Abstract
Objectives:
Patients with seizure disorders are at risk for shoulder instability. Management of these patients is challenging given they often present with more complex pathology and higher bone loss compared to patients without seizures. This leads to high recurrence rates and varied functional outcomes. This study aims to evaluate demographic trends, functional outcomes, and recurrence rates in patients with seizure disorders undergoing shoulder stabilization surgery
Methods:
This single-institution, retrospective study compares patients with at least one seizure occurrence prior to shoulder stabilization surgery for recurrent shoulder instability to those without seizures who underwent the same surgeries. Procedures were performed by seven surgeons between 2009 and 2023. The primary procedures included Bankart repair, Latarjet, distal tibial allograft, Hill Sachs bone grafting, and remplissage. Data collected from electronic medical records encompassed patient demographics, clinical outcomes, functional markers, and recurrence rates.
Results:
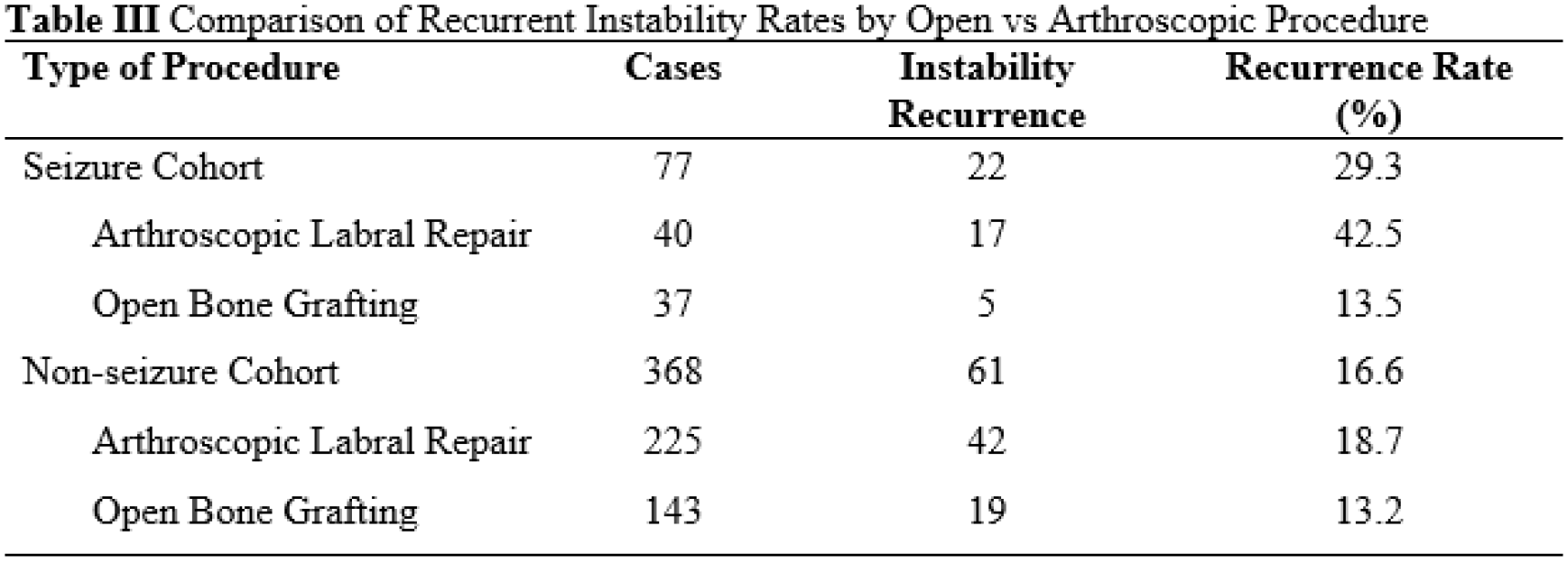
A total of 445 patients (332 male, 113 female) with recurrent shoulder instability underwent stabilization surgery. Of these, 77 had at least one seizure on average 2.4 years prior to index procedure. The seizure cohort included 38 patients with epileptic seizures and 39 with non-epileptic seizures. The mean age at time of instability surgery in the seizure group was 29.6 ± 8.2 years, with a mean follow-up period of 2.0 ± 3.0 years. These patients had a significantly higher Charlson Comorbidity Index (CCI) score (0.3 ± 0.8 vs. 0.1 ± 0.5, p=0.037) and American Society of Anesthesiologists (ASA) physical classification score (2.1 ± 0.5 vs. 1.5 ± 0.6, p=0.001) compared to the non-seizure group. The seizure cohort also had significantly higher rates of current smokers (41% vs 13%, p<0.001) and depression (60% vs 20%, p<0.001). Recurrent instability was the primary indication for surgery in all patients. Surgical management in the seizure group included arthroscopic labral repair (n=40) or open bone grafting (n=37). The direction of instability in the seizure group was anterior in 83% of seizure patients (vs. non-seizure: 77%). Average glenoid bone loss was significantly higher in the seizure group (19% vs 13%, p=0.009). Patients with seizures had significantly lower preoperative and postoperative ranges of motion (ROM) in forward elevation (FE), external rotation (ER), and internal rotation (IR), except for preoperative IR. Preoperative and postoperative strength was 5/5 in all measures between cohorts. Recurrent instability was significantly higher in the seizure group (29% vs. 17%, p=0.014). Within the seizure group, the recurrent instability rate was 43% for arthroscopic labral repair and 14% for open bone grafting (vs. 19% and 13% in the non-seizure group, respectively). The 2-year and 5-year recurrence-free rate was found to be significantly lower at 61% and 50% in the seizure group, compared to 80% and 58% in the non-seizure group (p=0.049). There were 13 seizure patients with seizure recurrence following Latarjet procedure. Among the 13 patients, one had recurrent instability leading to revision. Between groups, revision rates were similar: 13% of seizure patients underwent revision on average 2.9 years after the index procedure compared to 11% of non-seizure patients at 3.1 years. The 5-year revision-free rate was comparable between groups (seizure = 72%, non-seizure = 67%; p=0.94).
Conclusions:
Patients with shoulder instability and seizure disorders are a challenging subset of patients who have a high recurrent instability rate after surgical management compared to non-seizure patients. Recurrence is more likely to occur within the first 2 years following surgery in seizure patients. Patients undergoing arthroscopic labral repair had a higher rate of recurrence when compared to those undergoing open bone grafting as their stabilization procedure, regardless of seizure status. Addressing bone loss, reported as 18.6% in this cohort, is crucial to the success of these procedures. Shoulder ROM was lower in patients with seizures, emphasizing the overall goal of attaining shoulder stability rather than improved mobility. Additionally, seizure patients had higher rates of smoking, depression, and comorbidities, further complicating their management. Preoperative planning, comprehensive patient counseling, and tailored surgical approaches are essential to improve postoperative outcomes in this complex patient population.