and generalizability of findings. However, data were prospectively collected, and study design mitigated other biases. In summary, the HDT is a reliable exam maneuver for diagnosing hip abductor tears in lateral hip pain patients with high sensitivity, specificity, and NPV. We believe the HDT may be used to guide the initial treatment of patients with lateral hip pain, and patients with a negative Hip Drop Test may forego immediate advanced imaging.