Abstract
Objectives:
Focal cartilage lesions or osteochondral defects, most commonly observed in the knee, are also found in the hip, elbow, and ankle. Osteochondral autograft transplantation (OAT) and osteochondral allograft transplantation (OCA) are two viable surgical tissue transfer options, that often rely on press-fit graft fixation for cartilage restoration. Symptomatic lesions can occur on the peripheral aspects of a joint surface where there is loss of bone containment and as a result, graft stability could be compromised. This study attempts to understand properties of uncontained osteochondral lesions and identify factors affecting stability of an osteochondral graft.
Biomechanical study and analysis of skeletal reconstruction for cartilage restoration procedures should include properties of the joint, characteristics of host cartilage, bone, and donor tissue, graft and lesion sizes, and the nature of graft fixation. Current orthopaedic literature is without study of press-fit osteochondral transplant in sites with a loss of native bone containment. We thus hypothesized that stability of a graft would be affected by decreasing levels of bone containment at its recipient site; and that the peak tensile force to failure, defined as pull out or loosening of a press-fit osteochondral allograft plug, would decrease significantly at a specific threshold of containment.
Our analysis aimed to identify the optimal levels of lesion containment, and which characteristics determine stability of standard press-fit graft. This information may be useful to surgeons in decision making during OAT and OCA procedures, and determining when supplemental graft fixation or alternative treatments should be considered for these challenging defects.
Methods:
This study utilized 14 cadaveric distal femurs, and 5 osteochondral allograft plugs obtained from each specimen - 70 total allografts. Dual-energy X-ray absorptiometry (DEXA) scans were performed on each intact distal femur to determine subchondral bone mineral density (BMD) of five regions of interest (ROI), including the entire distal femur, medial condyle, lateral condyle, posterior condyles, trochlea, and individual plugs.
Using a single-use osteochondral autograft transplant system, osteochondral grafts were extracted from the medial or lateral trochlea as a cylindrical plug, to a size of 10 mm diameter by 10 mm depth. Five recipient sites were prepared on the medial and lateral femoral condyle and randomly assigned to simulate five different levels of bone containment: 100%, 90%, 80%, 70% and 60% contained (0% bone loss to 40% bone loss). The measured circumference for resection from each site was templated in 10% intervals, with the cartilage, cortical and cancellous bone removed from its wall in a peripherally directed fashion. The grafts were fixed to a suture passed through a central drill hole and a 2mm x 2mm steel plate at its base, in preparation for pull out testing. Using a standard surgical press-fit technique, the grafts were inserted coaxially into each recipient site and gently tamped to a level flush with the surrounding cartilage surface anatomy.
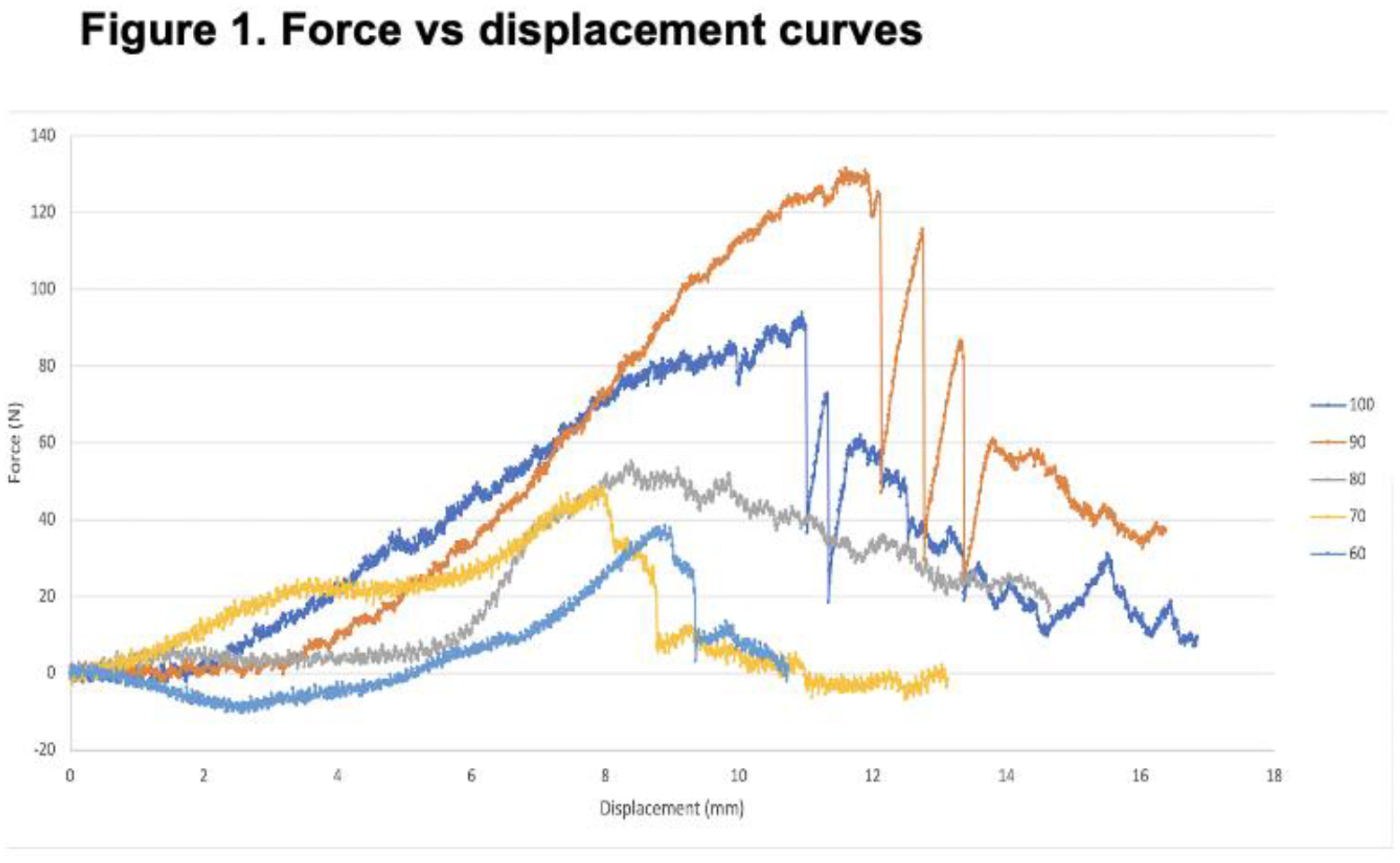
Tensile testing was performed using the MTS 858 Bionix testing system. A load perpendicular to the articular surface was applied at a rate of 0.20 mm/second, and force-displacement curves were generated to determine the tensile pull-out force (Newtons), required to remove or loosen the graft from its implanted site. Comparisons between anatomic and biomechanical data were made utilizing One-Way Analysis of Variance and post-hoc analysis via Tukey’s method to test for group comparisons. Significance level was set at alpha < 0.05.
Results:
The mean tensile force to failure of each graft, was higher at increased levels of lesion containment, and a significant difference was seen across all five levels of containment, 100-60% contained (P<.05).
Post-hoc analysis revealed significant differences between the mean forces at both 60 and 70% containment, when compared to 100% containment. No such difference was found between 80 or 90% containment, when compared to 100%, indicating a statistically significant threshold of 80% containment.
There were no significant differences in the dimensional characteristics or BMDs of corresponding ROIs across specimens. BMD of osteochondral grafts and recipient sites from the trochlea, medial and lateral femoral condyles, was similar.
Conclusions:
Our findings indicate that greater containment of a graft within its recipient site positively influences graft stability after transplantation, and suggests a critical threshold of 80% bone containment or greater for improved stability of a 10mm x 10mm press-fit osteochondral allograft.
This provides insight into containment level influencing the biomechanical stability of osteochondral grafts and the existence of a containment threshold for optimal graft stability. Likewise, may be valuable to surgeons when considering press-fit fixation during osteochondral grafting procedures. Future biomechanical research could extend these findings, and further in-vivo studies may validate the identified containment threshold, and its impact on graft failure versus successful incorporation. Ultimately, helping to develop techniques ensuring successful outcomes for patients undergoing OCA or OAT for articular cartilage restoration.