Abstract
Objectives:
Background: Olecranon stress fracture (OSF) is a pitching-related injury with an incidence rate of 5.4% among baseball elbow injuries. In a previous report, we classified OSF into five types (Furushima classification) and investigated its mechanism of onset, concluding that elbow valgus stress is involved. Since then, there have been no new studies on the mechanism, and only a few reports have detailed surgical methods using screw fixation, with no comprehensive analysis of surgical outcomes. OSF often presents as a nonunion, leading to calcification and bone sclerosis at the fracture site. This complicates the freshening of the sclerotic fracture site, making bone union difficult to achieve with screw compression alone. We have encountered cases where patients were referred to our hospital due to poor bone union following DTJ screw fixation at other facilities. As such, OSF remains challenging to treat, and there is currently no consensus on the optimal treatment approach. We have consistently treated OSF by inserting a bone peg into the nonunion site to facilitate fracture healing, achieving very good results. To evaluate the clinical outcomes of OSF in baseball players who underwent surgical treatment, categorized by fracture type according to the Furushima classification, and to report on the surgical techniques and outcomes associated with each OSF type.
Methods:
This study included 147 cases out of 171 male baseball players (mean age, 17.0 years; age range, 14–23 years) who underwent surgery for olecranon stress fractures or olecranon epiphyseal separation between 1992 and 2022, and were followed for more than one year postoperatively. Postoperative evaluation was conducted using the Conway-Jobe scale. Patients with olecranon osteophyte disorders and thoracic outlet syndrome were excluded. Surgical candidates were those who had persistent pain for more than three months with no evidence of bone union.
Results:
The OSF cases were classified as Physeal type (62 cases), Classical type (57 cases), Transitional type (21 cases), Sclerotic type (6 cases), and Distal type (11 cases). Surgical methods included inverted bone graft with TBW (62 cases), bone peg graft (78 cases), DTJ (6 cases), and drilling (1 case). According to the Conway-Jobe scale, 90.5% of cases achieved excellent or good outcomes, indicating very favorable postoperative results.
Conclusions:
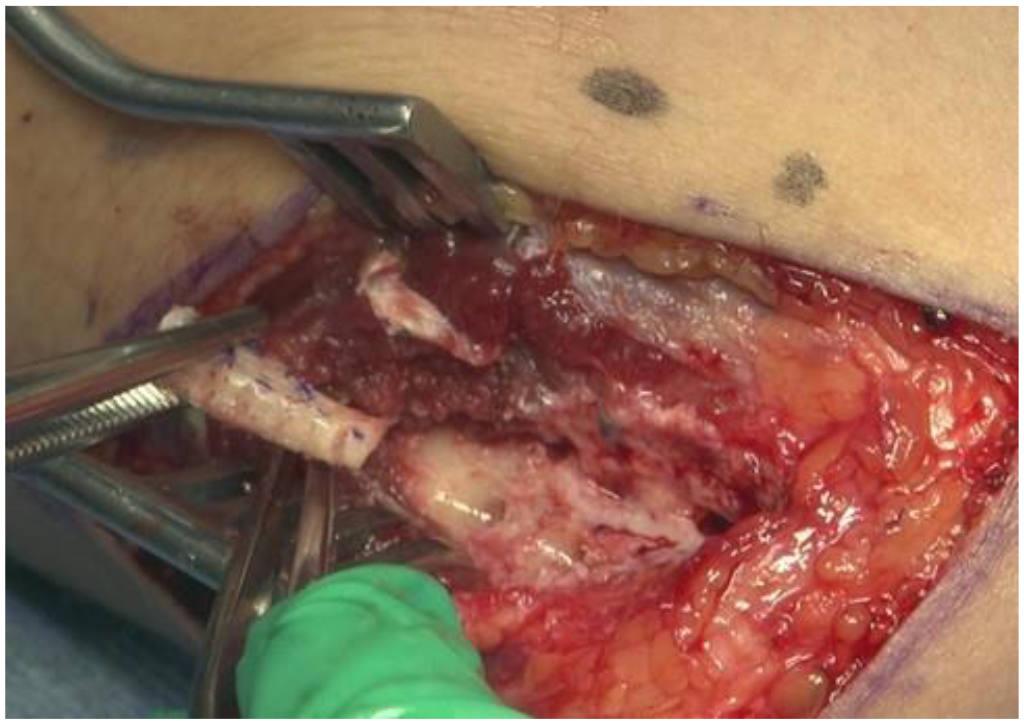
In OSF surgery, we consistently use bone pegs and tailor the surgical method based on the fracture type. In cases of olecranon epiphyseal separation, we perform inverted bone grafting. We ensure that the bone peg is inserted perpendicular to the fracture line, with specific techniques depending on the fracture type: insertion from the ulnar bone peg harvest site for the Transitional type, and from the proximal ulnar side of the olecranon and the proximal ulna for the Classical and Distal types, respectively. Additionally, we use a 4.5 mm thick bone peg to maximize the contact area at the nonunion site and further promote bone union. In conclusion, we achieved excellent results in 90.5% of cases, demonstrating that OSF treatment using bone pegs is highly effective.