Abstract
Objectives:
Recent trends in operative management are noted for medial epicondyle fractures, however, data from a large prospective multicenter cohort is still sparse. The objective of our study is to report on demographics, baseline characteristics, current treatment patterns, and early outcomes among operatively treated medial epicondyle fractures from the MEMO prospective study cohort. We hypothesized that while variability would exist, trends would emerge regarding demographics, injury characteristics, and treatment techniques of medial epicondyle fractures, while certain variables would affect range-of-motion (ROM) and return-to-sport (RTS).
Methods:
Patients 8-18 years old who underwent open reduction internal fixation of medial epicondyle fractures with displacement ≥3mm were identified from the operative arm of the prospective multicenter database established by the MEMO study group from 10 large pediatric hospitals. Demographic, injury, surgical characteristics and early clinical outcomes (including ROM and RTS) were recorded and analyzed, examining outcome variables in relation to patient demographics and injury characteristics. Baseline and demographic characteristics were summarized by standard descriptive summaries, and data were analyzed using Chi-squared and Mann–Whitney U tests where applicable.
Results:
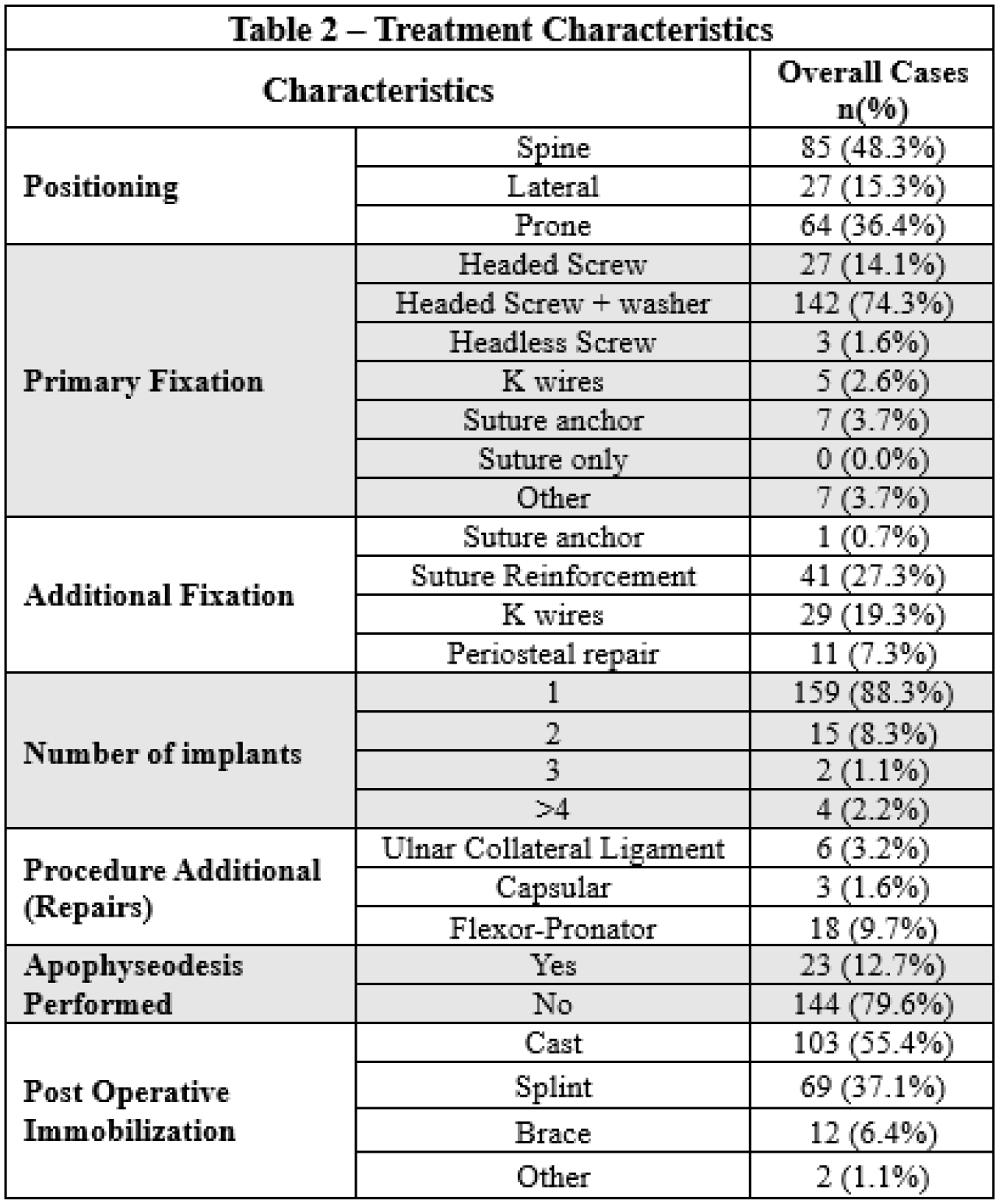
186 patients (56.8% male) were included with mean age of 12.8±2.1 years. 68.7% of injuries occurred while playing sports (baseball/softball>gymnastics>football). The dominant arm was affected in 48% of patients. 43.0% of injuries occurred in overhead athletes, and 27.5% occurred while throwing. 8.2% of fractures were associated with a dislocation and 3.8% with an ulnar nerve deficit. Single large fragment was the most common fracture pattern (89.5%) followed by an avulsion of only a small component (6.1%) (Table 1). Mean displacement on radiographs and CT scans was 11.4±4.8mm and 10.9±4.2mm, respectively. Fixation was preferred in the supine position (45.7%) and performed most commonly using a headed screw+washer (76.3%) followed by a headed screw (14.5%). Additional fixation was commonly achieved using suture reinforcement (27.3%). Long arm cast was the preferred post-operative immobilization method (55.4%) followed by splint (37.1%) and brace (6.4%) (Table 2). By the 3-month visit, patients lacked a mean of 6.2° (±16.5) extension and achieved 133.1° (±16.2) flexion, and 48.3% of patients were cleared for RTS. While RTS was not significantly affected by concomitant elbow dislocation, hand dominance, or when comparing overhead vs. non-overhead athletes, decreased ROM was found to be related to patients sustaining a concomitant elbow dislocation.
Conclusions:
Medial epicondyle fractures commonly occur in isolation with a low incidence of ulnar nerve injury. Fixation is commonly in the supine position using a screw+washer and immobilized in a cast post-operatively. 3-month range-of-motion outcomes are affected by concomitant elbow dislocations, while RTS is not. Our study presents the current operative trends of medial epicondyle fractures in a large cohort further allowing for evaluation of optimal treatment methods and associated patient-reported outcomes.