Abstract
Objectives:
Iliotibial band (ITB) grafts provide excellent anterior cruciate ligament reconstruction (ACLR) outcomes in skeletally immature patients, but graft harvest is associated with symptomatic muscle herniation in some. Closure of the ITB harvest interval is not an option in most, so approaches to harvesting a smaller ITB graft may be desirable. The purpose of this study is to compare ITB autograft length for 2 different procedures: 1. the Micheli over the top graft passage, and 2. the all-epiphyseal femoral drill hole graft passage. We hypothesize that the all-epiphyseal femur ITB graft will be significantly shorter than the over-the-top ITB graft.
Methods:
Six pediatric knees (mean age 9.7 years, range, 9 to 11) were utilized. Surgeons performed simulated Micheli and all-epiphyseal ITB ACLRs referencing anatomical landmarks, using number 2 suture as a proxy for ITB graft. A suture was attached at the ITB origin on Gerdy’s tubercle, and then passed over-the-top on the femur, over the front of the tibia, under the transverse meniscal ligament, and to the metaphyseal attachment anchor point. The length of the suture was measured. The suture was then placed through the all-epiphyseal femoral drill hole, through the joint, to the same tibial metaphyseal anchor point. Femoral condyle width was recorded. Statistical analysis was done using an analysis of covariance (ANCOVA) to account for femoral condyle widths.
Results:
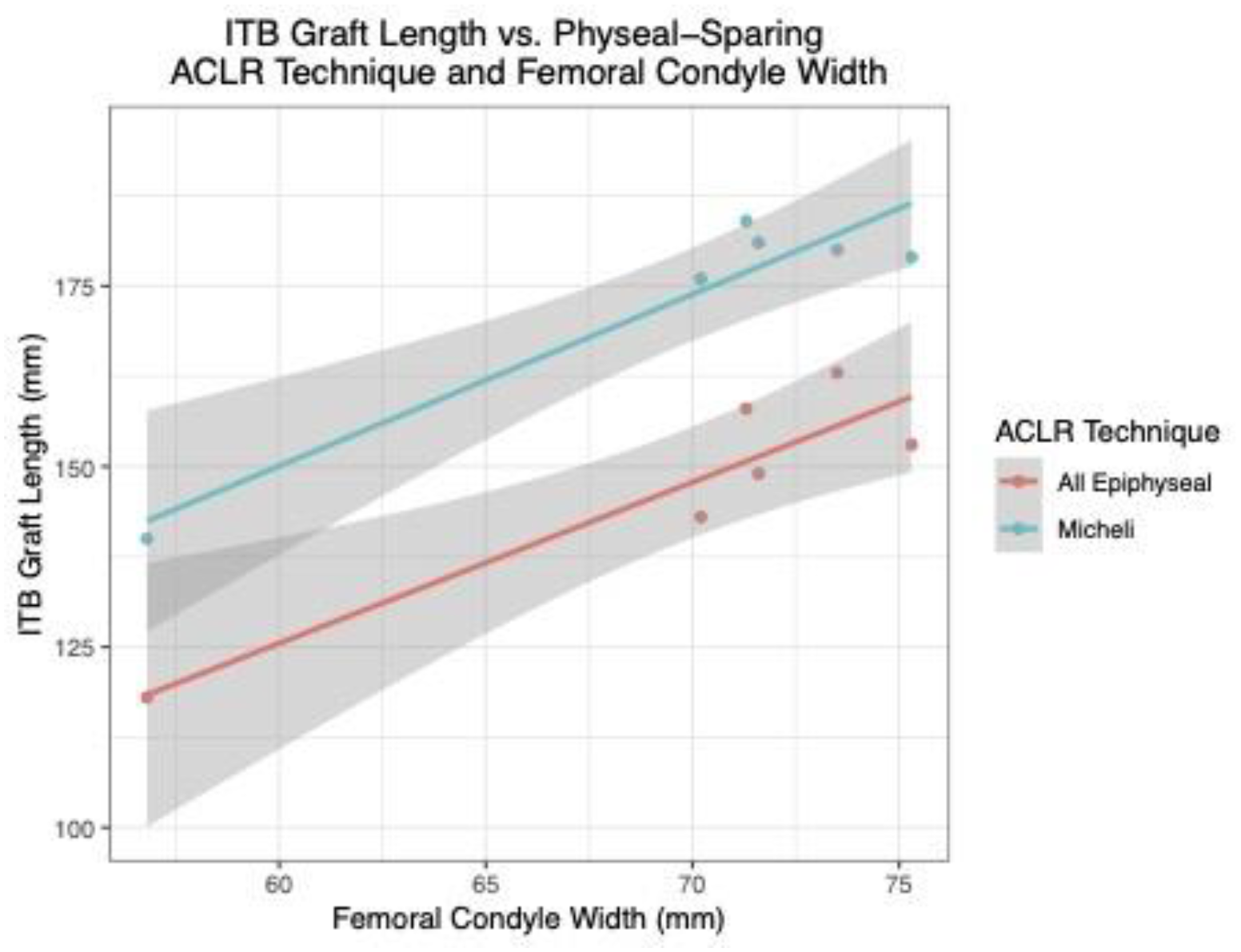
Graft length for the all epiphyseal ITB ACLR was significantly shorter than the Micheli ITB ACLR, with a mean difference of 26.0mm ± 6.0 (p<.001). Each additional millimeter of condyle width was associated with an increase in graft length by 2.3mm (p<.001). The mean graft lengths for the Micheli and all-epiphyseal femur were 173.3mm ± 16.5 and 147.3mm ± 16.0, respectively.
Conclusions:
This study found that the all-epiphyseal ITB technique requires a significantly shorter graft length compared to the Micheli ITB technique, and a nomogram was developed to estimate differences in graft length adjusted for condyle widths. Whether this shorter graft length has a significant impact on vastus muscle herniation is unclear, as these graft length differences appear to be relatively small. Future pediatric studies on the biomechanics of the over the top versus femoral tunnel graft passage should continue, as both graft techniques provide for a lateral extra-articular stabilization, which may reduce ACL re-injury rates.