Abstract
Objectives:
Shoulder pain is one of the leading causes of disability in the United States, with rotator cuff pathology being the primary cause. As a result, rotator cuff repair (RCR) is one of the most commonly performed orthopaedic procedures, with an incidence of greater than 400,000 per year and an annual prevalence reaching 7.4%. With the evolution of technology and implants utilized in RCR comes great variability in day-of-surgery costs, with much of this variability accounted for by surgeon-directed costs (i.e. implants, devices, and disposables). Suture anchors are the most expensive and variable surgeon-directed cost in primary rotator-cuff repair.
The purpose of this study was to determine the relationship between fixation construct costs and change in patient-reported outcomes over a one year episode of care. We hypothesize that there will not be a significant correlation between patient-reported outcomes and construct cost.
Methods:
This retrospective review was performed at two academic centers. Patients that underwent rotator cuff repair from 2018 to 2022 were identified through the institutional patient-reported outcomes (PROs) database. Patients with incomplete baseline and 1-year PROs, history of surgery on the operative shoulder, history of fractures about the shoulder of interest, and isolated subscapularis tears were excluded.
Patient demographics and history including age, body mass index (BMI), sex, American Society of Anesthesiologists, hand dominance, smoking status, diagnosis of depression or anxiety, alcohol or substance use, and diagnosis of diabetes mellitus or rheumatoid arthritis were collected through retrospective review of the patient’s medical record. Injury and surgical characteristics including injury chronicity, tear size, tendon involvement, concomitant procedures (i.e. biceps tenodesis, biceps tenotomy, subacromial decompression (SAD) and distal clavicle excision (DCE)), and fixation technique (single row, double row, or transosseous) were extracted from surgeon clinic notes and operative reports. PROs collected at baseline (preoperatively) and 1-year include Single Assessment Numerical Evaluation (SANE), American Shoulder and Elbow Surgery (ASES), and Visual Analog Scale (VAS). Anchor-based minimum clinically important difference (MCID) was calculated based on a 1-point improvement in VAS scores over the one-year episode of care. Clinical outcomes include symptomatic retear, complications, and reoperations within 1 year postoperatively. Quantity and cost of the fixation constructs were pulled from the institutional charge master database.
Statistical analysis was performed using Intellectus Statistics (Clearwater, FL).Descriptive analyses include means and standard deviations for scale variables, and counts and percentages for categorical variables. Chi-squared, Fischer Exact, T-tests, Mann Whitney-U, ANOVA, Pearson correlations, and Spearman correlations were utilized, as appropriate. Construct cost was analyzed as a scale variable and binned into quartiles (each quartile n = 225) for further analysis. Statistical significance was set at an alpha value of p ≤ 0.05.
Results:
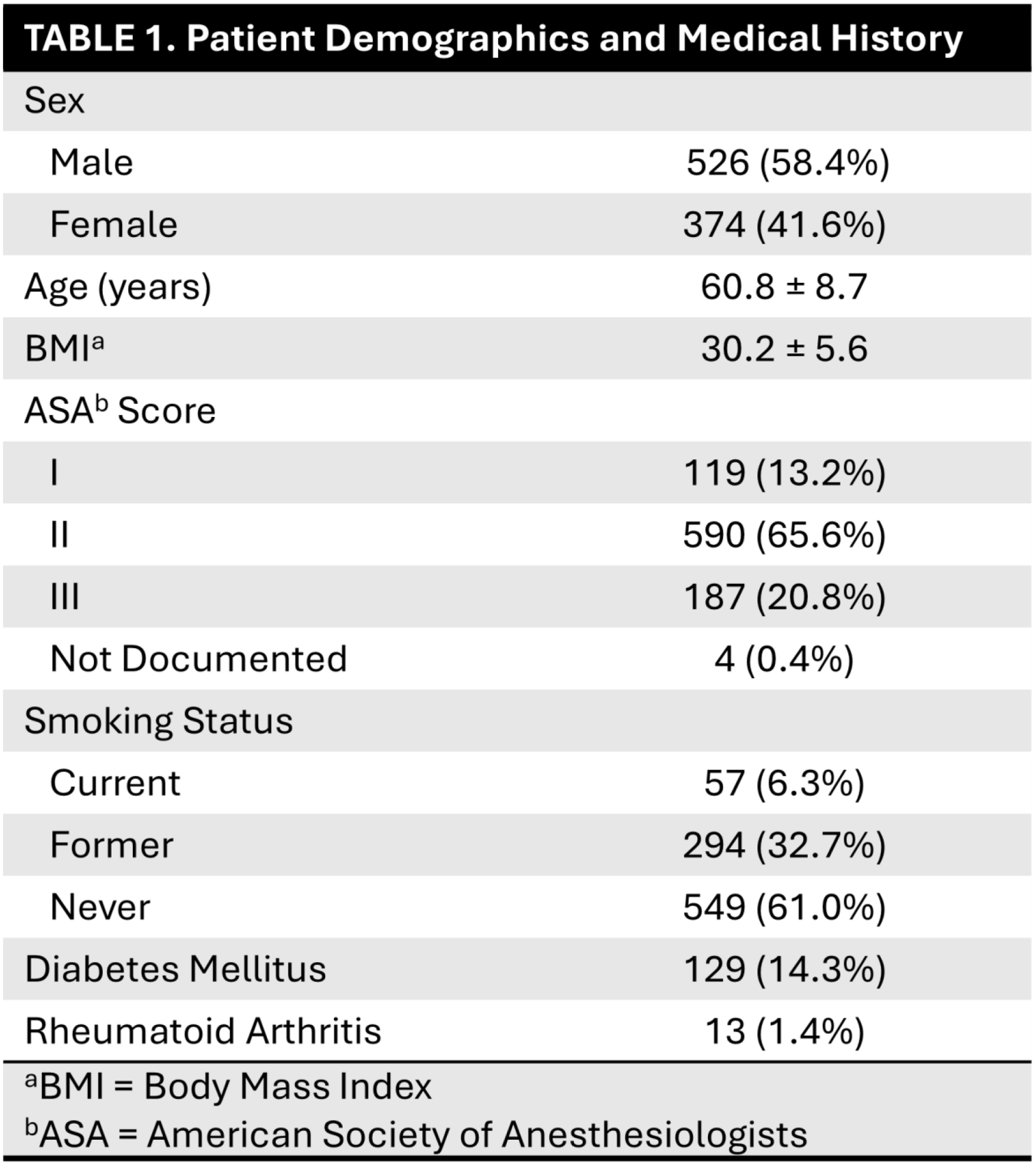
A total of 900 patients met criteria for inclusion in this study. The majority of patients were male (n = 526, 58.4%), with an average age at procedure of 60.8 ± 8.7 years. The average BMI was 30.2 ± 5.6 kg/m2, and the most common ASA score was II (n = 590, 65.6%). One hundred twenty-nine patients (14.3%) had a diagnosis of diabetes mellitus, and 57 patients (6.3%) were current smokers at the time of procedure (Table 1). Nearly all patients (n = 873, 97.0%) had tears involving the supraspinatus, and 478 (53.1%) had tears involving the infraspinatus (Table 2). The most common adjuvant procedure was subacromial decompression (n = 768, 85.5%), followed by biceps tenodesis (n = 221, 24.6%). Most fixation constructs involved three or fewer anchors (1 anchor: n = 226, 25.1%; 2 anchors: n = 218, 24.2%; 3 anchors: n = 206, 22.9%), with the maximum number of anchors in any one procedure being 13 (n = 1, 0.1%). The average total construct cost for the rotator cuff repair was $1,266.94 ± $864.03 (not including biceps fixation). Thirty-nine patients (4.3%) had a symptomatic retear within one year of the index procedure, with 17 patients (1.9%) undergoing reoperation within one year.
The average baseline ASES score for the entire cohort was 47.8 ± 17.4, increasing to 84.6 ± 17.9 at one year postoperatively. SANE scores saw similar increase from 41.4 ± 21.3 at baseline to 83.1 ± 20.6 at one year follow-up. The average VAS score at baseline was 4.8 ± 2.3, with improvement to an average of 1.4 ± 2.2 at one year postoperatively. Anchor-based MCID for ASES was 21.7, with 78.8% of patients (n = 709) meeting MCID.
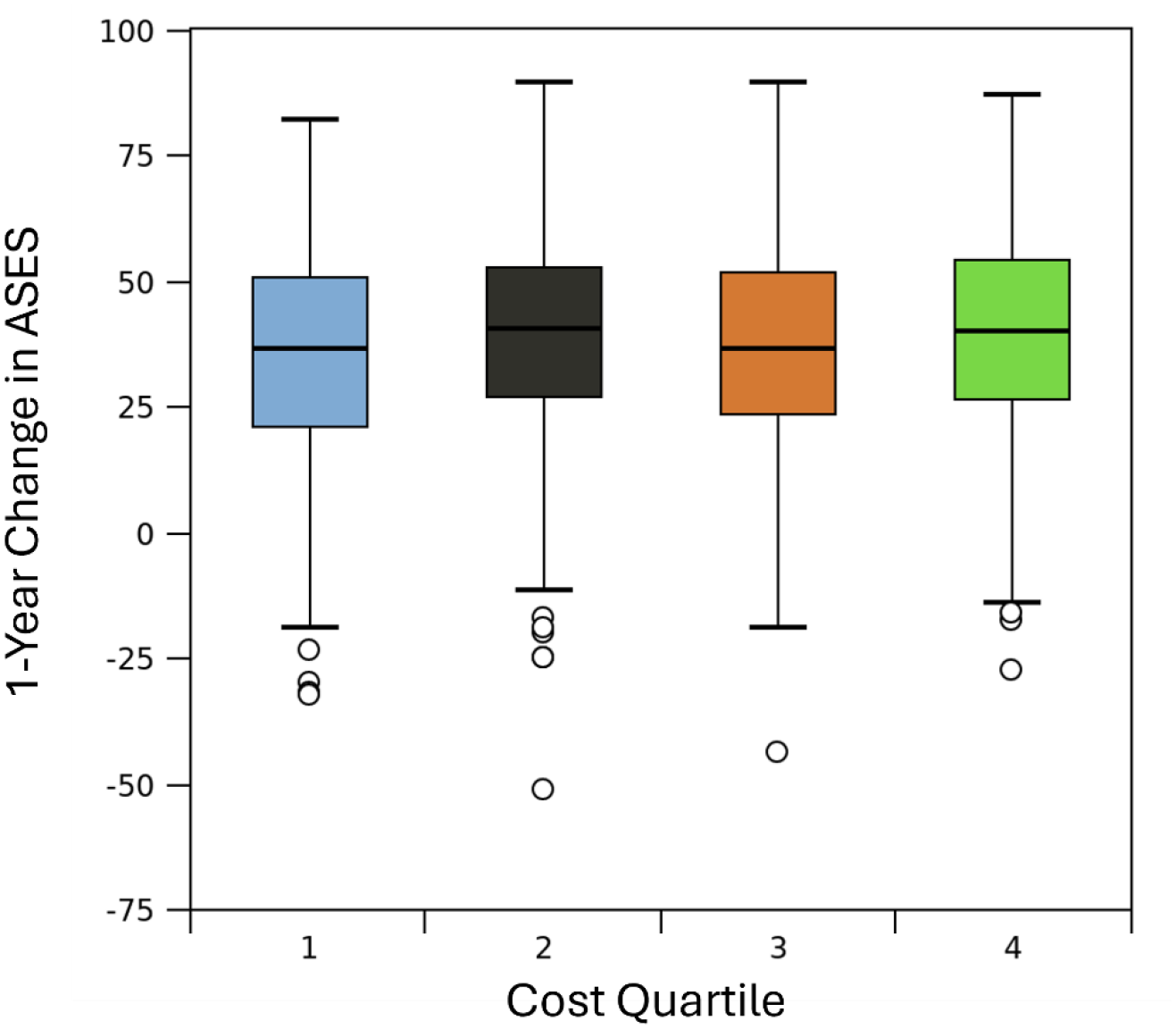
There was no correlation between construct cost and improvement in ASES score (r = 0.03, p = 0.458). There was no difference in average construct cost between those that met MCID and those that did not ($1,281.76 ± 882.26 vs $1,210.91 ± 791.1, respectively; p = 0.322). There was no significant difference in ASES score improvement between implant cost quartiles (p = 0.146). Subanalysis based on number of tendons involved revealed no correlation between construct cost and improvement in ASES for any number of tendons involved (r < 0.11 for all) (Figure 2).
Conclusions:
With the permeation of value-based care initiatives across orthopaedic policy and reimbursement, cost containment initiatives while maintaining patient-reported outcomes will be critical. The variation in construct cost for RCR presents an optimal opportunity for cost containment. The present study demonstrates no significant correlation between construct costs and PROs following primary RCR. Along with careful consideration of patient safety and repair integrity, surgeons should consider construct costs in surgical decision-making pathways.