
Abstract
Background:
Patients with femoroacetabular impingement (FAI) frequently experience sacroiliac joint (SIJ) pain. Patients with concomitant lower back symptoms may be at risk for poor patient-reported outcomes after cam resection.
Purpose:
To investigate whether SIJ stress in patients with FAI changes depending on posture or cam resection.
Study Design:
Descriptive laboratory study.
Methods:
Preoperative and postoperative computed tomography (CT) scans were analyzed in 31 patients with FAI who underwent cam resection. We created CT models of the lumbar spine, pelvis, and hip joints, including the SIJ cartilage and surrounding ligaments. For both pre- and postoperative conditions, we constructed models of standing, sitting, and sitting with 10° posterior pelvic tilt positions and measured the equivalent stress in the anterior, superior-posterior, and inferior-posterior regions of the SIJ under a 600-N load.
Results:
Preoperatively, the equivalent stress in the posterior-inferior SIJ region was generally higher in the sitting than in the standing position (up to 2.87-fold, P < .0001), whereas there was no significant difference between standing and sitting with a 10° posterior pelvic tilt position. After cam resection, the equivalent stress in the lower portion of the SIJ during sitting generally decreased (P < .0001). A positive correlation was observed between the preoperative posterior-inferior SIJ equivalent stress in the sitting position and preoperative α angle (r = 0.40; 95% CI, 0.04-0.66).
Conclusion:
In patients with FAI, the equivalent stress in the lower portion of the SIJ generally increased in the sitting posture. Cam resection decreased the equivalent stress in the posterior-inferior SIJ region in the sitting posture to a level similar to that observed with a 10° posterior pelvic tilt before surgery.
Clinical Relevance:
These findings suggest that optimizing pelvic posture and appropriate cam resection may help mitigate SIJ-related pain in patients with FAI, providing valuable insights for surgical planning and rehabilitation strategies.
The concept of femoroacetabular impingement (FAI) was first systematically presented by Ganz et al 10 and is widely known as a risk factor for the progression of hip osteoarthritis. 36 Arthroscopic cam resection and labral repair are standard treatments for FAI, with favorable outcomes reported.20,22 However, studies indicate that patients with FAI who also have lower back pain tend to show poorer patient-reported outcomes (PROs) after hip arthroscopy than those without lower back pain. 21 Clinically, many patients with FAI indicate persistent pain in the sacroiliac joint (SIJ) region. Horner et al 13 reported that among patients with FAI, those with SIJ pain exhibited lower postoperative PRO scores and were less likely to achieve the minimal clinically important difference or patient acceptable symptom state (PASS). In their cohort of 2556 patients undergoing hip arthroscopy for FAI, 75 hips (approximately 2.9%) were identified as having SIJ pain based on clinical evaluation. However, because SIJ pain was not assessed systematically across all patients, this percentage may represent a conservative estimate of its true prevalence. Furthermore, 76% of patients with SIJ pain reportedly had radiographic findings associated with FAI, 17 and 25.2% of patients with FAI showed abnormalities of the SIJ on radiograph, computed tomography (CT), or magnetic resonance imaging (MRI). 24 Thus, SIJ pain is closely related to FAI in the lumbar-pelvic-femoral complex, and we assume that examining the stress changes in the SIJ could contribute to comprehensive treatment strategies for patients with FAI.
Finite element analysis (FEA), a numerical technique for analyzing mechanical loads in complex 3-dimensional structures, has been demonstrated to accurately replicate load deformation data in SIJ. 29 Previous studies used FEA to analyze the changes in SIJ stress before and after surgery in patients with acetabular dysplasia, 38 suggesting that hip joint pathology can influence SIJ stress. However, FEA-based studies on SIJ stress in patients are extremely limited. In FAI, particularly in cases of large cam deformity, hip impingement is more likely to occur during flexion. Additionally, hip joint motion may influence the pelvic rotation. 2 Furthermore, patients with SIJ pain often report greater pain in the sitting or stooped posture than while standing. 19 Hence, both the hip in flexion and a large cam deformity may contribute to increased SIJ stress.
Against this background, the following clinical questions arose: How do standing and sitting postures and changes in pelvic tilt affect SIJ stress in patients with FAI? How does SIJ stress change after cam resection? We addressed these clinical questions using FEA models based on surgically treated FAI cases, specifically focusing on how SIJ stress changes across different postures and determining the changes in SIJ stress before and after cam resection. To our knowledge, this is the first study to evaluate SIJ stress in patients with FAI using FEA. Elucidating these biomechanical changes may provide valuable insights for optimizing surgical strategies and rehabilitation approaches, potentially improving patient outcomes by reducing SIJ-related pain and dysfunction.
Methods
This study was designed as a retrospective case series. We retrospectively reviewed 40 consecutive patients who visited the Yokohama City University Medical Center between March 2021 and July 2023 and were diagnosed with FAI. The diagnostic criteria for FAI were in accordance with the Japanese Hip Society guidelines. For pincer-type FAI: (1) center-edge (CE) angle angle ≥40°, (2) CE angle ≥30° and acetabular roof obliquity ≤0°, or (3) CE angle ≥25° and a positive crossover sign. For cam-type FAI: CE angle ≥25° and α angle ≥55°. Patients who satisfied these radiographic criteria and experienced hip pain were diagnosed with FAI. Surgical intervention was indicated for patients who met the diagnostic criteria for FAI and showed resistance to at least 3 months of conservative treatment. The exclusion criteria were known hip and inflammatory diseases, calcifications, abnormal ossifications, bone tumors, gouty arthritis, hemochromatosis, and avascular necrosis of the femoral head. Nine patients who did not undergo CT imaging with the calibration phantom were excluded, leaving 31 patients (31 hips) for the final analysis. Table 1 presents the participants’ basic characteristics.
Patient Characteristics (N = 31) a

Values are presented as mean ± SD unless otherwise indicated.
All patients underwent arthroscopic hip surgery performed by 2 experienced surgeons (N.K. and Y.Y.). The surgeries were performed in the supine position on a traction table. Traction was applied during the central compartment procedure, and under fluoroscopic guidance, an anterolateral portal was created, followed by the formation of a midanterior portal. Labral repair was completed using 2 or 3 suture anchors, and acetabular rim trimming was performed for pincer lesions. After procedures for the central compartment, traction was released, and the cam lesion was visualized. The cam lesion was resected in each case as appropriate.
To minimize selection bias, all consecutive patients who met the inclusion criteria during the study period were included. This study was approved by the institutional review board, and informed consent was obtained using an opt-out approach, allowing participants the opportunity to decline participation. Patient enrollment and 3-dimensional model reconstruction were conducted between July and October 2024.
The 3D models of the sacrum, pelvis, and femur were reconstructed using Mechanical Finder version 13.0 (Materialise). The cortical and cancellous bones were separated, and tetrahedral elements with 10 nodes each were used to create the mesh. The SIJ cartilage was reconstructed from the CT images. The ligaments surrounding the SIJ, such as the anterior sacroiliac, long posterior sacroiliac, short posterior sacroiliac, interosseous sacroiliac, sacrospinous, and sacrotuberous ligaments, were modeled as 3D tension-only truss elements (Figure 1).
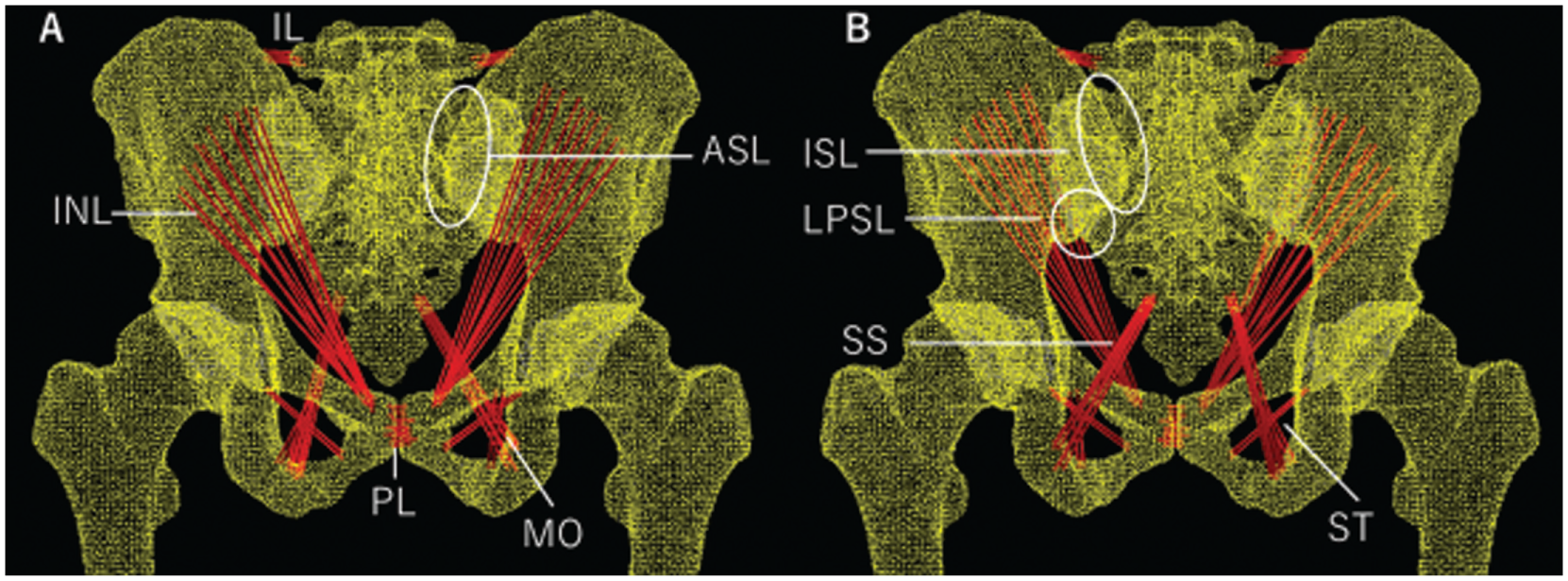
Lumbopelvic-femur model. (A) Anterior view of pelvis. (B) Posterior view of pelvis. ASL, anterior sacroiliac ligament; IL, iliolumbar ligament; INL, inguinal ligament; ISL, interosseous sacroiliac ligament; LPSL, long posterior sacroiliac ligament; MO, obturator membrane; PL, pubic ligament; PSL, posterior sacroiliac ligament; SS, sacrospinous ligament; ST, sacrotuberous ligament.
The attachment area of each ligament was reproduced as described by Kim et al. 15 Young's modulus of the bone was set to 11,000 MPa with a Poisson's ratio of 0.2, and Young's modulus for the SIJ cartilage was set to 4.1 MPa with a Poisson's ratio of 0.2. The material properties of the pelvic ligaments were reproduced as described in a previous report. 38
We assessed 3 conditions as follows. Standing: the distal femur was fixed with the anterior pelvic plane at 0°. Sitting: the hip was flexed to 90°, and the distal ischial region was fixed from the posterior aspect of the femur. Sitting with a 10° posterior pelvic tilt: the hip was flexed to 80°, and the distal ischial region was similarly fixed (Figure 2).

Loading conditions in each posture. (A) Standing. (B) Sitting. (C) Sitting with 10° posterior pelvic tilt.
Under all conditions, a compressive load of 600 N was applied to the L5 vertebra to simulate static loading. If impingement between the femur and pelvis occurred at an angle <90° of hip flexion, a compressive load was applied at that specific angle.
Following Poilliot et al, 28 the SIJ cartilage was divided into 3 compartments: anterior, posterior-superior, and posterior-inferior (Figure 3).

The 3 compartments of the sacroiliac joint: (A) anterior section, (B) superior-posterior section, and (C) inferior-posterior section.
The equivalent stress in each compartment was measured under the 3 loading conditions.
We used the CE angle, acetabular roof obliquity (ARO), and α angle as hip joint parameters. The CE angle and ARO were measured on the anteroposterior radiograph, and the α angle was measured on the 45° Dunn view. Descriptive statistics were calculated for continuous variables using means and standard deviations. We examined the changes in SIJ equivalent stress across different postures using repeated-measures analysis of variance, followed by t tests for post hoc multiple comparisons. Pearson's correlation coefficient was used to analyze the correlations between the radiographic parameters and SIJ stress in each region. Pre- and postoperative changes were evaluated using paired t tests. The significance level was set at 5%. Statistical analyses were performed using JMP PRO version 15 (SAS Institute). There were no missing data in this study.
Results
In 2 of the 31 hips, impingement occurred at angles <90° (85° and 82°), and sitting models were constructed based on these angles. The 10° posterior pelvic tilt simulation was successfully performed in all cases. Among the 31 cases, 28 showed an increase in the posterior-inferior SIJ equivalent stress in the sitting posture compared with the standing posture. Preoperative posterior-inferior SIJ equivalent stress values were 2.23 ± 1.26 MPa in standing, 6.42 ± 5.28 MPa in sitting, and 2.23 ± 1.49 MPa in the 10° posterior pelvic tilt sitting postures (Figure 4).

Preoperative equivalent stress in the inferior-posterior region of the sacroiliac joint by posture.
The posterior-inferior SIJ equivalent stress in the sitting posture was higher than that in the standing posture (P < .0001). No significant changes in posture were observed in the anterior or posterior-superior compartments.
A positive correlation was observed between the preoperative posterior-inferior SIJ equivalent stress in the sitting position and preoperative α angle (r = 0.40; 95% CI, 0.04-0.66; P = .0294), indicating that a larger α angle tended to accompany a greater rise in posterior-inferior SIJ stress under sitting conditions (Figure 5).

Relationship between preoperative sitting posterior-inferior sacroiliac joint stress and preoperative α angle.
No other radiographic parameters showed a statistically significant correlation with SIJ stress in any compartment, and SIJ stress did not differ according to the type of deformity (cam, pincer, or mixed).
Postoperatively, the α angle generally decreased from 68.0°± 9.2° to 42.5°± 5.4° (P < .0001). In 24 of the 31 hips, the posterior-inferior SIJ equivalent stress decreased in the sitting posture. Compared with the preoperative sitting posture, the posterior-inferior SIJ equivalent stress in the sitting and 10° posterior pelvic tilt sitting posture after surgery was generally lower (P < .0001) (Figure 6).

Changes in the inferior-posterior sacroiliac joint equivalent stress before and after surgery.
In the remaining 7 hips, the posterior-inferior SIJ equivalent stress did not decrease postoperatively. There were no significant differences in patient demographics or radiographic parameters between these 7 cases and those showing a decrease in stress. No clear trends were observed in the anterior or posterior-superior compartments before and after surgery (Table 2).
Stress Distribution in Each Region of the Sacroiliac Joint a
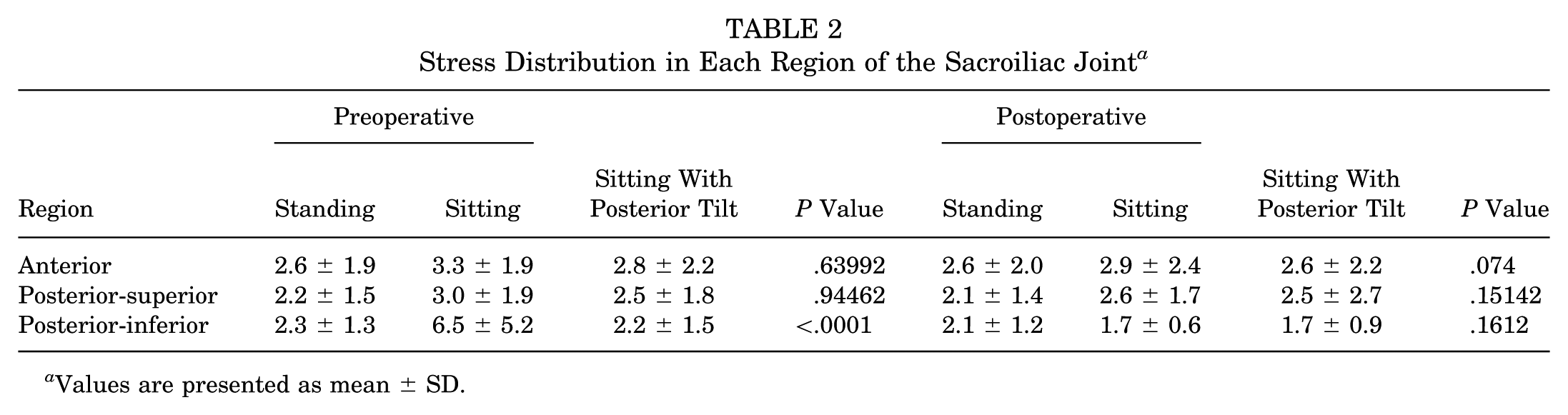
Values are presented as mean ± SD.
There was a positive correlation between the posterior and inferior SIJ equivalent stress in the preoperative 10° posterior pelvic tilt sitting posture and postoperative sitting posture (r = 0.57; 95% CI, 0.24-0.79; P = .00224).
Discussion
This study demonstrated that in patients with FAI, changes in posture generally affect the stress distribution in the posterior-inferior region of the SIJ, and cam resection also influences the equivalent stress in this region. Specifically, we found that preoperatively, the equivalent stress in the lower portion of the SIJ was approximately 3 times higher in the sitting than in the standing position; however, tilting the pelvis 10° posteriorly in the sitting posture reduced this stress to a level comparable with that in the standing position. Furthermore, cam resection lowered the equivalent stress in the posterior-inferior SIJ in the sitting posture to a level similar to that observed with a 10° posterior pelvic tilt before surgery. These quantitative results provide potentially important evidence of the association and clinical significance of FAI in SIJ disorders.
Clinically, patients with FAI often report SIJ region pain. 17 A recent systematic review indicated that SIJ dysfunction was present in 32.39% of athletes with low back pain, and stress-related injuries were identified as a potential risk factor. 23 A ligament injury model simulating SIJ dysfunction has been reported to increase SIJ stress by up to 43.6% compared with a healthy model. This finding supports the notion that elevated SIJ stress is associated with SIJ pain. 40 In athletes with FAI, lower back pain, SIJ pain, and sports hernia have been reported, indicating that problems may arise around the trunk region outside the groin region. 39 Cam-type impingement has been shown to increase the rotational motion at the pubic symphysis, 2 suggesting that kinematic changes may occur not only in the hip but also in the pelvic girdle and lumbar spine. This concept is known as the hip-spine syndrome, 25 and combined rehabilitation targeting both the hip and lumbar spine is reportedly effective for pain relief. 5 Pain in the SIJ region can stem from multiple sources, including the spine, hip, or primary SIJ, 8 making accurate differentiation crucial. Radiographic parameters associated with SIJ pain, such as SIJ, 37 sacral slope, and pelvic tilt, 34 have been documented. However, these parameters generally vary among individuals and cannot be easily standardized. 4 Additionally, the complex anatomy of the SIJ makes direct measurement of the intra-articular stress problematic. Therefore, we employed a 3D FEA approach to quantify SIJ stress in different postures in patients with FAI. We believe that the FEA approach is one of the most promising means of solving problems related to the lumbar-pelvic-femoral complex.
Kurosawa et al 19 advocated a scoring system for diagnosing SIJ pain that includes pain while sitting as one of its components. Additionally, SIJ pain is generally assessed by administering a block injection into the lower portion of the joint; therefore, our analysis first focused on the sitting posture and posterior-inferior region. The finding that the equivalent stress in the posterior-inferior SIJ increases during sitting is consistent with the clinical symptoms defined by Kurosawa et al. 19 In this study, the preoperative sitting posture showed a generally higher equivalent stress in the lower portion of the SIJ than that in the standing posture. Per previous reports, patients with SIJ pain have generally increased subchondral bone density in the lower portion of the SIJ, potentially due to prolonged stress loading. 27 The SIJ stress varies with posture,1,30 and reduced joint motion can alter the cartilage stress distribution. 33 In patients with FAI, rotational motion at the pubic symphysis is increased, 2 suggesting that rotational motion may also be elevated at the SIJ surface. As increased SIJ motion increases the intra-articular stress, 9 it is plausible that SIJ stress is heightened in the sitting posture of patients with FAI. Furthermore, a 10° posterior pelvic tilt was found to reduce posterior-inferior SIJ stress to a level comparable with that during standing. Kobayashi et al 16 reported that tilting the pelvis posteriorly by 10° could achieve hip range of motion improvements comparable with those obtained with cam resection. Based on these findings, the posterior pelvic tilt may play a critical role in addressing FAI-related issues.
As previously reported, a postoperative α angle <55° is associated with favorable outcomes, 7 and an α angle <55° yields good results without affecting 5-year outcomes. 3 In this study, the postoperative α angle was approximately 42.5°, suggesting that cam resection was performed adequately. Additionally, improvements in the Oswestry Disability Index, a measure of lower back symptoms, have been documented following cam resection, 35 indicating that addressing impingement can be beneficial for patients with lower back symptoms. SIJ disorders are among the causes of lower back symptoms, 11 and changes in sitting SIJ stress after cam resection may reflect the mechanism of pain relief. In this study, we confirmed that the equivalent stress in the lower portion of the SIJ during sitting generally decreased after cam resection. We hypothesized that cam resection may reduce compensatory SIJ rotation during hip flexion, thereby decreasing joint stress. Postoperatively, the stress in the posterior-inferior region of the SIJ while sitting was positively correlated with the α angle. Therefore, if a patient with FAI with a large α angle reports SIJ pain, cam resection may potentially improve the SIJ pain effectively, especially given that cam deformity has been observed in approximately 33% of patients with SIJ pain, 24 suggesting a possible biomechanical association between hip morphology and SIJ pathology.
Postoperative rehabilitation programs for FAI are typically divided into 4 phases: (1) protection of the joint, (2) return to full weightbearing, (3) return to preinjury function, and (4) return to running and sports, 18 as well as including exercises aimed at improving the hip function and core muscle strength. However, SIJ pain can persist even after FAI surgery,13,17,24 necessitating supplemental rehabilitation interventions tailored to each patient's condition. Sasaki et al 31 proposed a fundamental physical therapy approach for SIJ pain that comprised (1) stabilizing the SIJ using a pelvic belt and exercises targeting the transverse abdominis and gluteus maximus and (2) ensuring adequate mobility of the spine and hip joints. Jellad et al 14 reported the benefits of gluteal muscle stretching in patients with SIJ pain, suggesting the potential effectiveness of hip-focused exercises. In postures requiring hip flexion, enhancing the range of motion in both the pelvis (hip) and lumbar spine may help reduce SIJ stress. Also, training to consciously induce posterior pelvic tilt, core training, 32 and exercises using a balance disc 26 could help enhance the posterior pelvic tilt during movement, suggesting that these approaches could help alleviate SIJ stress in patients with FAI through rehabilitation. From the perspective of athletic performance, anterior pelvic tilt may offer functional advantages. A study of sprinters demonstrated a positive correlation between maximal running speed and anterior pelvic tilt, suggesting that anterior tilt may be required depending on the specific physical demands of the sport. 6 In our study, posterior pelvic tilt no longer reduced SIJ stress after cam resection. Therefore, in cases where anterior pelvic tilt is essential for sport-specific movements, cam resection may be particularly beneficial. We quantitatively demonstrated that the SIJ stress was generally affected by postural changes and cam resection in patients with FAI. Further research is needed to determine how physical therapy affects SIJ stress and identify more effective physical therapies.
Limitations
This study had some limitations. This was a retrospective case series and did not directly evaluate SIJ symptoms. Therefore, the relationship between changes in SIJ stress and symptom relief remains unclear. As the study targeted only patients with FAI, it remains unknown whether the posterior-inferior SIJ stress differs in healthy individuals. Additionally, although the 3D models were based on supine CT images, the actual pelvic tilt under true standing conditions may differ. To address this limitation, future studies should incorporate patient-specific motion and posture data using wearable sensors to simulate dynamic conditions more accurately. Integrating such motion data with finite element modeling may enable more realistic analyses of SIJ stress during functional activities.
In 7 cases, the posterior-inferior SIJ stress did not decrease postoperatively. There were no significant differences in patient demographics or radiographic parameters between these cases and those showing a postoperative decrease in SIJ stress. Given the complex 3D morphology of the SIJ, future studies should incorporate 3D morphologic analyses of the pelvis and hip joint. Statistical shape modeling has been reported as a useful approach for evaluating such 3D parameters 12 and may help clarify the mechanisms underlying residual SIJ stress in certain patients.
Conclusion
Using FEA, we investigated the effects of postural changes and cam resection on SIJ stress in patients with FAI. The sitting posture generally increased the posterior-inferior SIJ stress compared with standing, yet tilting the pelvis 10° posteriorly reduced it to a level generally not different from standing. The degree of stress increase in the sitting position positively correlated with the α angle. After cam resection, the posterior-inferior SIJ stress in the sitting position generally declined. These findings suggest that physical therapy focusing on the pelvic tilt or adequate cam resection may reasonably resolve SIJ pain in patients with FAI.
Footnotes
Final revision submitted October 16, 2025; accepted December 11, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by funding from the Yokohama Foundation for Advancement of Medical Science. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.