Abstract
Objectives:
Addressing patellofemoral instability in the skeletally immature patient population has historically posed challenges as it is essential to respect the growth plates to avoid growth arrest and subsequent associated complications. Medial patellofemoral ligament reconstruction (MPFL-R) is an effective procedure to address patellar instability, but in skeletally immature patients, standard anchor placement is often modified to avoid violation of the distal femoral physis. The purpose of this study was to compare post-operative outcomes between skeletally immature and skeletally mature patients who underwent isolated MPFL-R.
Methods:
This study represents a subset of patients from the prospectively-collected multi-center Justifying Patellar Instability Treatment by Results (JUPITER) cohort study, which utilized pre-defined research questions and hypotheses for inclusion – inclusive of the forthcoming analysis. Twenty-seven surgeons from twelve academic centers throughout the United States enrolled patients with a primary complaint of patellar instability and performed indicated procedures as guided by their specific training and clinical indications. Inclusion criteria were patients who underwent a primary, single-stage, isolated medial patellofemoral ligament reconstruction (MPFL-R) without concomitant boney procedure from January 2017 through July 2022. Patients were excluded if there was no discrete treatment data, no known skeletal maturity status, and no modification listed to address placement of the femoral tunnel in a skeletally immature patient – to reflect clinical equipoise. Collected patient data included age, sex, BMI, and Beighton score. Radiographic parameters included Caton-Deschamps Index (CDI), tibial tubercle-trochlear groove distance (TT-TG), axial width of the patellar tendon beyond the lateral trochlear ridge (PT-LTR), and trochlear crossing sign. Surgical data included MPFL-R graft type and concomitant procedures. Collected patient-reported outcome measures (PROM) include KOOS Pain, KOOS Symptoms, KOOS ADL, KOOS Sport/Rec, KOOS QOL, KOOS JR, Pedi-FABS, Pedi-IKDC, Banff Patellar Instability Index 2.0 (BPII 2.0), and Kujala at baseline, 1, 2, and 5 years. Paired and unpaired t-tests were used to assess the difference in means between the two groups over time, where appropriate. Chi-square test of independence was used to examine the discrepancy in frequencies between the two groups.
Results:
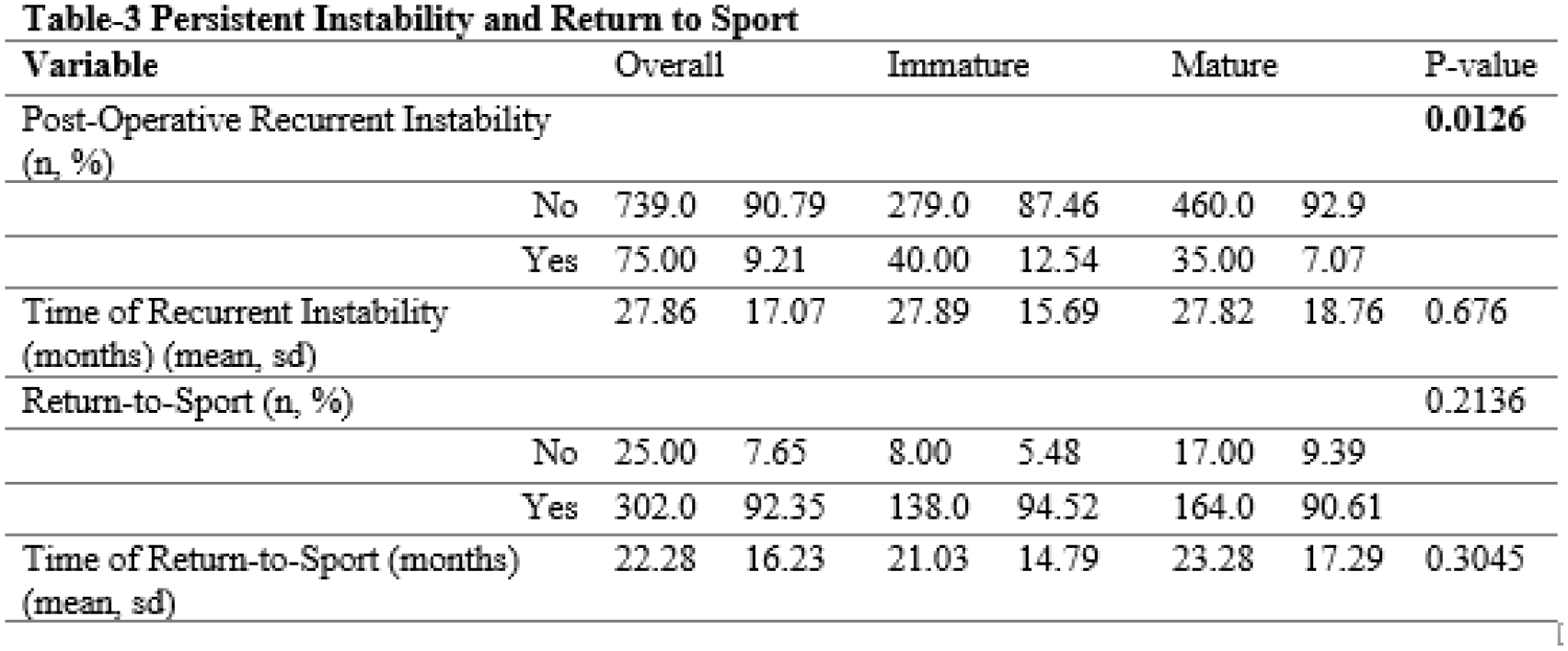
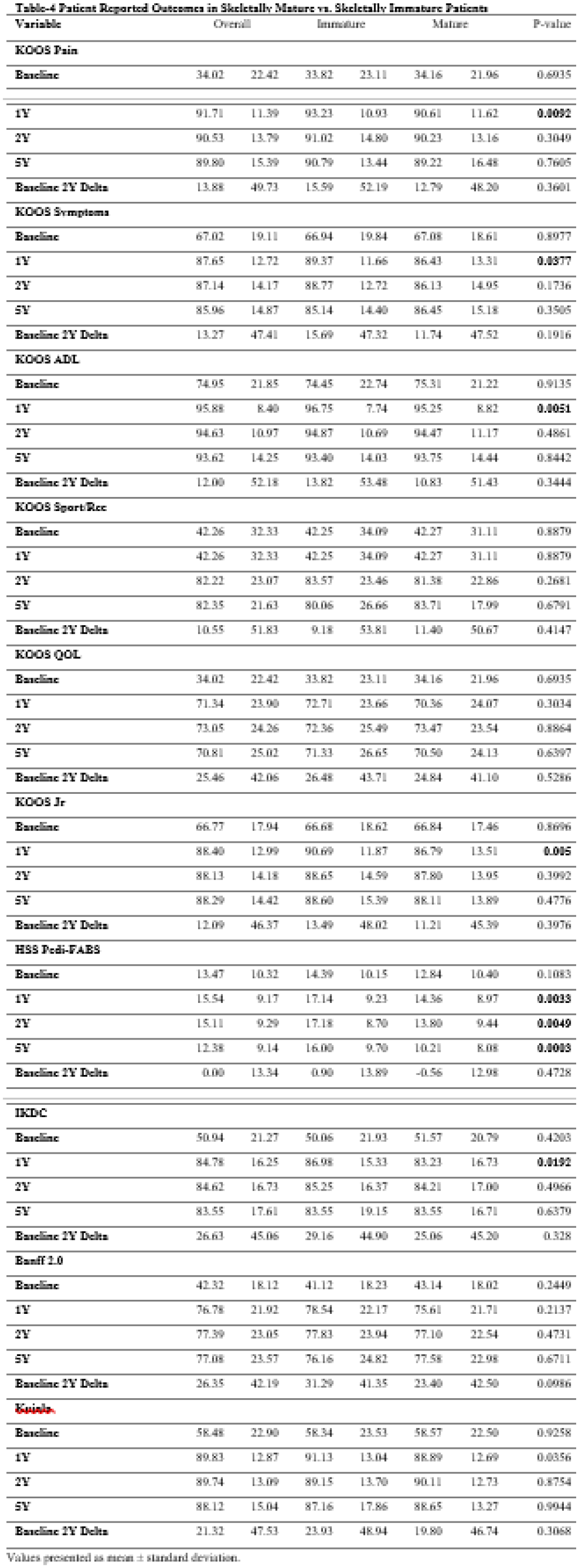
814 patients (16 ± 3.6 years old, 59.2% female) underwent isolated MPFL-R from January 2017 through July 2022. 319 (39%) of these patients were skeletally immature at the time of surgical intervention. When compared to skeletally mature patients, skeletally immature patients were younger (13.7 ± 1.9 vs. 17.5 ± 3.7 years, p < 0.0001), more often male (50.8% vs. 64.7%, p = 0.0002), and had a lower mean BMI (22.2 ± 5.4 vs. 25.5 ± 5.8, p < 0.0001) (Table 1). Skeletally immature patients were also found to have increased incidence of patella alta (71% vs 67%, p < 0.0001) and a higher PT-LTR (9.9 ± 6.5mm, 7.9 ± 6.5mm, p = 0.0396) than skeletally mature patients. There were additional significant differences in graft type (less autograft, more tibialis anterior and semitendinosus). Skeletally immature patients had lower rates of chondroplasty (32.3% vs. 46.7%, p < 0.0001) and higher rates of osteochondral fracture treatment (17.5% vs. 9.9%, p = 0.0018) than skeletally mature patients (Table 2). Skeletally immature patients experienced significantly more post-operative recurrent instability (12.5% vs. 7.0%, p = 0.0126, at a mean time of 27.8 months) than skeletally mature patients. There was no significant difference in rates of return-to-sport between the two groups (p = 0.2136) (Table 3). There were no significant differences in baseline PROMs between the two groups. At 1 year post-operatively, skeletally immature patients had higher KOOS Pain, KOOS Symptoms, KOOS ADL, KOOS JR, and Pedi-IKDC (p < 0.05) but this significance was not maintained at 5 years. The difference in Pedi-FABS between the two groups persisted through 5 years post-operatively (Table 4).
Conclusions:
This study showed that skeletally immature patients experienced post-operative recurrent instability at a higher rate than skeletally mature patients. Rates of recurrent instability are consistent with the current published literature; however, the rate of recurrent instability is lower than reported in previous literature, potentially representing an improvement in isolated MPFL-R techniques over time. The greater PROMs for skeletally immature patients at 1-year that becomes similar at 2 and 5 years may represent faster recovery in the immediate post-op period for the younger population, which balances out over time. Future studies may allow for an attempt to discern a difference in outcomes based on type of physeal-sparing technique.