Abstract
Objectives:
Objective: The purpose of this study was to evaluate UCL injured patients using both dynamic valgus stress ultrasound and the FEVER MRI to assess its reliability in confirming the diagnosis of an incompetent UCL requiring surgery.
Methods:
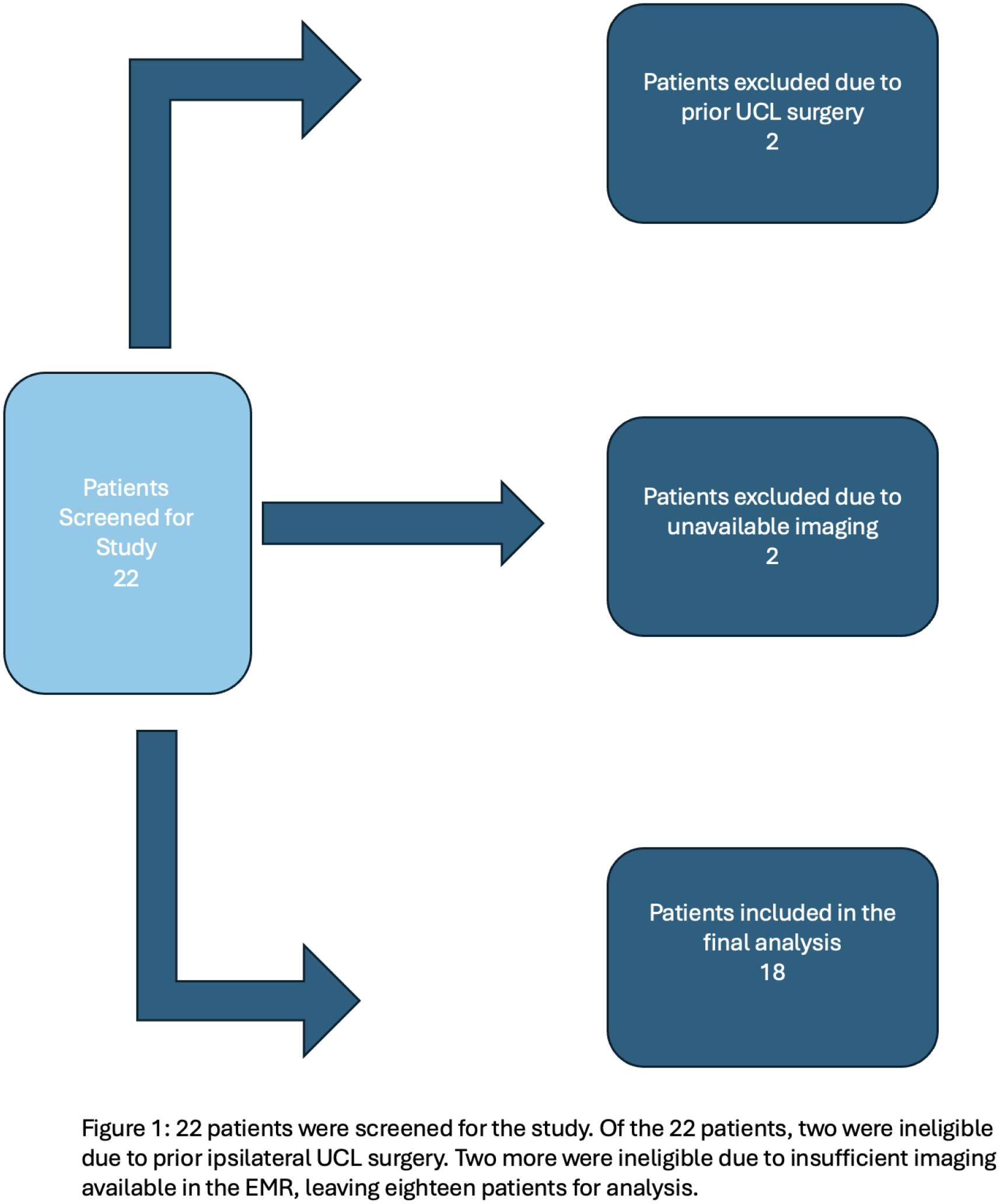
Methods: Professional and varsity athletes who met inclusion criteria of the following were included in the study: >16 years of age, acute presentation with signs of UCL injury, participation in an overhead throwing sport. Exclusion criteria included prior ipsilateral UCL surgery, other concomitant elbow injuries, and patients who could not undergo MRI. Both a valgus stress US performed by one blinded MSK radiologist and a FEVER MRI were conducted on all patients according to protocol. A positive stress ultrasound was defined as >2mm widening of the ulnohumeral joint with valgus stress of the elbow compared to neutral, while a positive FEVER MRI was defined as >1mm widening on stress sequence compared to the neutral sequence. Using positive stress ultrasound as a marker for true injury, sensitivity and specificity were calculated based on the results from the MRI to determine the ability of the FEVER MRI to detect a UCL tear.
Results:
Results: Of the 18 patients who met inclusion criteria, 16 were male (89%), the average age at presentation was 20.7 years (range 16-28), and 13 were right-handed (72%). Of the 18 patients, seven had a UCL injury as defined by a dynamic stress ultrasound with greater than 2mm of ulnohumeral gapping. All seven patients with a positive ultrasound also had greater than 1mm ulnohumeral gapping on FEVER MRI. Furthermore, all 11 patients who had a negative stress ultrasound also had a negative FEVER MRI (Sn 1.0, Sp 1.0). Four patients with a positive test underwent surgery, while the other three patients all had surgery recommended to them but elected not to undergo the procedure.
Conclusions:
Conclusion: A correct diagnosis of an ulnar collateral ligament injury is critically important when deciding to perform a ligament reconstruction in high level athletes. All patients in this study with a positive UCL stress ultrasound (>2mm ulnohumeral gapping) also had a positive FEVER MRI (>1mm ulnohumeral gapping). Additionally, there were no patients with a positive FEVER MRI and a negative UCL stress ultrasound. Therefore, the FEVER MRI may be both sensitive and specific for detecting UCL injuries and guiding surgical decision making while obviating the need for joint contrast fluid.