Abstract
Objectives:
Os trigonum (OT) syndrome involves an accessory bone at the posterior talus crowding the tarsal tunnel and is frequently described in performance athletes, such as dancers, cheerleaders, and gymnasts. When reaching terminal plantarflexion as such athletes frequently do, OT can cause painful impingement of the posterior ankle. A low-lying flexor hallucis longus (FHL) muscle belly may aggravate symptoms. Local anesthetic injection is used as a diagnostic measure and initial intervention, with >80% immediate symptom resolution, and is preferred to casting. Surgical excision of OT also results in symptom resolution. We aimed to describe short-term pain relief of pediatric patients undergoing an injection of the OT and evaluate the relationship between several patient factors and progression to surgery.
Methods:
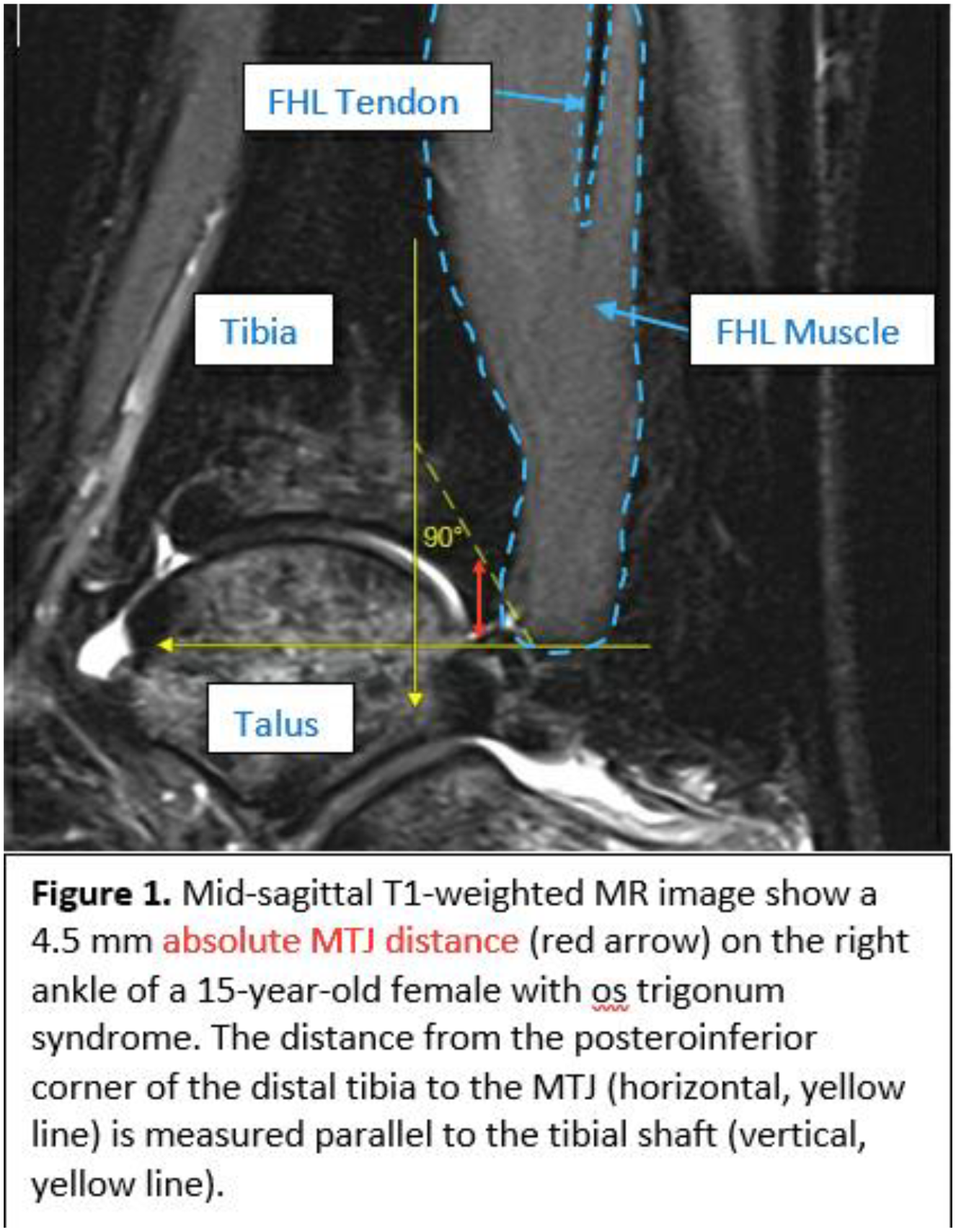
Retrospective review at one institution was conducted of patients with diagnosis codes for OT syndrome between 2014 and 2023. We collected demographics, treatment details, injection content (lidocaine with or without betamethasone), post-injection symptom relief, and radiographic measurements: regional maturity (distal tibial physeal status), musculotendinous junction (MTJ) distance from end of tibia to end of FHL muscle belly (Figure 1), relative MTJ- ratio of MTJ distance to the distance from tibia to tarsal tunnel, axial area of the FHL muscle belly or tendon at the midpoint of OT, and volume of OT. Volume of OT was calculated by multiplying OT length on the axial slice by OT area on the sagittal slice (Figure 2). Injections and surgeries were performed by one pediatric sports medicine specialist and two orthopaedic surgeons.
Results:
76 patients (59 female) with OT syndrome of mean age 13.9 ± 2.5 years were enrolled. 24 patients (26 ankles) underwent injections for OT. 17 patients (18 ankles) underwent surgical removal of OT. No patient or treatment factors that were collected were significantly related to post-injection symptom relief (p>0.05) (Table 1). Advancement to surgery is significantly related to FHL MTJ distance, relative FHL MTJ distance, the relative position of the OT against the talus, FHL muscle belly presence at the midpoint of the OT, distal tibial physeal status, gender, and whether the patient is a performance athlete (Table 2). The odds of advancement to surgery are significantly affected by FHL MTJ distance and relative FHL MTJ distance (p=0.009 OR=1.02, p=0.008 OR=1.13), but not by the initial level of relief from injection (p=0.453).
Conclusions:
Given the high prevalence of OT syndrome among performance athletes and the frequent use of plantarflexion in such activities, it is important for clinicians to understand the relationship between patient factors and level of relief from injection to the OT. Our results suggest that size and position of OT, physeal status, gender, being a performance athlete, sports participation, age, and presence of steroid with lidocaine injection are not related to immediate symptom relief from OT injection. This suggests that local lidocaine injection is effective across all patients. Because performance athletes rely heavily on the FHL when they bear weight on a plantarflexed ankle on demi-pointe and pointe, it is important for clinicians to understand the influence of the FHL on OT treatment. Our results suggest that FHL location and size are not related to immediate symptom relief from OT injection. Furthermore, initial level of relief from local injection does not predict likelihood of advancing to surgery. A more distal FHL MTJ location and a more inferior OT are significantly related to advancement to surgery. These factors may be associated with more severe symptoms, indicating that a low-lying FHL muscle belly and more inferior OT are used by providers as an indication for surgery. Gender and being a performance athlete, who are predominantly female, are each significantly related to progression to surgery for symptomatic OT. Patients who rely heavily on their ankles for their primary activity, such as performance athletes, may have more persistent OT symptoms indicating a need for surgery. Clinicians may consider these factors when determining treatment plans for pediatric and adolescent patients with OT syndrome.