Abstract
Objectives:
Although magnetic resonance imaging (MRI) is one of the crucial imaging modalities for identifying shoulder disorders, its usefulness for identifying shoulder pathology in overhead-throwing athletes is yet to be determined. Superior labrum anterior and posterior lesions and internal impingement in MR findings are characteristic findings for overhead-throwing disorders.However, a previous study demonstrated that MRI abnormalities consistent with internal impingement could be observed in asymptomatic patients. Furthermore, another study reported that MRI findings were not predictive of future injury list placement or duration of placement.
Glenohumeral stability is important for over overhead-throwing athletes. Jobe and Bradley stated that a lack of shoulder stability leads to common disorders in young athletes. A more recent study suggested that the physiopathology of internal impingement with anterior instability in throwing athletes might be related to the dysfunction of the anterosuperior glenohumeral capsular ligament.The assessment of capsular redundancy on MR arthrography, including the abduction external rotation (ABER) position, allows for accurate differentiation of patients with shoulder instability.
This study aimed to compare MR arthrography findings in the ABER position among internal impingement with anterior instability, traumatic shoulder dislocation, and multidirectional instability (MDI).
Methods:
Data from consecutive patients who were treated in our hospitals were retrospectively reviewed. Between August 2017 and December 2023, 243 patients underwent surgery for shoulder instability, including overhead-throwing disorders (throwing group), traumatic dislocation (dislocation group), and MDI (MDI group). Shoulder instability was diagnosed based on traumatic episodes, physical examination, plain radiography, and MRI. The present study defined internal impingement with anterior instability presenting positive outcomes in painful or loose anterior apprehension and relocation tests (Jobe’s relocation test). All examinations were started after intra-articular injection including iotrolan 240 mg/ml and gadoteridol. Once MR examination in a neutral position was completed, patients were instructed to place the ipsilateral hand behind the head or neck with the elbow flexed to obtain the ABER position.
In total, 82 shoulders (69 males and 13 females; mean age, 25.7 ± 10.2 years) who underwent arthroscopic procedures were divided into three groups: 32 shoulders in the throwing group, 39 in the dislocation group, and 11 in the MDI group. We classified the glenohumeral capsular ligaments into the following four types based on a previous report: taut, disappearance, crescent sign, and fluctuation sign (Figure 1). In addition, the triangular accumulation of intra-articular contrast material between the humeral head, articular surface of the glenoid, and glenohumeral capsular ligament was independently evaluated for glenohumeral joint stability in the ABER position as a triangle sign.
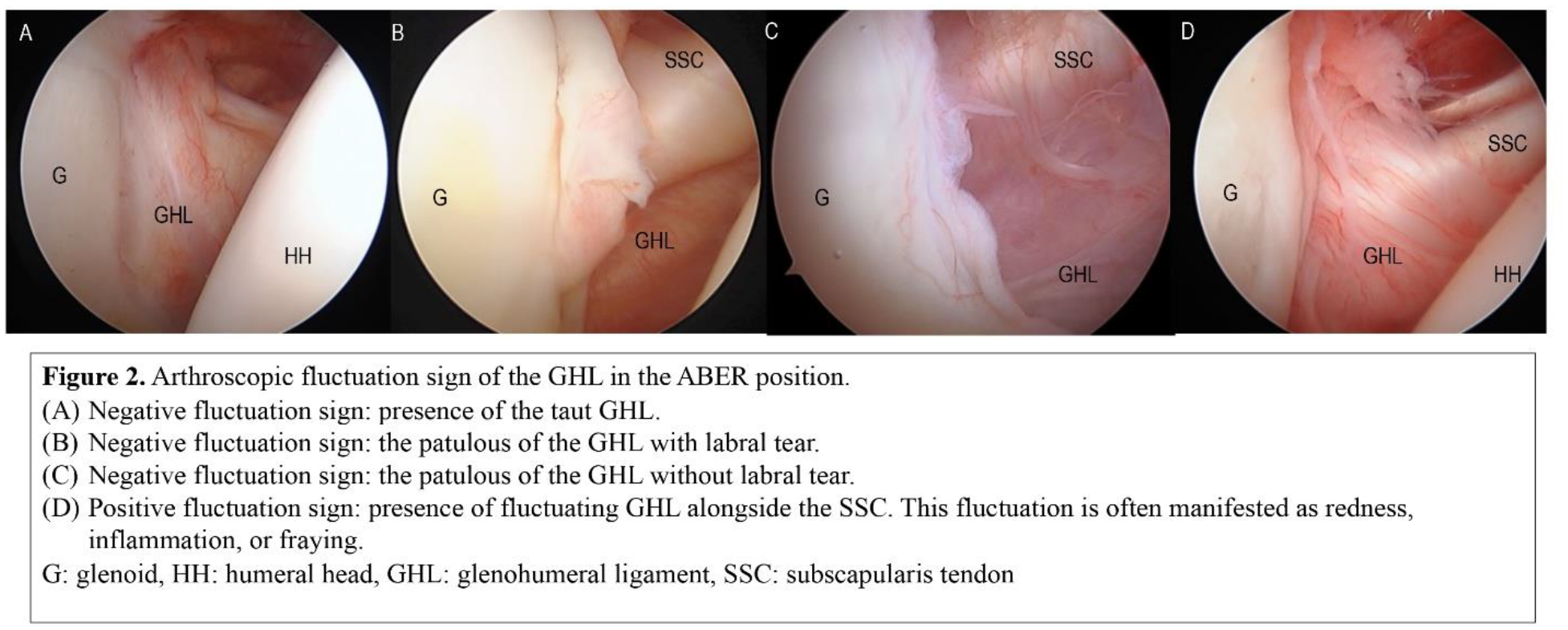
Arthroscopic fluctuation sign of the GHL was defined as follows:
Negative: The GHL appeared either completely taut (Figure 2A) or patulous with labral tear (Figure 2B) or without labral tear (Figure 2C) in the ABER position.
Positive: In the ABER position, the GHL exhibited upward displacement accompanied by fluctuations alongside the subscapularis tendon. This fluctuation is often manifested as redness, inflammation, or fraying (Figure 2D). Compared with arthroscopic findings, MR arthrography in the ABER position was evaluated for its accuracy in detecting the fluctuation sign.
Results:
MR arthrography revealed that the fluctuation sign in 72% of patients in the throwing group was significantly greater than that in 27% and 21% of those in the MDI and dislocation groups, respectively (P < 0.001, Table I). Conversely, in the MDI group, the crescent sign in 55% of the patients had a notably higher incidence compared to 23% and 13% of those in dislocation and throwing groups, respectively. MR arthrography revealed that the triangle sign in 66% of patients in the throwing group was significantly greater than that in 31% of those in the dislocation group (P < 0.001). The arthroscopic fluctuation sign of the GHL was more frequent in 72% of the patients in the throwing group than in 18% and 15% of those in the MDI and dislocation groups, respectively. Compared with the arthroscopic findings, MR arthrography findings in the ABER position achieved an accuracy of 84% for detecting the fluctuation sign. (Table II)
Conclusions:
The fluctuation signs on MR arthrography findings in the ABER position were found more frequently in overhead-throwing athletes with internal impingement and anterior instability than in patients with traumatic shoulder dislocation and MDI. The fluctuation of the GHL on MR arthrography in the ABER position was defined as a relatively thick but fluctuating GHL. The majority of GHLs (85%) in the throwing group were categorized as either taut or exhibiting fluctuation, where the GHL was clearly visible on MR arthrography in the ABER position. In addition, the triangle signs on MR arthrography findings in the ABER position were found more frequently in overhead-throwing athletes than in patients with traumatic shoulder dislocation. Our study indicated that MR arthrography in the ABER position could potentially detect characteristic lesions of internal impingement with anterior instability in throwing athletes. These findings may be useful for the correct diagnosis and appropriate treatment strategy for disabled overhead-throwing athletes with internal impingement and anterior instability.