
Abstract
Background:
Proximal tibiofibular joint (PTFJ) instability is a relatively rare clinical condition, and the establishment of an evidence-based standard of care remains an ongoing challenge because of its low incidence in the literature. Current reports in the literature focus on isolated PTFJ reconstruction, and there remains to be any report on outcomes of PTFJ reconstruction performed concurrently with procedures for associated knee injuries, such as lateral collateral ligament (LCL) insufficiency coupled with tibiofibular instability.
Purpose:
To assess subjective and clinical outcomes after combined reconstruction of the LCL and PTFJ utilizing a semitendinosus allograft in the setting of anterior PTFJ instability and concomitant knee injuries requiring additional procedures.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review was conducted on consecutive patients who underwent anatomic PTFJ reconstruction utilizing a semitendinosus allograft from 2016 to 2021, with a ≥2-year follow-up. Exclusion criteria included ipsilateral concomitant lower extremity fracture, prior knee surgery, previous diagnosis of connective tissue disorder, and postoperative follow-up <2 years. Clinical outcomes were measured by PROs (return to function, return to play, International Knee Documentation Committee [IKDC], Single Assessment Numeric Evaluation score, Lysholm score, 12-item Short Form Health Survey, and range of motion), radiographic parameters, and subjective outcome measures obtained through a retrospective chart review, as well as a patient outcomes questionnaire.
Results:
Between August 2016 and November 2021, 29 patients underwent combined PTFJ and LCL reconstruction by the senior author. Of these, 25 patients (86%) met inclusion criteria and had a mean follow-up of 4.3 ± 2.1 years. Concomitant procedures were performed in 20 patients (80%), including anterior cruciate ligament reconstruction (48%), PCL reconstruction or repair (12%), and meniscal procedures (52%). Significant improvements were observed in patient-reported outcome measures, including the Lysholm score (preoperatively: median, 49 [IQR, 30-56]; follow-up: median, 95 [IQR, 76-95]; P < .001), IKDC (preoperatively: median, 34 [IQR, 18-54]; follow-up: median, 83 [IQR, 72-95]; P < .001), and Western Ontario and McMaster Universities Osteoarthritis Index total score (preoperatively: median, 36 [IQR, 21-49]; follow-up: median, 2 [IQR, 0-7]; P < .001). No patients required revision surgery related to the combined reconstruction. Sporting activity level remained high at follow-up (Tegner Activity Scale: median, 6.0 [IQR, 3.0-7.0]).
Conclusion:
Favorable outcomes can be expected after combined LCL and PTFJ reconstruction utilizing a semitendinosus allograft, even when performed alongside other procedures for concomitant injuries.
Keywords
Instability of the proximal tibiofibular joint (PTFJ) is a rare condition, with only 96 cases reported in the literature as of a 2017 systematic review. 11 Thus, a robust evidence-based standard of care remains to be established for PTFJ instability injuries.11,15,19 First-line treatment generally consists of conservative treatment with closed reduction and immobilization, with persistent and severe symptoms treated with surgical intervention. While conservative treatment for PTFJ injuries can be successful in resolving symptoms, the rate of persistent symptoms necessitating operative intervention remains high in literature.11,19 Surgical treatment of PTFJ injuries, specifically anatomic graft reconstruction and biceps tendon rerouting, has been found to improve outcomes with reduced complications, while fixation and fibular head resection were found to have higher rates of complication. 11
With the low incidence of PTFJ instability reported in literature, evaluating both long- and short-term outcomes of surgical intervention remain valuable for determining the efficacy of varying treatment methods. Current literature primarily evaluated outcomes of PTFJ instability treatment using patient-reported outcomes (PROs), subjective and objective clinical outcomes, and radiographic and other imaging modalities. ‖
This study is designed to be a retrospective chart review of patients who have undergone PTFJ reconstruction from 2016 to 2021 by a single surgeon (M.T.P.). The goal of the study is to evaluate the radiographic and clinical outcomes of PTFJ reconstruction utilizing a semitendinosus allograft. It is hypothesized that anatomic reconstruction of the PTFJ will result in improved subjective and objective clinical outcomes and high patient satisfaction with outcome.
Methods
This retrospective review was conducted following approval from the institutional review board. All patients who underwent combined PTFJ and lateral collateral ligament (LCL) reconstruction by the senior author (M.T.P.) between August 2016 and November 2021 were eligible for inclusion after a minimum follow-up of 24 months.
Operative Indications
Combined PTFJ and varus instability was diagnosed via physical examination in all patients. Patients generally complained of pain and/or instability symptoms in the lateral side of the knee. They were unable to compete in cutting sports and rotational leg activities. A physical examination confirmed anterior PTFJ instability by comparing the injured with the noninjured limb. With the patient supine on the examination table, the knee was placed in 90° of flexion and the hamstring tendon relaxed. The PTFJ was assessed by putting an index finger and thumb around the proximal fibula and shucking the fibula anterior and posterior. The fibula is almost always unstable in an anterior direction and if it is unstable, this anterior translation difference is assessed side to side. The typical amount of anterior translation for these patients from a side-to-side difference based on clinical examination was approximately 5 mm but could range up to 9 to 10 mm. Patients were also tested for rotatory instability, and those with high-grade posterolateral rotatory instability were excluded.
A series of bilateral knee radiographs was obtained on all patients. This included a hip-to-ankle image to assess overall alignment, bilateral extension weightbearing view, bilateral flexion posteroanterior (PA) view, a flexion lateral view, and a varus stress radiograph.
The PTFJ was assessed on the standing anteroposterior (AP), bilateral imaging plate, as well as a flexion posteroanterior (PA) view. The position of the fibula was assessed relative to the tibia, and what we termed “fibular splay” or “lateral distraction” from the tibia was measured on a weightbearing AP radiograph. To measure fibular splay, a line parallel to the joint starting at the most lateral aspect of the fibular head to the lateral tibia was drawn on both the affected and the unaffected side. The amount of splay was measured and documented, with side-to-side differences between the affected and unaffected knee being used as an indicator of PTFJ instability. Generally, this difference could be between 1 and 3 mm of the fibular diastasis from the tibia laterally to support the diagnosis of PTFJ instability (Figure 1). Accordingly, we treated fibular splay as a supportive, not determinative, finding.

This is a knee anteroposterior bilateral weightbearing radiograph showing the fibular splay sign. To measure fibular splay, a line parallel to the joint starting at the most lateral aspect of the fibular head to the lateral tibia is drawn on both the affected and the unaffected side. This image shows side-to-side differences of the fibular diastasis from the tibia laterally, indicating proximal tibiofibular joint instability.
The femorotibial angle was also assessed on preoperative weightbearing radiographs to evaluate coronal plane alignment and determine whether varus deformity contributed to lateral-sided knee instability. Varus stress radiographs were specifically used to evaluate for LCL incompetence, with 2.5 to 4.0 mm of increased lateral gapping compared with the contralateral side considered indicative of LCL incompetence. These findings informed operative decision-making and helped guide the decision to perform simultaneous LCL reconstruction.
Final diagnosis relied on patient history and reproducible provocative examination, with imaging used to corroborate instability and to exclude common mimics. Surgery was indicated in patients that had failed at least 4 to 6 months of nonoperative care including lateral stabilizing (LCL) bracing, physical therapy, Kinesio taping, band-strengthening exercises, and posterior/kinetic chain exercises. If they had persistent symptoms that kept them from performing their activities (which were typically cutting and rotational sports), surgery was offered to those patients. Concomitant ligamentous injuries were not subjected to additional nonoperative delay and, when indicated, were addressed at the index procedure. Operative intervention was also considered for patients with common peroneal nerve irritation.
Patient Setup and Approach
The patient was placed in the supine position with a lateral post under general anesthesia. Both limbs were examined to demonstrate the laxity in the PTFJ and the LCL. Anatomic landmarks were identified and marked, including the fibular head, Gerdy tubercle, the lateral epicondyle, and the lateral joint line. With the knee at 90° of flexion, a curvilinear incision was made from the lateral epicondyle to a point intersecting the fibular head and Gerdy tubercle. Full-thickness flaps were created and exposed the underlying iliotibial band (ITB) and biceps femoris. The common peroneal nerve (CPN) was identified and neurolysis was performed (Figure 2).
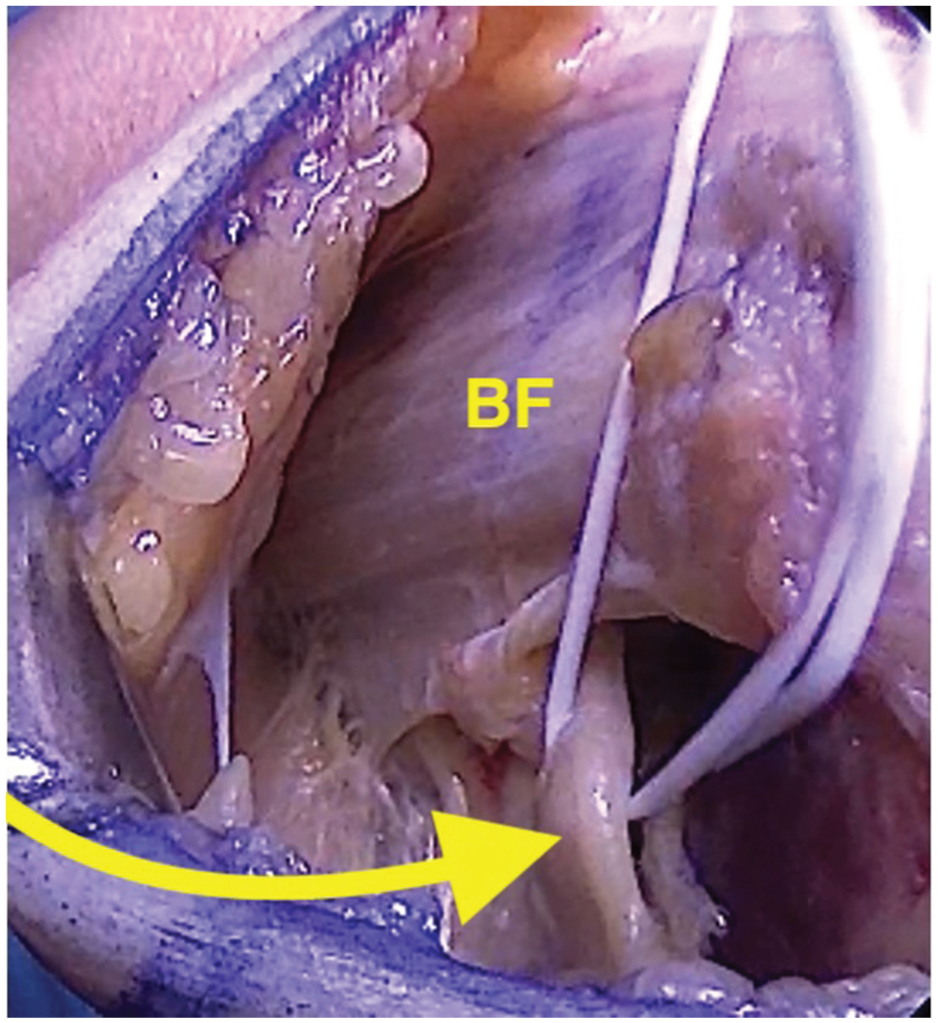
The common peroneal nerve is identified (yellow arrow) at the level of the fibular neck and deep/posterior to the biceps femoris (BF).
A second interval between the ITB and biceps femoris was created and the LCL was found and tagged. Pulling on the tagging stitch allowed easier identification of the LCL origin, which was on average 1.4 mm proximal and 3.1 mm posterior to the lateral epicondyle. 8 A 2-cm incision was made in the ITB to expose the femoral origin, where a Beath pin was placed and overreamed to 30 mm before shuttling a passing stitch (Figure 3).

(A) The femoral origin of the lateral collateral ligament (LCL; black arrow) is identified by splitting the iliotibial band (ITB) and pulling on the LCL tagging stitch. (B) A Beath pin is passed through the origin, aiming anteromedial and out of the medial skin. (C) A 6-mm reamer is used over the guide pin to a depth of 30 mm. (D) A passing stitch is shuttled through the femoral tunnel for later graft passage.
The LCL insertion was then identified and marked on the proximal fibular head, which was on average 8.2 mm posterior to the anterior border of the fibula and 28.4 mm distal from the fibular styloid. 8 Next, the lateral head of the gastrocnemius was bluntly elevated off the posterolateral fibular head, taking care to avoid injury to the CPN and posterior neurovascular bundle. A window was created by blunt dissection to palpate the posterior PTFJ and the posterior tibial metaphysis. From the LCL insertion, a 2.4-mm guide pin was drilled posteromedially, followed by a 6-mm reamer to create a fibular tunnel. A passing stitch was shuttled through, and a sub-ITB/biceps femoris tunnel was created toward the femoral origin for a third passing stitch (Figure 4).
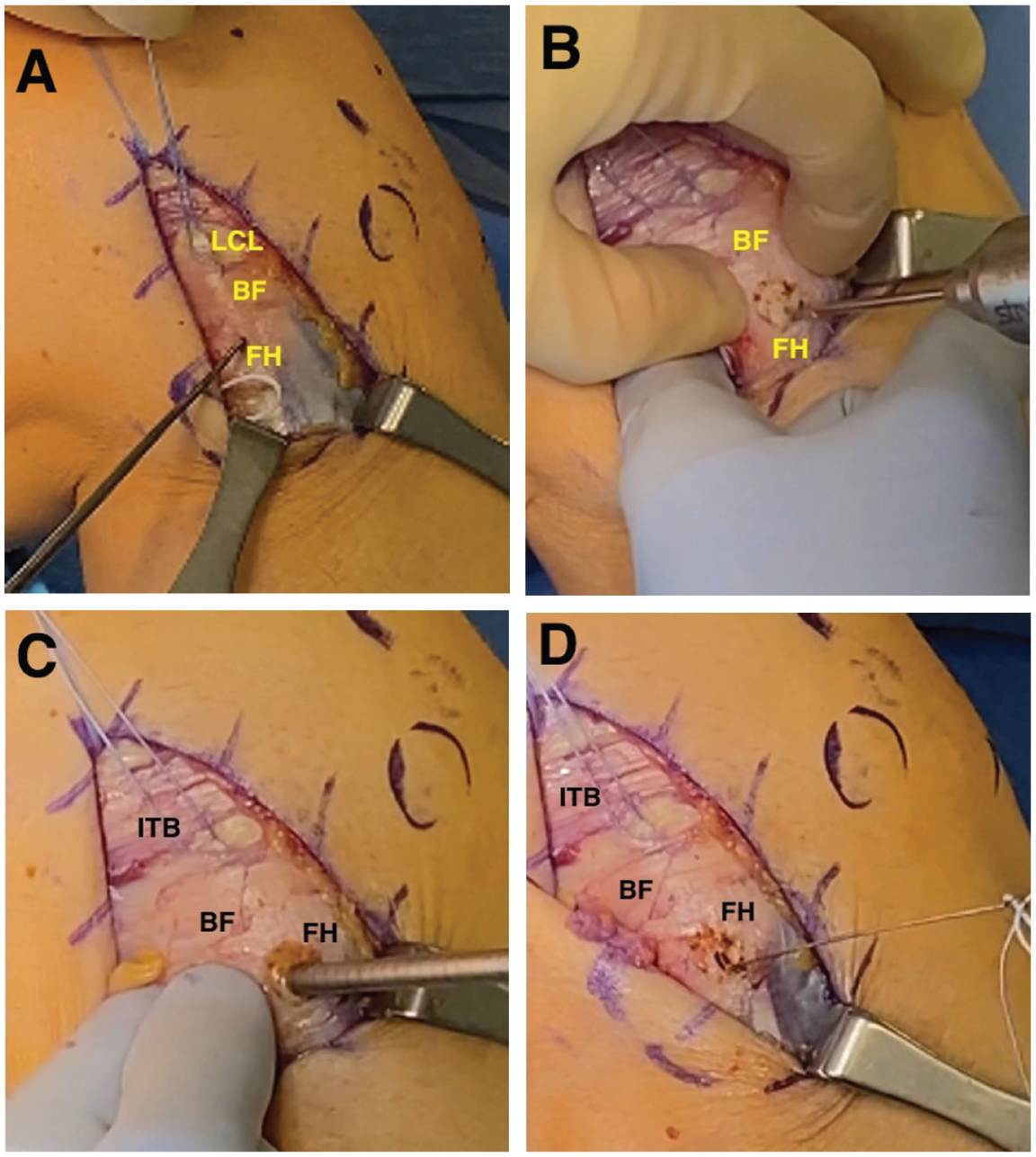
(A) The lateral collateral ligament (LCL) insertion on the fibular head (FH) as it traverses under the biceps femoris (BF) is identified by pulling on the traction suture. (B) A guide pin is passed in a posteromedial direction through the FH. (C) A 6-mm reamer is drilled bicortically through the FH. (D) A passing wire is used to shuttle a passing suture through the FH for later graft passage. ITB, iliotibial band.
Next, attention was turned to the PTFJ reconstruction. The Gerdy tubercle was identified, and a guide pin was placed in the AP position aiming toward the lateral tibial metaphyseal flare just medial to the PTFJ. This tunnel was reamed to 6 mm, and a wire suture-passing device was used to pass the last passing stitch so the graft could be passed from posterior to anterior in this tunnel (Figure 5).

(A) Gerdy's tubercle (GT) is identified and marked (yellow arrow); ITB, iliotibial band. (B) A guide pin (yellow arrow) is passed parallel to the tibial slope from Gerdy's tubercle to the tibial aspect of the proximal tibiofibular joint posteriorly using a window behind the fibular head. A Chandler retractor or Hohmann retractor can be used to palpate the landmark during drilling and to provide protection to the posterior knee structures; ITB, iliotibial band; LCL, lateral collateral ligament, arrow points to Gerdy's tubercle. (C) The tibial tunnel is created by reaming bicortically over the wire; ITB, iliotibial band; LCL, lateral collateral ligament; GT, Gerdy's tubercle. (D) A passing wire is used to shuttle a passing suture through the tibial tunnel for later graft passage; ITB, iliotibial band; LCL, lateral collateral ligament; GT, Gerdy's tubercle.
A semitendinosus allograft was prepared using a No. 2 nonabsorbable Krakow stitch (Arthrex) on both ends. It was first docked in the LCL femoral tunnel and secured with a 7 × 23–mm polyether ether ketone (PEEK) interference screw, then passed under the ITB and biceps femoris toward the fibular head. The graft was shuttled through the fibular tunnel from anterolateral to posteromedial and fixed with a second 7 x 23–mm PEEK screw with the knee at 70° of flexion with slight internal rotation of the tibia and a valgus stress on the knee, completing the LCL reconstruction.
To complete the PTFJ reconstruction, the remaining posterior graft was passed posterior to anterior through the tibial tunnel and secured with an 8 × 30–mm biocomposite screw with the knee at 20° to 30° of flexion (Figure 6).

(A) A semitendinosus allograft is docked in the femoral tunnel and an interference screw is inserted while holding the graft in the trajectory of the native lateral collateral ligament. (B) The graft is shuttled under the iliotibial band (ITB) and biceps femoris (BF) to the anterolateral fibular head (FH), and then through the FH from anterior to posterior. An interference screw is inserted in the FH to complete the lateral collateral ligament reconstruction. (C) The graft is then shuttled from posterior to anterior through the tibial tunnel and fixated with an interference screw for the proximal tibiofibular joint reconstruction. GT, Gerdy tubercle.
The ITB was closed using interrupted No. 0 Vicryl suture (Ethicon) followed by layered closure of the subdermal and subcuticular layers.
Rehabilitation
The patient is restricted to toe-touch weightbearing and 0° to 90° range of motion in a knee brace for 4 to 6 weeks postoperatively. Light strengthening and mobility exercises are used for the first 12 weeks followed by more progressive strengthening and sports-specific training with expected return to play by 8 to 9 months.
Patient Characteristics and Operative Data
Chart review was performed to collect demographic, injury- and surgery-related data. Preoperative AP whole-leg weightbearing radiographs were analyzed with regard to the femorotibial angle, grade of osteoarthritis (OA) (according to Kellgren-Lawrence) 9 and fibular splay. The Kellgren-Lawrence grade was determined as the worst score in any compartment, with a scale from grade 1 (no OA) to grade 4 (severe OA). All preoperative radiographic measurements were performed by a single sports medicine orthopaedic surgery fellow (D.K.) to ensure consistency and limit interobserver variability. These measurements were subsequently reviewed and confirmed by the senior author to verify accuracy. Although the radiographs were obtained as part of routine clinical care, the measurements included in this study were performed specifically for the purposes of this investigation. Pre- and postoperative images are presented for comparison in Figure 7.

(A) Preoperative imaging of a patient with proximal tibiofibular joint instability including an anteroposterior (AP), lateral, and hip-to-ankle view to assess overall alignment. (B) Postoperative imaging in the AP and lateral views with the purple, red, and yellow asterisks denoting the femoral, tibial, and fibular anchors, respectively.
Outcome Measurements
PRO measures (PROMs), including the Lysholm score, International Knee Documentation Committee (IKDC) Subjective Knee Form, 12-item Short Form Health Survey Physical Component Summary, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and its subscales (pain, stiffness, function) were evaluated preoperatively and ≥2 years postoperatively. Additionally, sporting activity level (Tegner Activity Scale [TAS]) was evaluated at follow-up. Finally, revision surgery rates were evaluated.
Statistical Analysis
PRO scores were reported with medians and quartiles. The Wilcoxon signed-rank test was used to test for statistically significant improvements from baseline to ≥2 years postoperatively. P values <.05 were deemed statistically significant. No P value adjustments were made for multiple comparisons. All statistical analyses were performed using the statistical computing language R Version 4.4.0 (R Foundation for Statistical Computing).16,20
Results
Between August 2016 and November 2021, 29 patients underwent combined PTFJ and LCL reconstruction with the senior author. In total, 25 patients (86%) were followed up after a mean of 4.3 ± 2.1 years. Details on patient demographics are listed in Table 1. Preoperative radiological measurements are reported in Table 2. One patient who also underwent anterior cruciate ligament (ACL) reconstruction at the index procedure underwent arthroscopic debridement for a cyclops lesion 11 months postoperatively and was included for the outcome analysis. No patient underwent revision surgery for a complaint related to the combined PTFJ and LCL reconstruction. Twenty (80%) out of the 25 included patients underwent concomitant procedures (Table 3).
Patient Demographics (N = 25) a

Data are presented as mean ± SD or n (%).
Preoperative Radiological Measurements (N = 25) a
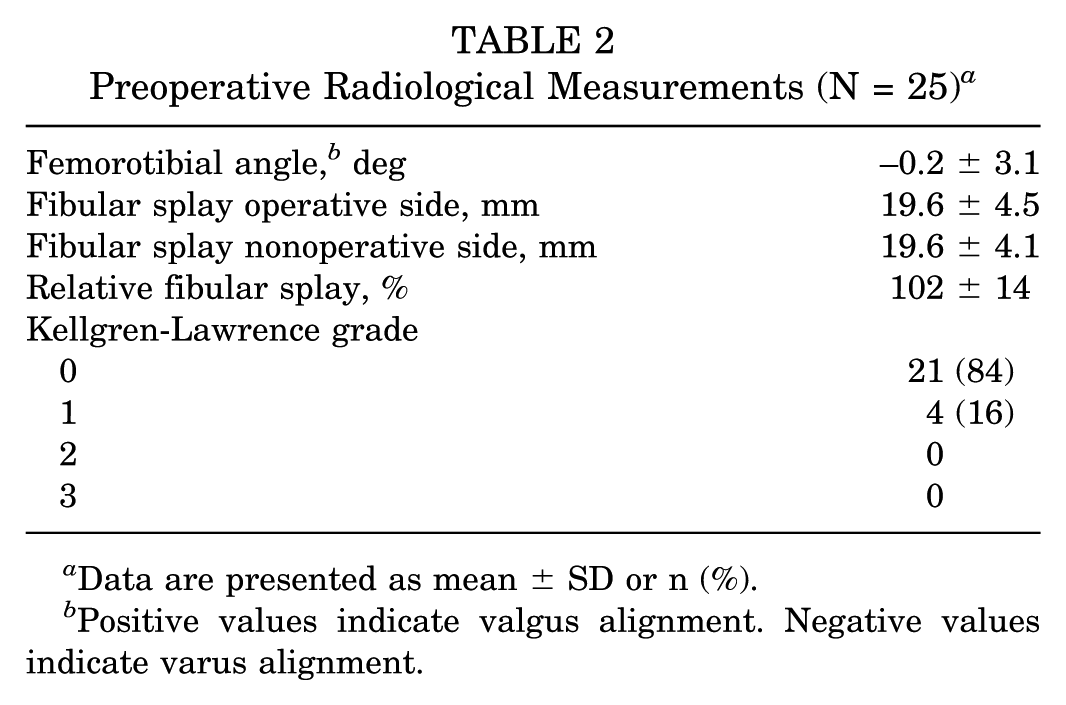
Data are presented as mean ± SD or n (%).
Positive values indicate valgus alignment. Negative values indicate varus alignment.
Concomitant Procedures (N = 25) a

Data are presented as n (%). ACL, anterior cruciate ligament; MCL, medial collateral ligament; MPFL, medial patellofemoral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner.
Outcome Assessment
All PROMs improved significantly from preoperatively to follow-up (P < .001) (Table 4). Sporting activity level (TAS) at follow-up was high (median, 6.0 [IQR, 3.0-7.0]). At a mean 4.3-year follow-up, 14 patients (56%) were not limited in sports following their injury at the recreational, collegiate, or national/Olympic levels. Furthermore, 5 patients (20%) were unable to participate in a few sports and 1 patient (4%) was unable to participate in any sport at follow-up.
Comparison Between Pre- and Postoperative PROMs a
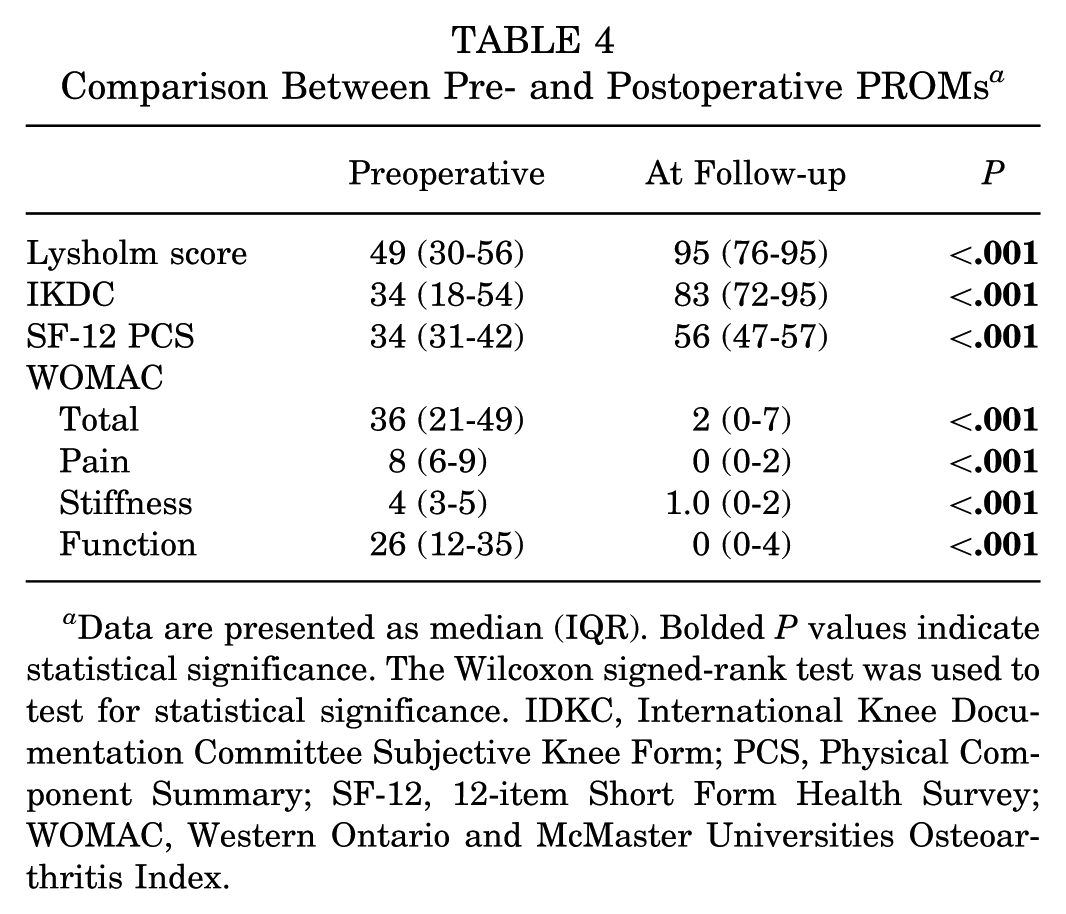
Data are presented as median (IQR). Bolded P values indicate statistical significance. The Wilcoxon signed-rank test was used to test for statistical significance. IDKC, International Knee Documentation Committee Subjective Knee Form; PCS, Physical Component Summary; SF-12, 12-item Short Form Health Survey; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Concomitant ACL reconstruction was not statistically significantly associated with postoperative PROMs (all P > .05), and the observed group differences were not clinically significant either. Similarly, patients who underwent a concomitant meniscal procedure did not exhibit statistically significantly different PROMs than those who did not undergo a meniscal procedure (all P > .05) (Appendix Tables A1 and A2).
Discussion
The most important finding of this study was that anatomic reconstruction of the PTFJ reconstruction with a single semitendinosus allograft resulted in favorable subjective and clinical outcomes at minimum 2-year follow-up, even when performed alongside additional procedures for concomitant knee injuries. The significant improvements observed in PROMs in this study, including the Lysholm score, IKDC score, and WOMAC, are consistent with the outcomes reported in similar studies that evaluated isolated PTFJ reconstruction. No patient required revision surgery due to issues related to the combined reconstruction of the PTFJ and LCL.
The findings of this study contribute to the limited body of literature on the surgical management of PTFJ instability, particularly in the context of concomitant knee injuries. As PTFJ instability is a rare condition with relatively few reported cases, the establishment of standardized treatment protocols remains challenging. Traditionally, nonoperative management has been the first-line approach for this condition, but surgical intervention is increasingly considered for patients with persistent or severe symptoms. 15
Recent studies have highlighted the efficacy of anatomic reconstruction techniques, as it allows for improved subjective and clinical outcomes as well as fewer complications compared with traditional methods such as arthrodesis and fibular head resection.2,3,5,8,10,11,14,18,22 In 2017, Kruckeberg et al 11 conducted a systematic review of various treatment approaches for PTFJ instability. A total of 44 relevant studies were identified, involving a total of 96 patients who were eligible for inclusion in the study. While the authors were unable to draw definitive conclusions due to the heterogeneity of techniques and small number of patients in each treatment group, they observed that biceps rerouting and anatomic reconstruction displayed the most favorable outcomes with low complication rates, whereas PTFJ fixation and fibular head resection were associated with higher complication rates (28% and 20%, respectively). They also found that nonoperative treatment was associated with persistent symptoms despite improvement.
Horst and LaPrade 7 assessed the outcomes of 2 patients who underwent free anatomic hamstring autograft PTFJ reconstruction. At a 2-year follow-up, both patients demonstrated significant improvement, reporting resolution of symptoms and the ability to return to their preinjury activity levels.
The largest case series to date performed by Dekker et al 2 reported on a cohort of 16 patients who underwent anatomic reconstruction and assessed their preoperative characteristics and postoperative outcomes. At ≥2-year follow-up, 84.6% of patients were able to return to full desired activities and previous level of sport. However, approximately half of the patients in the study required meniscal debridement or isolated chondroplasty for either a meniscal or chondral pathology, respectively. The authors attributed these concomitant pathologies to the fact that these patients showed only fair to moderate improvement at final follow-up in final debility, as assessed by their final Lysholm score and significant improvement from the minimal detectable change threshold of 8.9. 2 Our study finds that even despite concomitant injuries requiring additional intervention, which included meniscal debridement and chondroplasty, patients had significant improvement in PROMs at final follow-up.
Limitations
This study has several limitations inherent to its retrospective case series design. The lack of a control group limits the ability to directly compare the outcomes of combined PTFJ and LCL reconstruction with isolated procedures or alternative treatment methods. Additionally, while this study included a cohort with a relatively long follow-up period (mean, 4.3 years), the sample size remains small because of the rarity of PTFJ instability, potentially limiting the generalizability of the findings.
A significant limitation of this study is the absence of validated, objective radiographic criteria for diagnosing PTFJ instability. We measured fibular splay as the side-to-side difference in lateral diastasis on plain radiographs; however, this did not consistently differentiate the operative limb from the contralateral side. Prior studies have highlighted the challenges of using plain radiographs for this purpose, as subtle malalignment is often occult and highly dependent on positioning.1,4,6,13,17 A large cross-sectional analysis by Hey et al 6 described normal radiographic relationships in terms of tibiofibular overlap percentages and fibular orientation, reporting that >90% of normal knees demonstrate between 0% and 75% overlap of the fibular head with the tibia on AP views and that the fibula typically points toward the lateral femoral epicondyle or posterior half of the Blumensaat line. While these parameters appear highly specific, they are confounded by factors such as weightbearing status, degree of knee flexion, and radiographic technique.6,13 Moreover, reproducibility of fibular splay or tibiofibular overlap has not been formally studied, and no consensus thresholds exist for pathologic widening. This, combined with the fact that we did not perform a reliability assessment, makes it difficult to confirm true accuracy in our measurements. CT and MRI are more accurate in demonstrating displacement and ligamentous injury, respectively, and MRI in particular has been shown to detect soft tissue changes in both acute and chronic instability. 1 However, neither modality has established validated criteria or reliability metrics specifically for fibular splay. These findings highlight that while fibular splay is a conceptually useful radiographic parameter, its diagnostic objectivity is limited without standardized protocols. Future studies should incorporate standardized imaging protocols, reliability testing, and advanced modalities to establish objective diagnostic parameters for PTFJ instability.
Finally, concomitant knee injuries requiring additional procedures makes it difficult to isolate the specific impact of PTFJ and LCL reconstruction on patient outcomes. Although all patients showed significant improvements in PROMs, it is unclear to what extent these improvements were attributable to the PTFJ and LCL reconstruction versus the concomitant procedures. Despite these limitations, the consistency of our findings with the existing literature on isolated PTFJ reconstruction suggests that combined anatomic reconstruction techniques can be effective and produce favorable outcomes even in the setting of concomitant knee injuries.
Conclusion
The findings of this study highlight that patients who undergo anatomic reconstruction of the PTFJ reconstruction with a single semitendinosus allograft have favorable subjective and clinical outcomes at ≥2-year follow-up, even when performed alongside additional procedures for concomitant knee injuries. However, further investigation with a larger patient cohort is warranted to validate these outcomes and establish the clinical significance of anatomic reconstruction for PTFJ instability in the setting of concomitant injuries.
Footnotes
Appendix
Furthest Available Min 2-yr Post-operative PRO scores: By Concomitant Meniscus Procedure

| Characteristic | Overall (N = 25) | No Concom. (N = 14) | Yes Concom. (N = 11) | P |
|---|---|---|---|---|
| Lysholm | 0.738 | |||
| Median (Min-Max) | 91 (22-100) | 95 (22-100) | 91 (64-100) | |
| [Q1, Q3] | [73, 95] | [65, 95] | [73, 95] | |
| IKDC | 0.337 | |||
| Median (Min-Max) | 85 (25-99) | 90 (25-99) | 79 (39-97) | |
| [Q1, Q3] | [74, 95] | [66, 98] | [74, 92] | |
| Tegner Activity Scale | 0.956 | |||
| Median (Min-Max) | 6.00 (2.00-10.00) | 6.00 (2.00-10.00) | 6.00 (3.00-8.00) | |
| [Q1, Q3] | [4.00, 7.00] | [3.00, 8.00] | [4.00, 6.00] | |
| SF-12 PCS | 0.869 | |||
| Median (Min-Max) | 56 (23-60) | 55 (23-60) | 56 (32-59) | |
| [Q1, Q3] | [44, 57] | [38, 58] | [44, 57] | |
| SF-12 MCS | 0.411 | |||
| Median (Min-Max) | 56 (36-64) | 53 (36-64) | 57 (38-59) | |
| [Q1, Q3] | [50, 58] | [48, 60] | [55, 58] | |
| WOMAC Pain | 0.600 | |||
| Median (Min-Max) | 1.0 (0.0-13.0) | 0.0 (0.0-11.0) | 2.0 (0.0-13.0) | |
| [Q1, Q3] | [0.0, 2.0] | [0.0, 4.0] | [0.0, 2.0] | |
| WOMAC Stiffness | 0.954 | |||
| Median (Min-Max) | 1.00 (0.00-6.00) | 1.00 (0.00-5.00) | 1.00 (0.00-6.00) | |
| [Q1, Q3] | [0.00, 3.00] | [0.00, 3.00] | [0.00, 3.00] | |
| WOMAC Function | 0.931 | |||
| Median (Min-Max) | 1 (0-36) | 1 (0-30) | 1 (0-36) | |
| [Q1, Q3] | [0, 4] | [0, 10] | [0, 4] | |
| WOMAC Total | 0.715 | |||
| Median (Min-Max) | 2 (0-55) | 2 (0-46) | 2 (0-55) | |
| [Q1, Q3] | [0, 8] | [0, 19] | [0, 8] |
Final revision submitted November 3, 2025; accepted December 7, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.P. has received royalties from Arthrex, Arthrosurface, Responsive Arthroscopy, and Anika Therapeutics; consulting fees from Arthrex, the Joint Restoration Foundation, Zimmer Biomet, Arthrosurface, and JRF Ortho; grants from the US Department of Defense, the National Institutes of Health, and DJO; and honoraria from Flexion Therapeutics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Vail Health Hospital institutional review board (protocol No. 2023-180-SPRI).