Abstract
Objectives:
Among existing biologics used within the field of orthopaedics, bone marrow aspirate concentrate (BMAC) has become a popular option for surgeons in recent years. BMAC has shown to contribute to satisfactory outcomes, including improved wound healing and superior patient-reported outcomes, following various orthopaedic procedures. Several studies have documented the surgical technique for meniscus repair with the use of BMAC, while others have described the effects of the use of BMAC on the quality of meniscal tissue following repair. However, few studies have investigated patient-reported outcomes after meniscus repair with the use of BMAC. Therefore, the purpose of this study was to compare clinical outcomes in patients undergoing arthroscopic meniscus repair with and without the use of BMAC.
Methods:
A prospective, multi-surgeon cohort study was conducted on all patients undergoing arthroscopic meniscus repair without BMAC (MR) and with BMAC (MR-BMAC) between October 2021 and January 2024. An electronic survey of patient-reported outcome measures (PROMs) was completed by each patient at a minimum of 6 months postoperatively. PROMs included a visual analog scale (VAS) for pain, University of California, Los Angeles (UCLA) activity scale, the Lysholm Knee Scoring Scale (LKSS), the Knee Outcome Score - Sports Activities Scale (KOS-SAS), and the International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form.
Results:
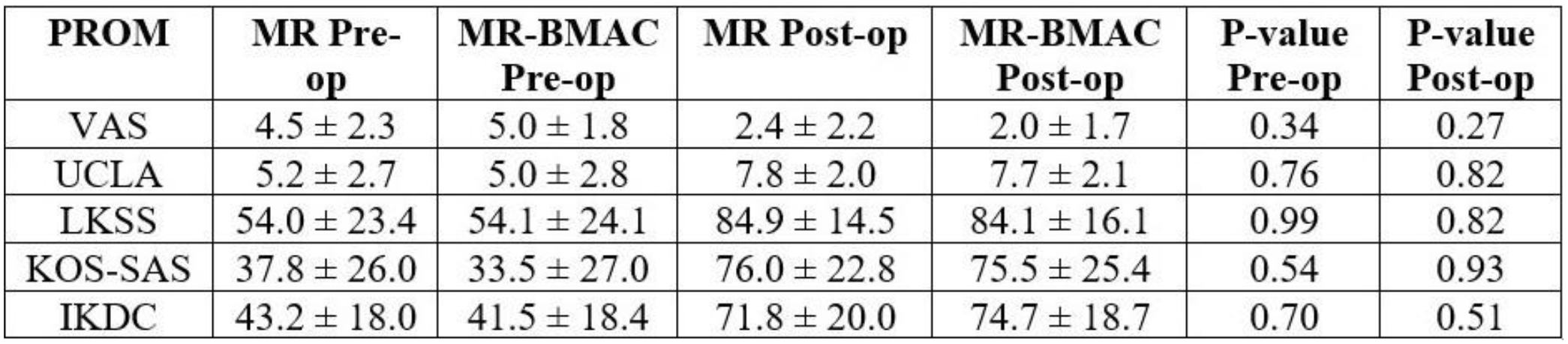
Ninety patients were reached for follow-up (46 MR, 44 MR-BMAC). Patients in the MR group were significantly younger than patients in the MR-BMAC group at the time of surgery (32.0 ± 15.6 vs. 41.8 ± 14.8 years old, p=0.003). No differences were found between MR and MR-BMAC groups in terms of sex (51.4% vs. 48.6% female, p=0.34), body mass index (BMI) (26.4 ± 4.4 vs. 27.4 ± 4.7, p=0.46), or time to follow-up (11.5 ± 5.6 vs. 13.1 ± 6.7 months, p=0.24). There were no significant differences between MR and MR-BMAC groups in terms of preoperative PROMs including VAS (4.5 ± 2.3 vs. 5.0 ± 1.8, p=0.34), UCLA (5.2 ± 2.7 vs. 5.0 ± 2.8, p=0.76), LKSS (54.0 ± 23.4 vs. 54.1 ± 24.1, p=0.99), KOS-SAS (37.8 ± 26.0 vs. 33.5 ± 27.0 p=0.54), and IKDC (43.2 ± 18.0 vs. 41.5 ± 18.4, p=0.70). The most commonly performed concomitant procedure in both groups was anterior cruciate ligament (ACL) reconstruction.
There were no differences between MR and MR-BMAC groups in terms of the proportion of patients undergoing meniscus repair with all-inside (87% vs. 86%, p=0.82), inside-out (2.2% vs. 0%, p=0.54), outside-in (0% vs. 2.5%, p=0.38) techniques, or meniscus root repairs (11% vs. 13%, p=0.79). There were no differences between MR and MR-BMAC groups in terms of their postoperative PROMs including VAS (2.4 ± 2.2 vs. 2.0 ± 1.7, p=0.27), UCLA (7.8 ± 2.0 vs. 7.7 ± 2.1, p=0.82), LKSS (84.9 ± 14.5 vs. 84.1 ± 16.1, p=0.82), KOS-SAS (76.0 ± 22.8 vs. 75.5 ± 25.4, p=0.93), and IKDC (71.8 ± 20.0 vs. 74.7 ± 18.7, p=0.51) (Table 1).
Conclusions:
Our study demonstrates comparable postoperative PROMs in patients undergoing arthroscopic meniscus repair with and without the use of BMAC. Larger studies with longer follow-up duration are warranted to further corroborate these findings and better delineate the effects of BMAC on meniscus repair.