
Abstract
Background:
There is limited and inconsistent evidence pertaining to comparative studies examining functional outcomes after acromioclavicular joint (ACJ) stabilization in either the acute or chronic setting for high-grade injuries.
Purpose/Hypothesis:
The purpose of the study was to compare functional outcomes of patients undergoing arthroscopically assisted ACJ stabilization for isolated acute or chronic type 5 ACJ injuries. It was hypothesized that patients would achieve similar functional outcomes at midterm follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Consecutive patients who underwent ACJ stabilization using coracoclavicular (CC) suspensory fixation with an additional acromioclavicular (AC) cerclage for isolated acute or chronic type 5 ACJ injuries from January 2015 to August 2021 and had a minimum follow-up of 2 years were identified and their records analyzed. Chronic ACJ injuries were defined as an interval of ≥3 weeks from injury to surgery according to the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine consensus statement and received an additional biological augmentation using a gracilis autograft. Functional outcome measures included the Constant-Murley (CM), American Shoulder and Elbow Surgeons (ASES), and Nottingham Clavicle (NC) scores as well as the visual analog scale (VAS) score for pain, which were compared between groups at the final follow-up.
Results:
A total of 82 patients (mean age at surgery, 40.3 ± 12.7 years; 54 acute and 28 chronic injuries) with a mean follow-up of 5.5 ± 2.0 years (range, 2.0-9.9 years) were included in the study. At the final follow-up, patients with acute or chronic injuries showed similar CM (acute: 85.3 ± 13.3; chronic: 85.5 ± 12.0; P = .98), ASES (acute: 94.3 ± 10.1; chronic: 93.5 ± 14.4; P = .69), and NC (acute: 85.6 ± 14.2; chronic: 86.8 ± 14.0; P = .68) scores. Furthermore, there was no difference in VAS score for pain (acute: 1.9 ± 1.1; chronic: 2.0 ± 1.6; P = .47) and postoperative subjective satisfaction with the cosmetic appearance of the ACJ (P = .753). Five patients in the acute group and 2 patients in the chronic group experienced failure and underwent revision surgery (acute: 9.3%; chronic: 7.1%; P = .75).
Conclusion:
Patients who underwent ACJ stabilization using CC suspensory fixation with an additional AC cerclage for isolated type 5 ACJ injuries in the acute setting achieved similar midterm functional outcomes, satisfaction with the cosmetic appearance of the ACJ, and failure rates to those who underwent delayed surgery with additional biological augmentation using a gracilis autograft ≥3 weeks after injury.
Acromioclavicular joint (ACJ) injuries represent up to 12% of traumatic shoulder injuries and typically show a high incidence in the young and active population.3,13,18 While contemporary evidence still supports a surgical treatment of high-grade (Rockwood types 5-6) ACJ injuries in specific cases, the technique used for surgical stabilization depends on the chronicity of injury.2,10,14,20 According to the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) Shoulder Committee, biological augmentation using a tendon auto- or allograft should be performed in chronic ACJ injuries (>3 weeks after injury), which has been implemented in current treatment guidelines. 3 Consequently, the urgency of surgical intervention is a critical factor in the shared decision-making process in patients with high-grade ACJ injuries. 3
Although a growing body of evidence reports favorable and reliable postoperative outcomes after arthroscopically assisted ACJ stabilization,11,14,23,24 there is limited and inconsistent evidence pertaining to comparative studies examining functional outcomes after ACJ stabilization in either the acute or chronic setting for high-grade injuries. Dey Hazra et al 7 found a superiority of early surgical stabilization (<3 weeks) for Rockwood type 3b and 5 ACJ injuries compared with delayed surgery (>3 weeks) in terms of functional scores. In contrast, Lädermann et al 12 observed that early (<2 weeks) and delayed (>2 weeks) surgical intervention resulted in equivalent clinical outcomes for type 3 to 5 ACJ injuries. However, these studies were limited to small sample sizes along with a heterogeneous severity of included ACJ injuries (Rockwood types 3-5), short follow-up period, and varied reconstruction techniques and graft augmentations in chronic cases.7,12
Thus, the purpose of the study was to compare functional outcomes of patients undergoing arthroscopically assisted ACJ stabilization for isolated acute or chronic type 5 ACJ injuries. It was hypothesized that patients who underwent delayed ACJ stabilization (≥3 weeks) in the chronic setting would achieve similar functional outcomes at midterm follow-up compared with those who underwent surgery in the acute setting (<3 weeks).
Methods
This was an institutional review board–approved retrospective monocentric outcome study of prospectively collected data (2022-223-S-Np). An institutional data bank review was performed to identify patients who underwent coracoclavicular (CC) suspensory fixation with an additional acromioclavicular (AC) cerclage for isolated acute or chronic type 5 ACJ injuries (according to the Rockwood classification 19 ) between January 2015 and August 2021 and had a minimum follow-up of 2 years. A type 5 injury was determined based on the preoperatively performed radiographs, which were obtained in a nonweighted panoramic view to measure the CC distance. Rockwood type 5 was defined by an increase of the CC distance >100% compared with the contralateral side. Patients were excluded if the ACJ injury was treated nonoperatively, stabilized using a different surgical technique, or not classified as Rockwood type 5 in the retrospective radiographic review. Furthermore, patients undergoing concomitant surgical procedures (eg, long head of the biceps tenodesis/tenotomy, rotator cuff repair, and labral repair) were excluded. Informed consent was obtained from each patient.
The decision in favor of nonoperative treatment was made after comprehensive and critical counseling about the advantages and disadvantages of both operative and nonoperative options. In doing so, the patient's functional demand and cosmetic expectation as well as the current complaints were specifically taken into account, and the therapy was determined according to the patient's individual preferences.
Surgical Technique
Arthroscopically assisted surgery was performed under general anesthesia. The patient was placed in the beach-chair position with the head slightly turned to the opposite direction to facilitate sufficient access to the clavicle. A thorough clinical examination was performed under anesthesia to assess the severity of ACJ instability and evaluate the possibility of anatomic manual reduction of the ACJ. After the operation field was prepared and draped in a sterile fashion, the arm was placed in a mechanical/passive arm holder.
First, diagnostic arthroscopy was performed via a standard posterior viewing portal using a 30° arthroscope. The joint was carefully assessed for concomitant intra-articular injuries. Subsequently, an anterior working portal was established in an outside-in technique through the rotator interval. Next, the arch and base of the coracoid process were carefully prepared with an electrothermal ablation device, while optimal visualization of the coracoid base was ensured by switching the arthroscope to an additional lateral transtendinous viewing portal through the supraspinatus tendon. 5
Subsequently, an incision was made over the ACJ in the orientation of the distal clavicle. Soft tissue impeding anatomic joint reduction (eg, discus articularis) was then removed. Consecutively, 2 horizontal tunnels were drilled through the distal clavicle and acromion, 10 to 15 mm on either side of the ACJ using a 2.4-mm cannulated drill. Via shuttle sutures (SutureLasso; Arthrex), a high-strength suture tape (FiberTape; Arthrex) was passed through the drill holes in a box configuration. 8 Now, anatomic reduction of the ACJ was performed, radiographically controlled, and temporarily transfixed using a trans-AC Kirschner wire.
Then, a second small skin incision was placed over the clavicle at the anatomic position of the trapezoid and conoid ligament approximately 3.5 cm medial to the ACJ line. An ACJ drill guide (Arthrex) was introduced via the anterolateral portal and a transclavicular-transcoracoid tunnel was established 3.5 cm medial to the ACJ line using a 2.4-mm cannulated drill, which is located between the attachments of the conoid and trapezoid ligaments. Using a shuttle wire, we shuttled the free strands of a looped high-strength suture tape retrograde through the coracoid and the clavicle via the anterior portal. The distal implant loops were attached to a titanium button (Dog Bone; Arthrex), and the button was positioned flush under the base of the coracoid process with the help of a grasper device. The proximal strands and loop of the suture tape were then threaded in a second titanium button (Dog Bone) on top of the clavicle. Next, the suture tapes were tightened and secured by alternating knots.
In a chronic situation, 4 the CC construct was biologically augmented using a gracilis tendon autograft, which was shuttled along with the suture tape construct and then recovered from superior by shuttling it laterally around the coracoid basis and transferring it superiorly parallel to the transcortical strand anterior to the clavicle. The ends of the autograft were then tied, and the knot was reinforced with multiple stitches of an absorbable suture. For graft passage, a 4-mm drill was used. Finally, the ACJ cerclage was fixed by alternating knots, with the knot placed posterior to the ACJ for less soft tissue irritation (Figure 1). 5
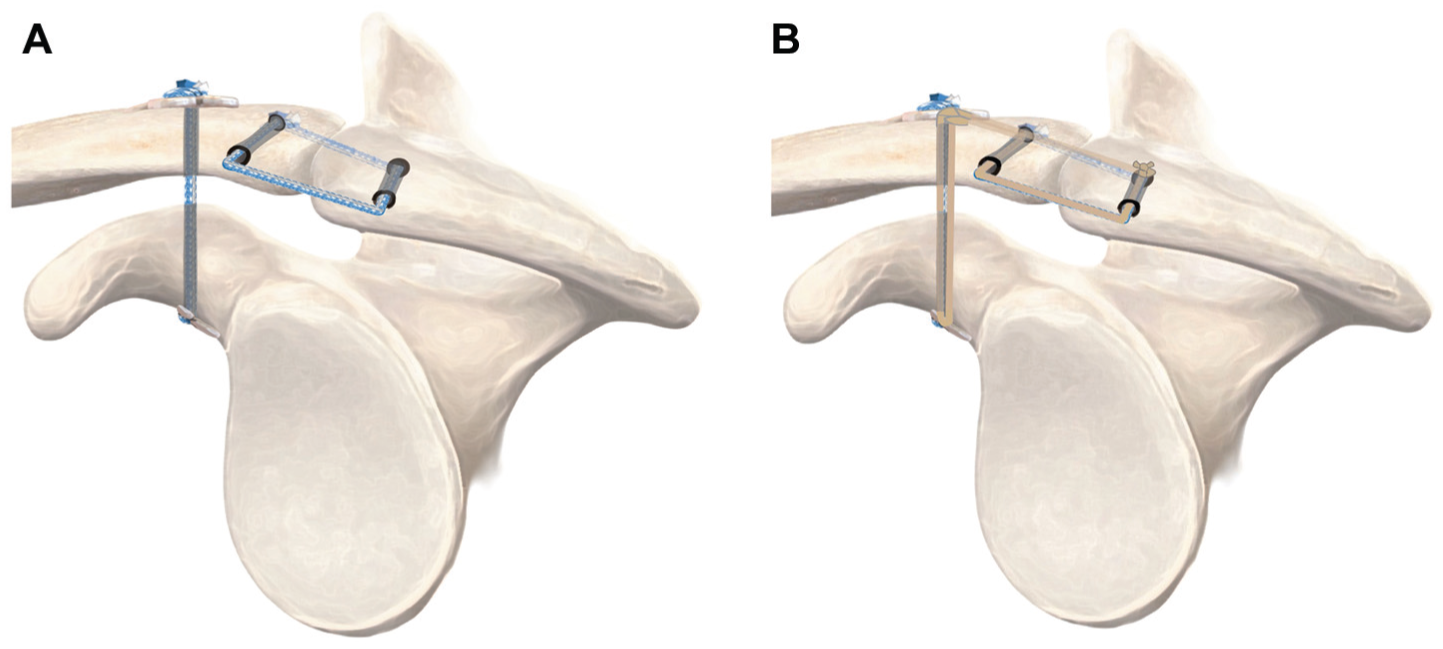
Schematic drawing of the sagittal perspective of the final construct after coracoclavicular (CC) and acromioclavicular (AC) stabilization via suspensory fixation in a right shoulder in the (A) acute and (B) chronic settings. For CC stabilization, a construct incorporating a suspensory fixation system consisting of high-strength suture tape and 2 titanium buttons is shuttled through a transclavicular and transcoracoid tunnel. In the chronic setting, the gracilis tendon autograft is shuttled cranially lateral of the coracoid and anterior of the clavicle and sutured to itself posterosuperior of the clavicle. For the AC stabilization, an AC cerclage consisting of a high-strength suture tape is passed through a horizontal transacromial and transclavicular tunnel and fixed in box configuration, placing the knot posterior to the acromioclavicular joint.
Postoperative Rehabilitation
The operated arm was immobilized in a sling for 6 weeks postoperatively. During the first 4 weeks postoperatively, only active-assisted range of motion (ROM) was allowed. In the first and second weeks, abduction/adduction and flexion/extension (30°/0°/0°) as well as internal/external rotation (80°/0°/15°) was allowed. ROM was increased in the third and fourth weeks to abduction/adduction and flexion/extension at 45°/0°/0° as well as internal/external rotation at 80°/0°/30°. In the fifth and sixth weeks, active ROM was allowed with abduction/adduction and flexion/extension at 60°/0°/0° as well as free internal/external rotation. Starting from 7 weeks postoperatively, free active ROM was permitted with return to full load-bearing capacity after 3 months.
Clinical Outcome Parameters
At a minimum follow-up of 2 years postoperatively, functional outcome measures were evaluated including the Constant-Murley (CM), American Shoulder and Elbow Surgeons (ASES), and Nottingham Clavicle (NC) scores as well as the visual analog scale (VAS) score for pain, which were compared between groups at the final follow-up.
In addition, the postoperative patients’ subjective satisfaction with the cosmetic appearance of the ACJ was evaluated using a 5-point Likert scale, stratified as “totally satisfied,”“very satisfied,”“moderately satisfied,”“slightly satisfied,” or “not at all satisfied.”
Statistical Analysis
Given that this was a retrospective analysis, the availability of data determined the sample size. A power analysis was performed to determine the capability of the sample size to detect a clinically meaningful difference of 17 points in ASES score. 17 Assuming a standard deviation of 20 points, a sample size of 23 patients would provide 80% power at an alpha level of .05, performed with G*Power (HHU Düsseldorf, Düsseldorf, Germany). 9
Descriptive statistics were used to summarize categorical and continuous variables, with categorical variables reported as counts and percentages, and continuous variables reported as mean ± standard deviation. The Shapiro-Wilk test was used to evaluate the distribution of continuous variables. Parametric tests (unpaired t test) or nonparametric tests (Mann-Whitney U test) were used to compare continuous variables between groups, depending on the respective distribution of the data. Categorical variables were compared using the binary Fisher exact test or chi-square test, as appropriate. Correlations were assessed using the Pearson or Spearman correlation coefficient where appropriate. Confidence intervals of 95% were calculated and a significance level of P < .05 was used. The statistical analysis was performed using SPSS software (Version 29.0; IBM).
Results
A total of 144 patients were assessed for eligibility after a review of the institutional database between January 2015 and August 2021. Of those, 82 patients (mean age at surgery, 40.3 ± 12.7 years; 54 acute and 28 chronic injuries) with a mean follow-up of 5.5 ± 2.0 years (range, 2.0-9.9 years) were included in the final analysis. A flowchart detailing the inclusion process for the acute and chronic groups is provided in Figure 2.

Flowchart visualizing the patient population of the acute and chronic groups after accounting for inclusion and exclusion criteria as well as those lost to follow-up. AC, acromioclavicular; ACJ, acromioclavicular joint; CC, coracoclavicular; LHBT, long head of the biceps tendon; ORIF, open reduction internal fixation.
There were no significant differences between groups regarding age at surgery (acute: 38.4 ± 12.2 years; chronic: 43.7 ± 13.2 years; P = .086), sex (female acute: 13.0%; female chronic: 14.3%; P = .87), or follow-up time (acute: 5.5 ± 1.8 years; chronic: 5.5 ± 2.5 years; P = .83). However, there was a significant difference in surgical time (acute: 89.7 ± 18.0 minutes; chronic: 111.2 ± 20.6 minutes; P < .001). Characteristics of the patient population are provided in Table 1.
Characteristics of the Study Groups a
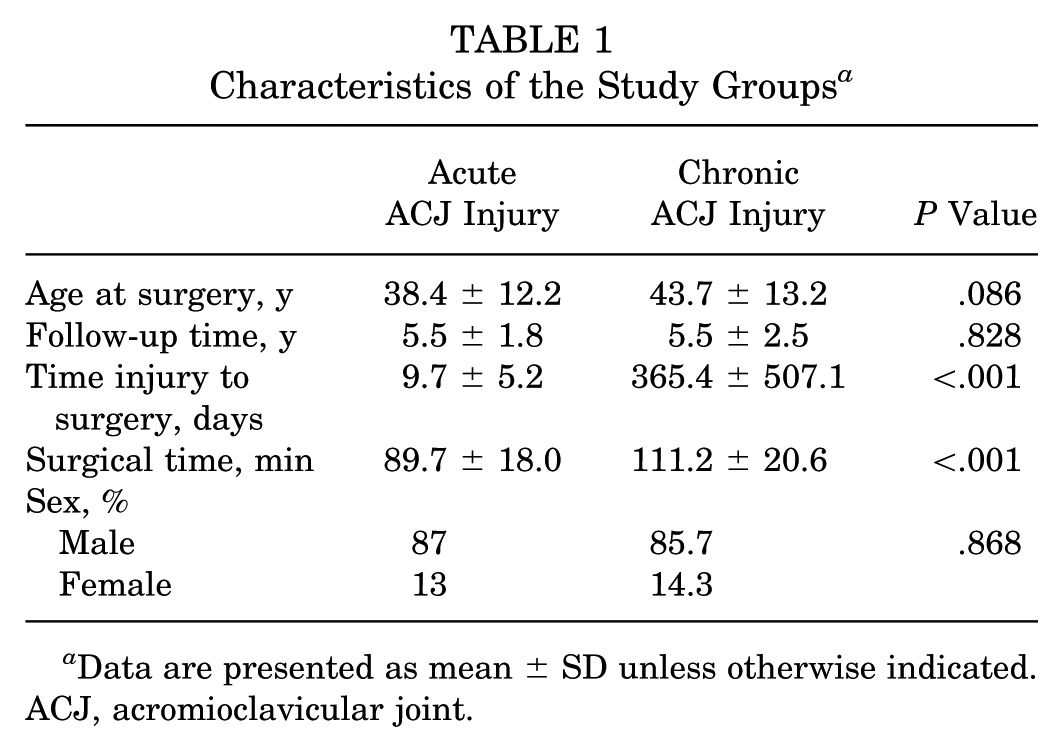
Data are presented as mean ± SD unless otherwise indicated. ACJ, acromioclavicular joint.
Clinical Outcomes
At the final follow-up, patients with acute or chronic injuries showed similar CM (acute: 85.3 ± 13.3; chronic: 85.5 ± 12.0; P = .98), ASES (acute: 94.3 ± 10.1; chronic: 93.5 ± 14.4; P = .69), and NC (acute: 85.6 ± 14.2; chronic: 86.8 ± 14.0; P = .68) scores (Table 2). Furthermore, there was no difference in VAS score for pain (acute: 1.9 ± 1.1; chronic: 2.0 ± 1.6; P = .47). Neither age at surgery nor follow-up time was correlated with any of the functional outcome scores (P > .05 for both).
Functional Outcome Measures a
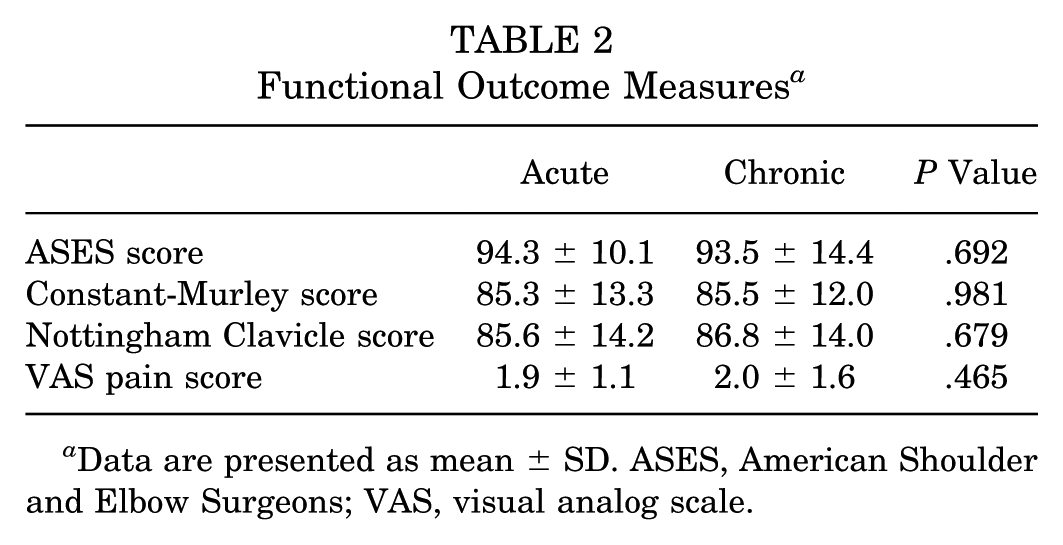
Data are presented as mean ± SD. ASES, American Shoulder and Elbow Surgeons; VAS, visual analog scale.
In terms of the postoperative patients’ subjective satisfaction with the cosmetic appearance of the ACJ, 28.6% were “totally satisfied,” 27.0% were “very satisfied,” 33.3% were “moderately satisfied,” 4.8% were “slightly satisfied,” and 6.3% were “not at all satisfied.” There was no significant difference in postoperative subjective satisfaction with the cosmetic appearance of the ACJ between acute and chronic ACJ injuries (P = .753) (Table 3).
Subjective Cosmetic Appearance of the ACJ a

Data are presented as percent. ACJ, acromioclavicular joint.
Complications and Revisions
Five patients in the acute group and 2 patients in the chronic group experienced failure, defined as loss of reduction along with clinical complaints, and underwent revision surgery (acute: 9.3%; chronic: 7.1%; P = .75). In the acute group, 2 of the patients showed immediate postoperative loss of reduction and underwent revision surgery after 2 and 4 days, respectively, using the same technique (CC suspensory fixation with an additional AC cerclage). Furthermore, 3 patients of the acute group had symptomatic loss of reduction during early follow-up. These patients underwent revision surgery after 5, 6, and 9 months, respectively, using CC suspensory fixation with an additional AC cerclage and biological augmentation (ipsilateral gracilis tendon autograft).
In the chronic group, 1 patient had immediate postoperative loss of reduction and underwent revision surgery after 4 days using the same technique along with renewed fixation of the gracilis tendon autograft. Another patient had recurrent ACJ instability along with suspicion of a low-grade infection, consequently undergoing implant removal 5 months after the index surgery as well as antibiotic therapy after evidence of Cutibacterium acnes.
Discussion
The most important finding of the study was that patients who underwent ACJ stabilization using CC suspensory fixation with an additional AC cerclage for isolated type 5 ACJ injuries in the acute setting achieved similar midterm functional outcomes and failure rates to those who underwent delayed surgery with additional biological augmentation using a gracilis autograft ≥3 weeks after injury. In addition, there was no significant difference in the subjective satisfaction with the postoperative cosmetic appearance of the ACJ between injuries treated in the acute and chronic settings. These data may serve as a reference point for shoulder surgeons in guiding discussions with their patients about the timing of surgical intervention within the context of personalized decision-making.
Current evidence still supports a surgical stabilization of high-grade ACJ injuries depending on the specific functional and cosmetic demands of the patient.2,10,14,15,20 While available evidence reports favorable and reliable postoperative outcomes after arthroscopically assisted ACJ stabilization,11,14,23,24 the surgical technique used depends on the chronicity of injury. More specifically, the ISAKOS Shoulder Committee recommends an additional biological augmentation using a tendon auto- or allograft in chronic ACJ injuries, defined as an interval from injury to surgery of >3 weeks. 3 Consequently, the urgency of surgical intervention is a critical factor in the shared decision-making process in patients with high-grade ACJ injuries. 3
However, evidence pertaining to comparative studies evaluating functional outcomes after ACJ stabilization in either the acute or chronic setting for high-grade ACJ injuries is highly limited.7,12 Furthermore, these previously published studies show inconsistent and rather conflicting results.7,12 More specifically, Dey Hazra et al 7 found a statistically significant superiority of early surgical stabilization (<3 weeks) for Rockwood type 3b and 5 ACJ injuries compared with delayed surgery (>3 weeks) in terms of functional scores at a mean follow-up of 3.2 years, which is contrary to the results of the present study. Importantly, it has to be considered that the mean differences, which were observed by Dey Hazra et al, 7 in the Constant score (4.0 points) and Taft score (0.9 points) lie far below the minimal clinically important difference. 22 Furthermore, those of the NC score (5.1 points) and ASES score (6.5 points) may also be of little clinical relevance, while there was no statistically significant difference in the Subjective Shoulder Value and VAS score for pain. 7 In addition, both the acute and chronic groups each comprised 18 type 3b and 15 type 5 injuries, resulting in a small subgroup sample size and limited statistical power. 7
Contrarily, Lädermann et al 12 observed that early (<2 weeks) and delayed (>2 weeks) surgical intervention resulted in equivalent clinical outcomes for type 3 to 5 ACJ injuries at a mean follow-up of 3.5 years, which is confirmed by the data of the present study. Again, this study included patients with heterogeneous severity of ACJ injuries (Rockwood types 3-5), with only 15 of 31 (48%) type 5 injuries in the acute group and 7 of 22 (32%) in the chronic group. 12 Furthermore, the authors used a 2-week cutoff to differentiate between early and delayed surgery, which is not common practice according to international guidelines.3,20 This clearly limits the validity and statistical robustness of the results and highlights the need for outcome studies with larger sample sizes, homogeneous patient collectives, and longer follow-up periods. Taking this into account, the results of the present study hold a greater statistical robustness given the larger homogeneous sample sizes of only patients with a type 5 ACJ injury and may have an effect on the shared decision-making process in patients with high-grade ACJ injuries.
In their study, Rupp et al 21 examined patients aged ≥50 years treated with the identical arthroscopically assisted AC and suspensory fixation used in the present study, applying an identical hamstring-tendon augmentation protocol for chronic cases. They likewise observed equivalence between acute (≤3 weeks) and chronic (>3 weeks) procedures in pain relief and core functional metrics (ASES, Quick Disabilities of the Arm, Shoulder and Hand, and VAS scores), mirroring the results of the present study. Of interest, their acute cohort showed a trend toward higher Single Assessment Numeric Evaluation scores and a return to a wider range of sports, hinting at a subtle functional advantage for early intervention despite overall parity in objective outcomes.
Of clinical importance, a recent study demonstrated that successful nonoperative treatment resulted in similar functional outcomes for acute type 5 ACJ injuries when compared with surgical stabilization. 1 Even though 15% of initially nonoperatively treated patients eventually required surgery, these findings clearly challenge the urgency of early surgical intervention in patients with high-grade ACJ injuries. 1 Considering the results of the present study, initial nonoperative treatment of acute high-grade ACJ injuries seems justifiable, as delayed surgery would achieve similar functional outcomes and cosmetic appearance of the ACJ to early intervention in those patients in whom the nonoperative approach fails. This is also supported by a recent study showing that patients with successful nonoperative treatment for type 3 to 5 ACJ injuries achieved similar clinical outcomes at a minimum 5-year follow-up to those who were converted to anatomic CC ligament reconstruction. 16 Although delayed surgery requires augmentation using a tendon graft and a longer surgical time due to tendon harvest and additional shuttle maneuvers, the equality of delayed surgery and early intervention is important when counseling patients regarding the urgency of surgery and managing their expectations.
In addition, it has to be acknowledged that operative treatment fails in some patients, with many subsequently requiring revision surgery. Even though the failure rates in the present study were similarly low in the acute (9.3%) and chronic (7.1%) groups, potential postoperative loss of reduction should be considered when giving treatment recommendations. Possible reasons for the immediate or early loss of reduction observed in the present study are manifold. Because in all the patients with failure the Dog Bone–FiberTape construct was intact and no fractures were observed, loss of reduction may be related to the patient not complying with the restrictions of the rehabilitation protocol or remaining slack in the suspensory system.
The study has several limitations. Although data were collected prospectively, the chart review was performed retrospectively. Consequently, the study inherits the associated biases of a retrospective design. However, the absence of preoperative baseline data may be negligible for a comparison of outcomes between the acute and chronic patient cohorts at the final follow-up, as acute and chronic injuries represent completely different types of injury. It is to be expected that patients with an acute injury have significantly poorer preoperative baseline values compared with patients with a chronic injury, who have already received nonoperative treatment. Second, the monocentric study design may limit the external validity of the results as surgery was performed in a single reference center for arthroscopic stabilization of ACJ injuries. Third, donor site morbidity from harvesting of the gracilis tendon (eg, hamstring strength and saphenous nerve injury) was not assessed in the chronic group. Finally, as the clinical outcome was elected as the primary endpoint of this study, a postoperative radiological evaluation at the final follow-up was not conducted. The decision was made not to expose patients to additional radiation, as previous studies did not reveal an association between radiological reduction and clinical findings after ACJ stabilization.6,17 Consequently, loss of radiographic reduction as well as the potential presence of iatrogenic fractures, tunnel widening, heterotopic ossifications, osteoarthritis, or osteolysis around the ACJ could not be evaluated.
Conclusion
Patients who underwent ACJ stabilization using CC suspensory fixation with an additional AC cerclage for isolated type 5 ACJ injuries in the acute setting achieved similar midterm functional outcomes, satisfaction with the cosmetic appearance of the ACJ, and failure rates to those who underwent delayed surgery with additional biological augmentation using a gracilis autograft ≥3 weeks after injury. These data may serve as a reference point for shoulder surgeons in guiding discussions with their patients about the timing of surgical intervention within the context of personalized decision-making.
Footnotes
Final version submitted December 5, 2025; accepted December 9, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S. is a consultant for Arthrex GmbH. S.S. is consultant for Arthrex GmbH, KLS Martin Group, and medi. M.C.R. has received payments/honoraria and support for attending meetings/travel/fellowships from Arthrex GmbH. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Technical University of Munich (2022-223-S-Np).