Abstract
Objectives:
In the pediatric population, the primary goal of the patient after a musculoskeletal injury is often return to activity, either recreational play or organized sports. Despite this, even for the most common upper extremity fracture patterns, there is little to no standard of practice in the literature for activity clearance by the treating provider after non-operative treatment. The aim of this study is to identify variation and establish national trends in timing of return to sport clearance after upper extremity fracture to guide standard of care.
Methods:
A survey was distributed electronically to the membership body of the Pediatric Orthopaedic Society of North America (POSNA) with four clinical scenarios depicting UE fractures: distal radius (DR) fracture, buckle and complete, and both bone forearm (BBFA) fracture, pediatric and adolescent. Respondents were queried about the time after fracture at which they would allow the patient RTP clearance for non-contact, contact, and upper extremity weightbearing sports.
Results:
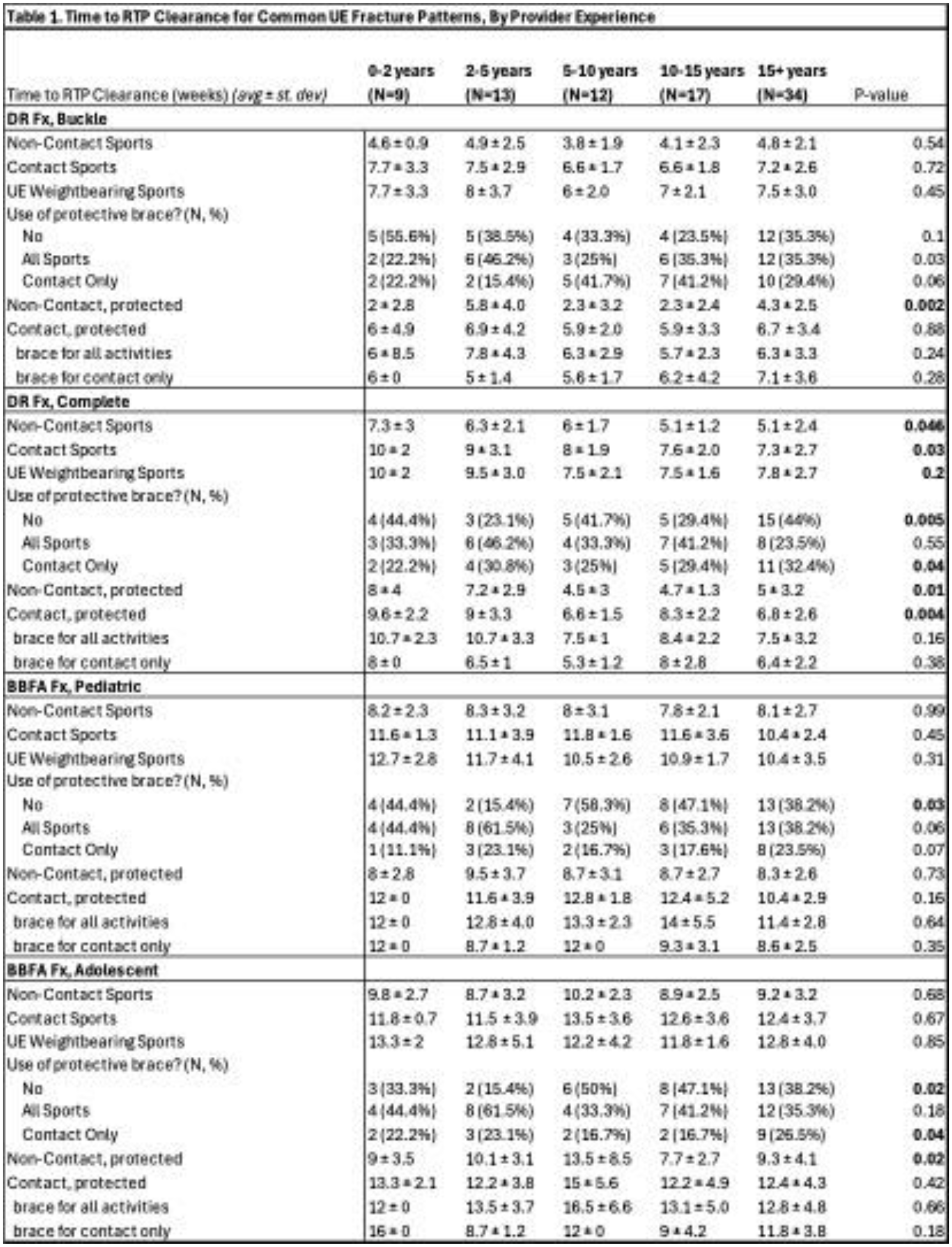
A total of 85 POSNA members completed the survey (approximately 6% response rate). For each fracture pattern, mean RTP clearance times increased with increasing activity level (Figure 1). RTP time for contact activity in a brace was longer when the brace was recommended for use with all activities versus when recommended just for contact.
In treatment of complete DR fractures, clearance for non-contact sports averaged 5-7 weeks from injury, and contact sports between 6-9 weeks from injury. For BBFA fractures, patients were returned to non-contact activities between 6 and 9 weeks after injury and to contact sports between 10 and 14 weeks after injury (Figure 1). Increasing years of experience was associated with shorter RTP clearance after complete DR fracture for all activities and with decreased use of protective bracing for all fracture patterns (Table 1).
Comparing sports fellowship training to those without, there was no difference in overall RTP timeline or use of bracing for any fracture pattern (Table 2). Sports fellowship training was associated with longer RTP clearance with brace protection for contact activity after DR fracture and non-contact activity after pediatric BBFA fracture.
Conclusions:
Understanding national trends in timing of return to sport clearance after common pediatric and adolescent upper extremity fractures can guide standard of care. Patients with DR fractures were cleared for return to sport earlier than those with BBFA fractures and physician experience was associated with shorter time to return and less use of a protective brace. Trends demonstrate increasing time of restriction based on fracture type and pattern, as well as demand of activity participation. Variability amongst treating clinicians based on years of experience and type of fellowship training most notably exists in the application of bracing as it relates to RTP clearance, a subject which warrants further investigation.