Abstract
Objectives:
Anterior instability is the most common type of shoulder instability, comprising 80% of all instability in young athletes. The classic injury pattern seen in the setting of anterior instability is a Bankart lesion, which is a tear of the anteroinferior glenoid labrum with disruption of the scapular periosteum. However, there are other variants of the Bankart lesion that have the potential to influence clinical outcomes and surgical management, including glenolabral articular disruption (GLAD) lesions. GLAD lesions are defined as concomitant tears of the anteroinferior labrum and adjacent articular cartilage, and are estimated to occur in 1.5 – 3% of traumatic labral tear cases. Given their relative rarity, there is limited literature of the long-term prognosis of such injuries and whether these lesions increase the risk of failure following arthroscopic Bankart repair. The aim of this study was to compare clinical outcomes of patients with and without GLAD lesions in the setting of first-time anterior instability events. A secondary aim was to determine the rates of recurrent instability following surgical stabilization in both groups. We hypothesized those with GLAD lesions would exhibit worse range of motion (ROM) and patient-reported outcomes (PROs) postoperatively with increased rates of recurrent instability compared to those without GLAD lesions.
Methods:
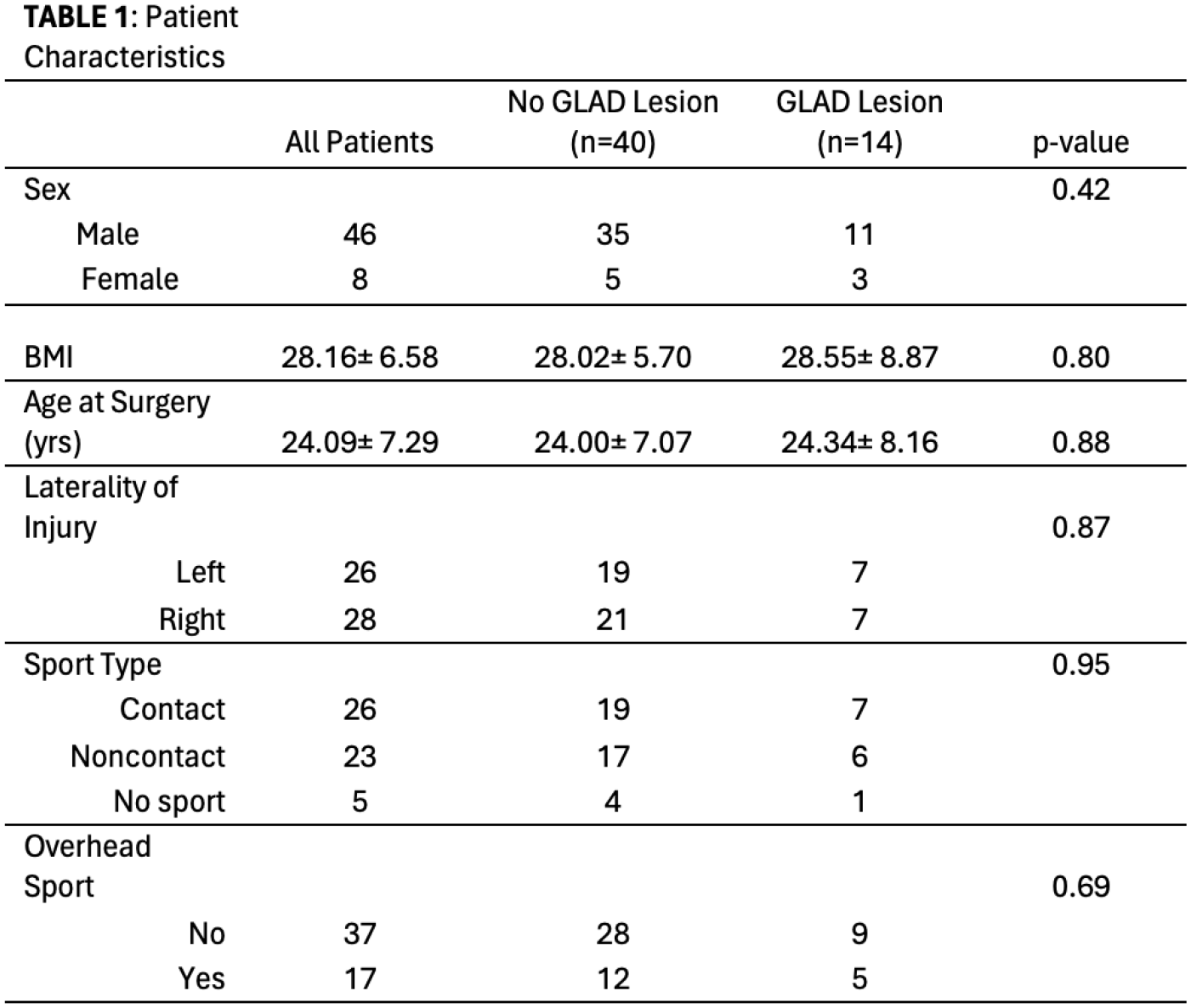
This was a retrospective comparative case series of consecutive patients with GLAD lesions in the setting of first-time anterior instability events who underwent arthroscopic Bankart repair. Patients aged 14 to 50 years between 2012-2020 were included. Those with a history of recurrent or chronic anterior instability, posterior instability, multidirectional instability, or incomplete medical records were excluded. A total of 54 patients were included for analysis. 14 patients with GLAD lesions (cases) were matched in a 1:3 ratio for age and BMI to those without GLAD lesions (controls). Additional demographic data collected included laterality of injury, contact sport, and overhead sport participation. Primary outcomes included postoperative ROM (forward elevation and external rotation) and PROs: Subjective Shoulder Value (SSV), Visual Analog Scale (VAS), and Western Ontario Shoulder Instability Index (WOSI). Recurrent instability following primary arthroscopic stabilization was also collected. STATA was used for data analysis. Statistical significance was set at P ≤ 0.05.
Results:
The mean age was 24.00±7.07 and 24.34±8.16 years in the control and GLAD groups respectively (p=0.88). Average follow-up from surgery to final clinic visit was 1.37 years, while the average time from surgery to final PROs collection was 8.00 years for both groups. There were no significant differences between groups regarding BMI, laterality of injury, contact sport participation, or overhead sport participation (
Conclusions:
Patients with GLAD lesions in the setting of first-time anterior instability had comparable PROs, forward flexion, and external rotation postoperatively to controls. In addition, the presence of a GLAD lesion did not influence the rate of recurrent instability. Although larger prospective studies are necessary to draw firmer conclusions, the findings of this study can guide clinical decision making, especially as it pertains to return to sports and postoperative rehabilitation. Given similar outcomes and rates of recurrent instability, our results support similar rehabilitation protocol for those with and without GLAD lesions following arthroscopic stabilization after a first-time anterior instability event.