Abstract
Objectives:
Most current classification systems and treatment algorithms for medial epicondyle (ME) fractures assume that both the medial ulnar collateral ligament (UCL) and flexor pronator mass (FPM) are attached to the ME fragment and thus that the anatomy of the medial elbow can be restored with reduction of the bony fragment. We hypothesized that separate attachments of the UCL and FPM may produce injury patterns where the UCL and FPM attachments are not avulsed together. This study aims to identify these previously unrecognized fracture patterns.
Methods:
A retrospective review of patients <18 years was performed. Patients presenting with radiographs and MRI Imaging within 6 weeks from injury were screened for a bony medial epicondyle elbow injury. Patients with only a soft tissue injury to the medial elbow were excluded. Data collected included age, gender, mechanism, lateral side injury, dislocation. Descriptive statistical analysis was performed.
Results:
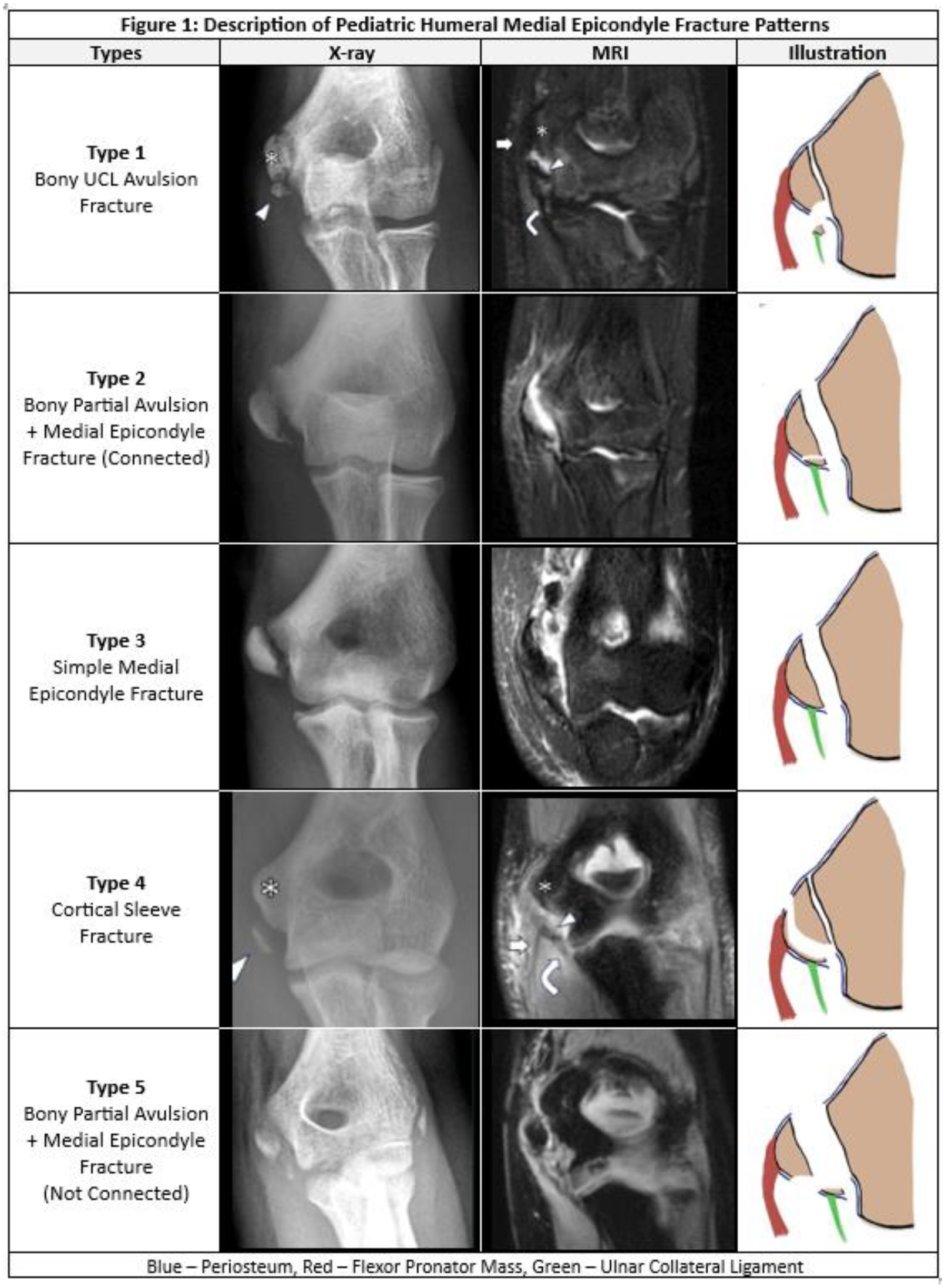
55 patients with mean age of 12.45 years (SD: 2.83) were identified. Five distinct fracture patterns were identified – Type 1: A well-corticated fragment attached to the UCL off the inferior pole of the ME, Type 2: A combination of Type 1 and ME where the fracture fragments are still connected through soft tissue attachments as a single unit, Type 3: A ME fracture through the physis with both the UCL&FPM attached to one large fragment, Type 4: A well-defined cortical sleeve/shell-like fragment off the inferomedial aspect of the ME with the main ME physis intact and both the UCL&FPM attached, Type 5: A combination of Type 1 and ME with two separate unconnected fragments. Age distribution was similar across all types, except for Type 5 which had younger patients (p=0.048) while gender was not significant (p=0.083). Type 1 and Type 2 injuries were associated with a throwing mechanism, while Type 3, 4 and 5 occurred following more traumatic injuries like a fall or during gymnastics/wrestling (p=0.005). Type 4 and Type 5 injuries more often had lateral elbow injuries (p=0.019), as well as dislocations (p=0.003).
Conclusions:
Five distinct medial epicondyle fracture patterns were found which variably involved displacement of the ME fragment attached the either UCL or FPM or both. As the treatment rationale for ME injuries is often predicated on restoring elbow biomechanics through anatomical restoration of the UCL, identification of these injury patterns is potentially a key first step in understanding the variability in clinical outcomes with different management strategies for medial elbow injuries.