
Abstract
Background:
Lateral ankle sprains are the most common lower extremity injury in athletes, most often involving the anterior talofibular ligament (ATFL). Although ATFL repair outcomes are well studied, optimal management for patients with generalized ligamentous laxity (GLL) remains less understood.
Purpose:
To (1) evaluate the radiographic findings, clinical measures, and complications in patients with GLL undergoing modified Broström-Gould repair and to (2) assess the role of suture augmentation in optimizing outcomes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
During July 2025, the PubMed, EMBASE, and Cochrane library databases were systematically searched to identify studies examining outcomes and complications in GLL patients who underwent modified Broström-Gould repair.
Results:
Eight studies including 301 GLL patients (309 ankles) and 367 patients (370 ankles) without ligamentous laxity were analyzed. Both cohorts demonstrated postoperative clinical improvement. A significant difference in postoperative talar tilt angle existed only between GLL patients who underwent modified Broström-Gould repair without suture augmentation and patients without ligamentous laxity (mean difference, 2.18°; 95% CI, 0.57°-3.79°; P = .008). GLL patients experienced 53 (17.2%) failures and were 4.79 times more likely to develop recurrent mechanical instability than patients without ligamentous laxity (risk ratio [RR], 4.79; 95% CI, 1.70-13.5; P = .003). Among GLL patients, the absence of suture augmentation was associated with a 2.95-fold higher complication risk compared with patients without ligamentous laxity (RR, 2.95; 95% CI, 1.08-8.01; P = .03). When suture augmentation was performed, no significant difference in complication rates existed between cohorts.
Conclusion:
Patients with GLL experienced significantly higher rates of complication and failure following modified Broström-Gould repair compared with patients without ligamentous laxity. Suture augmentation may lower complication rates in GLL patients, but its effect on failure rates remains undetermined, as no studies directly compared augmented and nonaugmented GLL patients. Importantly, both GLL patients and patients without ligamentous laxity experienced clinical improvements from the modified Broström-Gould repair. While GLL increases the risk of mechanical complications, it should not be considered a contraindication to undergoing the modified Broström-Gould procedure. However, suture augmentation may be beneficial for GLL patients to reduce the risk of complications after undergoing ATFL repair.
Registration:
CRD420251182303 (PROSPERO identifier).
Acute ankle sprains are the most common lower extremity injury in athletes, accounting for up to 40% of all sports-related injuries. 7 The anterior talofibular ligament (ATFL) is the most frequently injured lateral ligament due to its inherently lower tensile strength and reduced load-bearing capacity compared with the other lateral ligaments. 5 While 80% of acute ankle sprains resolve with conservative management, 20% of patients will require surgical intervention. 1 One operative option for patients includes the modified Broström-Gould repair, in which the damaged ATFL is anatomically shortened and reattached to the fibula, with reinforcement from the inferior extensor retinaculum (IER). 13 Although numerous studies have evaluated outcomes following ATFL repair, there is a lack of evidence analyzing patients with underlying ligamentous conditions.
Generalized ligamentous laxity (GLL) is characterized by hypermobility and abnormally increased range of motion (ROM) in patients, present in approximately 5% to 15% of individuals in the general population.9,18 In athletes with GLL, increased dynamic pressures contribute to medial forefoot collapse, ultimately worsening ankle instability and predisposing players to ankle sprains. 6 Furthermore, soft tissue procedures remain challenging in this patient population, due to impaired wound healing and poorer tissue quality. 21 While patients with ligament conditions have a higher propensity for ankle injuries, there is a paucity of research investigating outcomes following ATFL repair in patients with GLL.
To date, there has been no systematic review and meta-analysis that comprehensively evaluates how ligamentous laxity affects clinical outcome scores, complications, and failure rates in patients undergoing ATFL repair. Therefore, the purpose of this systematic review and meta-analysis is to evaluate the radiographic findings, clinical measures, and complications in patients with GLL undergoing modified Broström-Gould repair and to assess the role of suture augmentation in optimizing outcomes for this patient population.
Methods
Search Strategy
In July 2025, a systematic review of the PubMed, EMBASE, and Cochrane Library databases was performed based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The following search terms were used: ((ATFL OR anterior talofibular ligament) AND (ligamentous laxity OR laxity OR hypermobility)). Studies met inclusion criteria if they reported on outcomes after ATFL repair in patients with ligamentous laxity defined as Beighton scores ≥4, were published in peer-reviewed journals, and were written in English. Studies were excluded if patients received an ATFL procedure that was not a modified Broström-Gould, were review articles, cadaveric studies, or case reports. Once the data were retrieved, the titles, abstracts, and full-text articles were screened by 2 independent reviewers (J.R., A.T.). If there were disagreements between reviewers, a senior author evaluated whether the paper should be included or excluded.
Assessment of Level of Evidence and Methodological Quality
The level of evidence (LOE) was assessed using previously accepted criteria. 11 The methodological quality of clinical evidence and risk of bias was assessed using the methodological index for non-randomized studies (MINORS) criteria by 2 independent reviewers (J.R., A.T.) (Table 1). 19 Studies that were comparative were evaluated with the additional criteria for comparative studies. The ideal MINORS score for noncomparative studies and comparative studies is 16 and 18, respectively. Of note, 2 of the included comparative studies reached ideal MINORS scores,17,27 while the other 2 studies represented a risk of bias.14,26 The certainty of evidence for each key outcome was assessed using the Grading of Recommendation, Assessment, Development and Evaluation (GRADE) criteria (Table 2). Overall, the certainty of evidence across outcomes ranged from low to very low. The quality of evidence was downgraded primarily for the high risk of selection bias due to nonrandomized cohort designs and imprecision resulting from small sample sizes and wide confidence intervals. Given the heterogeneity in the reporting of patient-reported outcomes across studies, some outcomes were also downgraded for inconsistency. If any discrepancy arose for either MINORS or GRADE criteria assessment, a senior author (J.G.K.) was consulted to evaluate the data for a final consensus.
Summary of Study Quality and Risk of Bias Assessment Based on MINORS Criteria for Noncomparative and Comparative Studies a

MINORS, methodological index for non-randomized studies; N/A, not applicable.
A - A clearly stated aim; B - Inclusion of consecutive patients; C - Prospective collection of data; D - Endpoints appropriate to the aim of the study; E - Unbiased assessment of the study endpoint; F - Follow-up period appropriate to the aim of the study; G - Loss to follow up less than 5%; H - Prospective calculation of the study size; I - An adequate control group; J - Contemporary groups; K - Baseline equivalence of groups; L - Adequate statistical analyses; M - Total.
Summary of GRADE Certainty of Evidence a
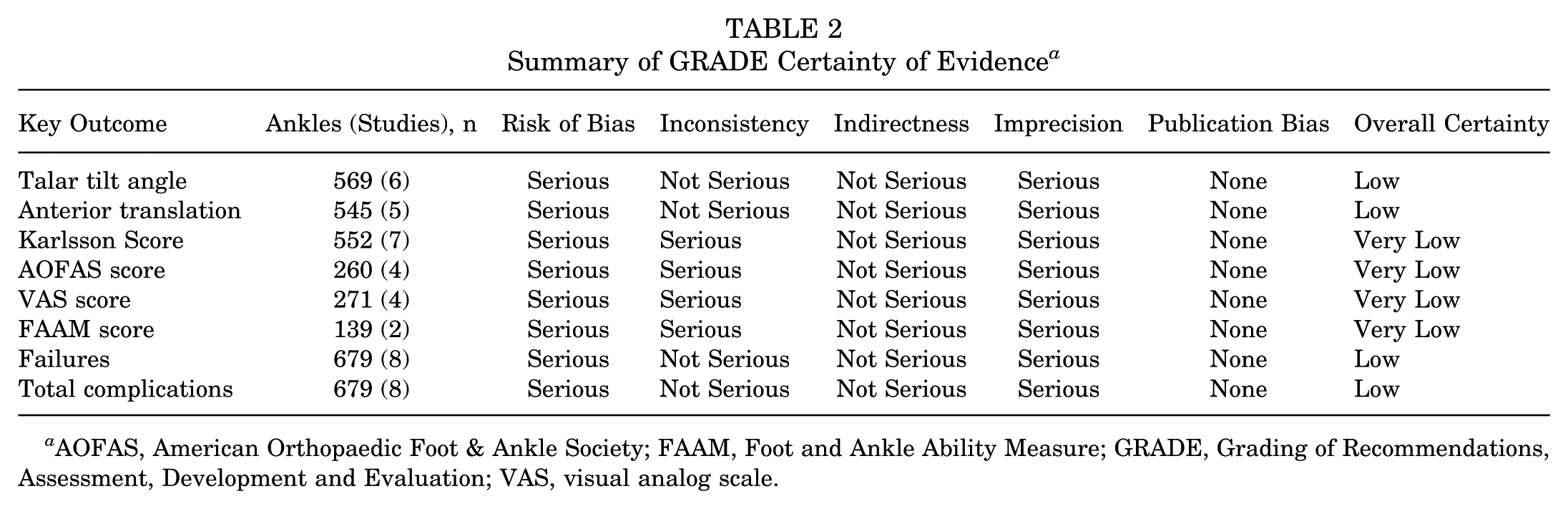
AOFAS, American Orthopaedic Foot & Ankle Society; FAAM, Foot and Ankle Ability Measure; GRADE, Grading of Recommendations, Assessment, Development and Evaluation; VAS, visual analog scale.
Data Extraction and Evaluation
Two reviewers (J.R., A.T.) independently extracted and assessed data from each study. Data on patient demographics, including number of patients, number of ankles, follow-up time, age, sex, laterality of injury, body mass index (BMI), Beighton score, and surgical technique utilized for ATFL repair were reported. Surgical characteristics, radiographic findings, clinical outcomes, complications, and failures were also evaluated.
Statistical Analysis
Statistical analysis was performed using RStudio (Version 2025.05.01). Descriptive statistics were calculated for all continuous and categorical variables. Continuous variables were reported as weighted mean and estimated standard deviation, whereas categorical variables were reported as frequencies with percentages. The outcome measures of interest were talar tilt angle, anterior translation, Karlsson score, failures, and total complications. Heterogeneity among studies was quantified using the I2 statistic, and random-effects DerSimonian-Laird model was used throughout given the expected clinical heterogeneity. For continuous outcomes, mean differences (MDs) and risk ratios (RRs) were calculated with a 95% CI. A value of P < .05 was considered statistically significant. Assessment of publication bias using a funnel plot or Egger regression was not feasible, as <10 studies were included in the meta-analyses and would not achieve sufficient statistical power to distinguish random chance from true asymmetry. 20
Results
Study Characteristics and Patient Demographics
The search generated 198 studies, published between 1983 and 2025. Of these, 8 met the inclusion and exclusion criteria (Figure 1). Study characteristics and patient demographics are listed in Table 3. Six of the included studies were LOE 314,17,24-27 and 2 were LOE 4.2,8 Of the 8 studies, 4 directly compared patients with ligamentous laxity to patients without ligamentous laxity.14,17,26,27

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
Study Characteristics and Patient Demographics a

Data are presented as n unless otherwise indicated. Dashes indicate data not reported. arth, arthroscopic; BMI, body mass index; F, female; GLL, generalized ligamentous laxity; LOE, level of evidence; M, male.
In total, there were 301 patients (309 ankles) with GLL and 367 patients (370 ankles) without ligamentous laxity.2,8,14,17,24-27 GLL was defined as a Beighton score ≥4 in 6 studies,2,8,14,24,25,27 Beighton score ≥5 in 1 study, 26 a Beighton score of ≥4, 5, or 6 dependent on patient age in 1 study. 17 The weighted mean age was 30.1 ± 4.7 years (range, 21.7-37.8 years) for patients with GLL and 32.7 ± 3.2 years (range, 29.0-35.9 years) for patients without ligamentous laxity.2,8,14,17,24-27 There were 149 (49.5%) men and 152 (50.5%) women with GLL, and 226 (61.6%) men and 141 (38.4%) women without ligamentous laxity.2,8,14,17,24-27 The weighted mean BMI was 23.6 ± 0.6 kg/m2 (range, 22.8-24.2 kg/m2) for patients with GLL and 23.9 ± 1.1 kg/m2 (range, 22.5-24.5 kg/m2) for patients without ligamentous laxity.14,17,24-26 The weighted mean follow-up time was 34.6 ± 15.2 months (range, 12.0-62.3 months) for patients with GLL and 38.6 ± 21.5 months (range, 12.0-59.5 months) for patients without ligamentous laxity.2,8,14,17,24-27 Of the 4 studies that reported on laterality of 183 ankles for patients with GLL, 92 (50.3%) right ankles and 91 (49.7%) left ankles were operated on.17,24-26 Of the 2 studies that reported on laterality of 138 ankles for patients without ligamentous laxity, 72 (52.2%) right ankles and 66 (47.8%) left ankles were operated on.17,26 The weighted mean Beighton score for patients with GLL was 5.8 ± 0.6.2,8,17,24,25 One study reported a Beighton score of 2.0 ± 1.3 for patients without ligamentous laxity. 17
Surgical Characteristics
The associated surgical characteristics included in this systematic review and meta-analysis are summarized in Table 4. Indications for surgery included chronic lateral ankle instability (CLAI) present in patients for ≥6 months.2,8,14,17,24-27 CLAI was defined as recurrent “giving-way” sensation, persistent pain, inability to resume preinjury activity level, or laxity despite treatment with nonoperative management. Of note, 4 studies required patients to have experienced CLAI for ≥6 months and to have a minimum failed 3 months of nonoperative management prior to undergoing surgery.2,8,17,24 All patients underwent the modified Broström-Gould technique in which the ATFL was repaired via suture anchors or bone tunnels, followed by reinforcement with the IER to enhance lateral ankle stability.2,8,14,17,24-27 Of note, 2 studies included 139 patients who underwent the modified Broström-Gould technique with suture augmentation.2,17 The associated conditions identified intraoperatively included soft tissue impingement, osteophytes, osteochondral lesions of the talus, os trigonum, synovitis, ossicles, syndesmosis widening, loose bodies, avulsion fractures, and sinus tarsi syndrome.8,14,17,24-27
Summary of Surgical Characteristics a

Dash indicates data not reported. arth, arthroscopic; ATFL, anterior talofibular ligament; CLAI, chronic lateral ankle instability; OLT, osteochondral lesion of the talus.
Radiographic Findings
The radiographic findings included in this systematic review and meta-analysis are summarized in Table 5. For patients with GLL, the weighted mean talar tilt angle was 13.5°± 1.5° (range, 12.2° to 16.2°) preoperatively and 5.3°± 1.9° (range, 2.1° to 7.9°) at final follow-up.2,8,14,17,26,27 For patients without ligamentous laxity, the weighted mean talar tilt angle was 11.3°± 2.2° (range, 8.0° to 12.7°) preoperatively and 4.4°± 0.6° (range, 3.9° to 5.2°) at final follow-up.14,17,26,27 There was no statistically significant difference in postoperative talar tilt angle between all GLL patients and patients without ligamentous laxity (MD, 1.55°; 95% CI, –0.23° to 3.33°; P = .09) (Figure 2). However, when excluding patients who received suture augmentation, there was a significantly greater postoperative talar tilt angle among GLL patients compared with patients without ligamentous laxity (MD, 2.18°; 95% CI, 0.57° to 3.79°; P = .008) (Figure 2).
Summary of Radiographic Findings a

Data are presented as n or mean ± SD. Dashes indicate data not reported. arth, arthroscopic; Preop, preoperative.

Meta-analysis of postoperative talar tilt angle between generalized ligamentous laxity (GLL) patients and patients without ligamentous laxity. IV, inverse variance; non-lax, non-laxity.
For patients with GLL, the weighted mean anterior translation was 9.5 ± 1.7 mm (range, 8.1 to 12.1 mm) preoperatively and 5.5 ± 1.0 mm (range, 4.1 to 6.5 mm) at final follow-up.2,8,14,17,25,26 For patients without ligamentous laxity, the weighted mean anterior translation was 8.7 ± 1.0 mm (range 8.1 to 10.0 mm) preoperatively and 5.2 ± 0.7 mm (range, 4.4 to 5.7 mm) at final follow-up (Table 5).14,17,26 There was no statistically significant difference in postoperative anterior translation between all GLL patients and patients without ligamentous laxity (MD, 0.48, 95% CI, –0.42 to 1.38; P = .30) (Figure 3).

Meta-analysis of postoperative anterior translation between generalized ligamentous laxity (GLL) patients and patients without ligamentous laxity. IV, inverse variance; non-lax, non-laxity.
Clinical Outcomes
The clinical outcomes included in this systematic review and meta-analysis are summarized in Table 6. Four different subjective scoring tools were utilized among the included studies, including the Karlsson score, the American Orthopaedic Foot & Ankle Society (AOFAS) score, the visual analog scale (VAS), and the Foot and Ankle Ability Measure (FAAM). The most commonly utilized patient-reported outcome measure was Karlsson, recorded in 6 of the included studies.8,14,17,24-26 For patients with GLL, the weighted mean Karlsson score was 57.1 ± 7.2 (range, 43.7 to 63.6) preoperatively and 86.3 ± 3.8 (range, 82.0-90.6) at final follow-up, for an overall increase of 29.2 ± 8.1 (P = .003).8,14,17,24-26 For patients without ligamentous laxity, the weighted mean Karlsson score was 53.0 ± 3.6 (range, 48.3 to 55.1) preoperatively and 88.4 ± 5.4 (range, 83.4 to 94.1) at final follow-up, for an overall increase of 35.4 ± 6.5 (P = .04).14,17,26 There was no statistically significant difference in postoperative Karlsson score between all GLL patients and patients without ligamentous laxity (MD, –4.00; 95% CI, –9.18 to 1.18; P = .13) (Figure 4). A secondary meta-analysis pooling all available patient-reported outcome measures demonstrated a standardized mean difference (SMD) favoring patients without ligamentous laxity (SMD, −0.47; 95% CI, −1.03 to 0.08; P = .09) (Appendix Figure S1).
Summary of Clinical Outcomes a
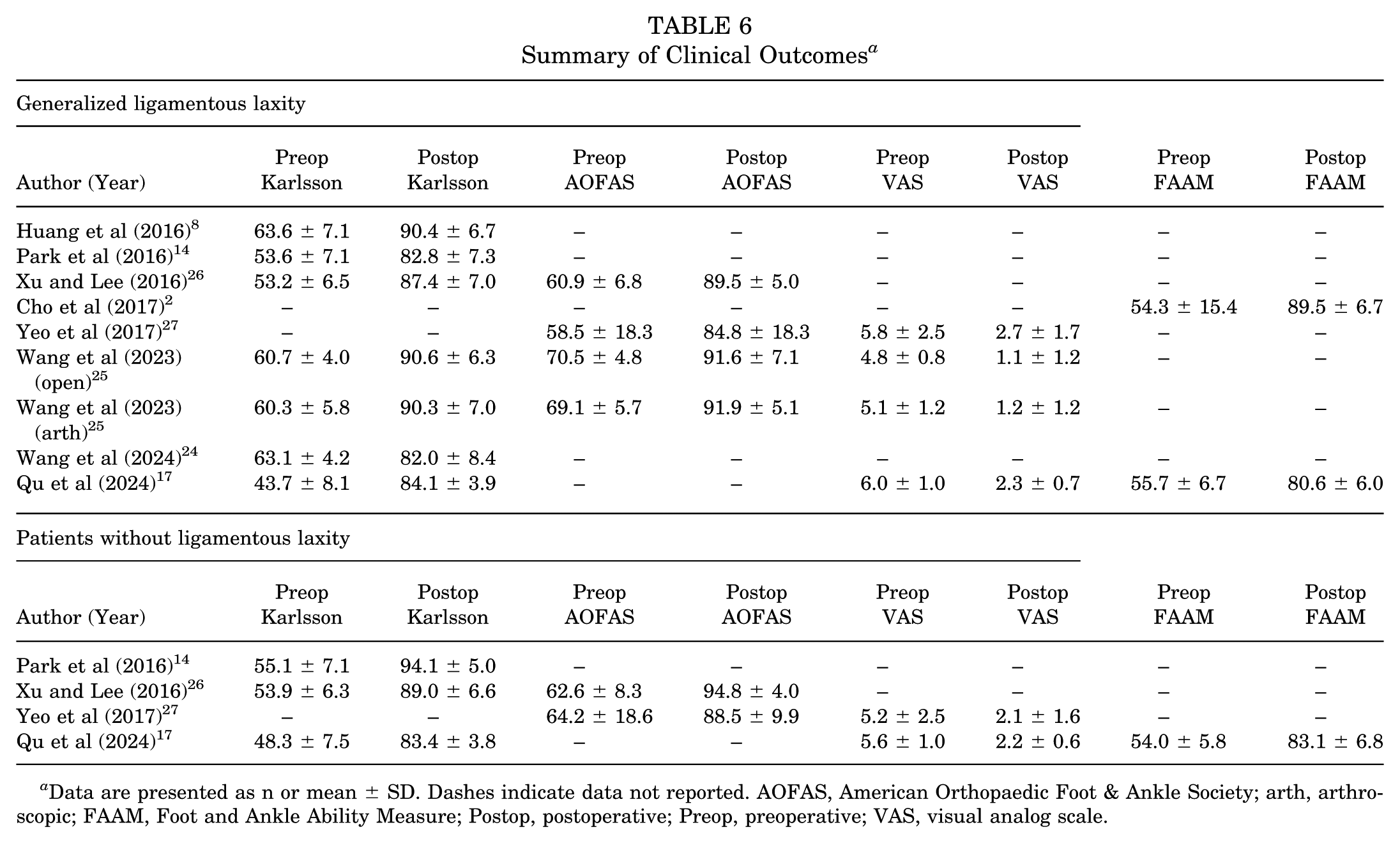
Data are presented as n or mean ± SD. Dashes indicate data not reported. AOFAS, American Orthopaedic Foot & Ankle Society; arth, arthroscopic; FAAM, Foot and Ankle Ability Measure; Postop, postoperative; Preop, preoperative; VAS, visual analog scale.

Meta-analysis of postoperative Karlsson score between generalized ligamentous laxity (GLL) patients and patients without ligamentous laxity. IV, inverse variance; non-lax, non-laxity.
For patients with GLL, the weighted mean AOFAS score was 64.7 ± 5.9 (range, 58.5-70.5) preoperatively and 89.5 ± 3.3 (range, 84.8-91.9) at final follow-up, for an overall increase of 24.8 ± 6.8 (P = .04).25-27 For patients without ligamentous laxity, the weighted mean AOFAS score was 63.5 ± 1.1 (range, 62.6-64.2) preoperatively and 91.2 ± 4.5 (range, 88.5-94.8) at final follow-up, for an overall increase of 27.7 ± 4.1 (P = .08).26,27 For patients with GLL, the weighted mean VAS was 5.4 ± 0.6 (range, 4.8-6.0) preoperatively and 1.8 ± 0.8 (range, 1.1-2.7) at final follow-up, for an overall decrease of 3.6 ± 1.0 (P < .001).17,25,27 For patients without ligamentous laxity, the weighted mean VAS was 5.4 ± 0.3 (range, 5.2-5.6) preoperatively and 2.2 ± 0.1 (range, 2.1-2.2) at final follow-up, for an overall decrease of 3.2 ± 0.3 (P = .03).17,27 For patients with GLL, the weighted mean FAAM was 55.0 ± 1.0 preoperatively (range, 54.3-55.7) and 85.0 ± 6.3 (range, 80.6-89.5) at final follow-up, for an overall increase of 30.0 ± 6.4 (P = .11).2,17 One study reported FAAM for patients without ligamentous laxity, demonstrating an increase from 54.0 ± 5.8 preoperatively to 83.1 ± 6.8 at final follow-up (P < .01) (Table 6). 17 Of note, Xu and Lee 26 reported a significant difference in Tegner score improvement between cohorts, with scores increasing from 3.3 to 6.4 in GLL patients and from 3.8 to 7.9 in those without ligamentous laxity (P = .01). 26
Complications and Failures
The complications and failures reported in this systematic review and meta-analysis are described in Table 7. Failures were defined as cases of recurrent mechanical instability or patients who required revision surgeries. There was a total of 66 (21.4%) complications in the ankles of patients with GLL who underwent ATFL repair.2,8,14,17,24-27 The most common complication was 53 (17.2%) failures after the operation, of which all GLL failures experienced recurrent mechanical instability consisting of “give-way” or subsequent ankle sprains.2,8,14,24-26 Of note, 10 (3.2%) of these patients underwent percutaneous allograft reconstruction as a revision surgery because of recurrent mechanical instability. Other complications for GLL patients included 6 (1.9%) cases of restricted ROM, 4 (1.3%) infections, 2 (0.6%) nerve injuries, and 1 (0.3%) case of persistent pain.2,8,14,17,24-27
Summary of Complications and Failures a

Data are presented as n. Dashes indicate data not reported. arth, arthroscopic; ROM, range of motion.
There were 20 (5.4%) complications in the ankles of patients without ligamentous laxity who underwent ATFL repair.14,17,26,27 The most common complication was 9 (2.4%) failures after the operation.14,17,26 One (0.3%) patient without ligamentous laxity experienced recurrent instability. Six (1.6%) patients without ligamentous laxity underwent percutaneous allograft reconstruction as a revision surgery because of recurrent mechanical instability. Other complications in the ankles of patients without ligamentous laxity included 5 (1.4%) infections, 4 (1.1%) nerve injuries, 2 (0.5%) cases of restricted ROM, and 2 (0.5%) cases of persistent pain.14,17,26,27
GLL patients who underwent modified Broström-Gould without suture augmentation demonstrated significantly higher rates of failure compared with patients without ligamentous laxity (RR, 6.25; 95% CI, 2.62-14.9; P < .0001) (Figure 5). Additionally, there was a statistically significant increase in failures when GLL patients were combined irrespective of surgical technique (RR, 4.79; 95% CI, 1.70-13.5; P = .003) (Figure 5). A statistical comparison between GLL patients undergoing modified Broström-Gould with versus without suture augmentation could not be performed because of a paucity of data, as no included studies directly compared these 2 GLL subgroups directly. GLL patients who underwent modified Broström-Gould without suture augmentation demonstrated a significantly higher rate of total complications compared with patients without ligamentous laxity (RR, 2.95; 95% CI, 1.08-8.01; P = .03) (Figure 6). However, when all GLL patients were combined irrespective of surgical technique, the difference in total complications between cohorts did not reach statistical significance (RR, 2.31; 95% CI, 0.93-5.75; P = .07) (Figure 6).
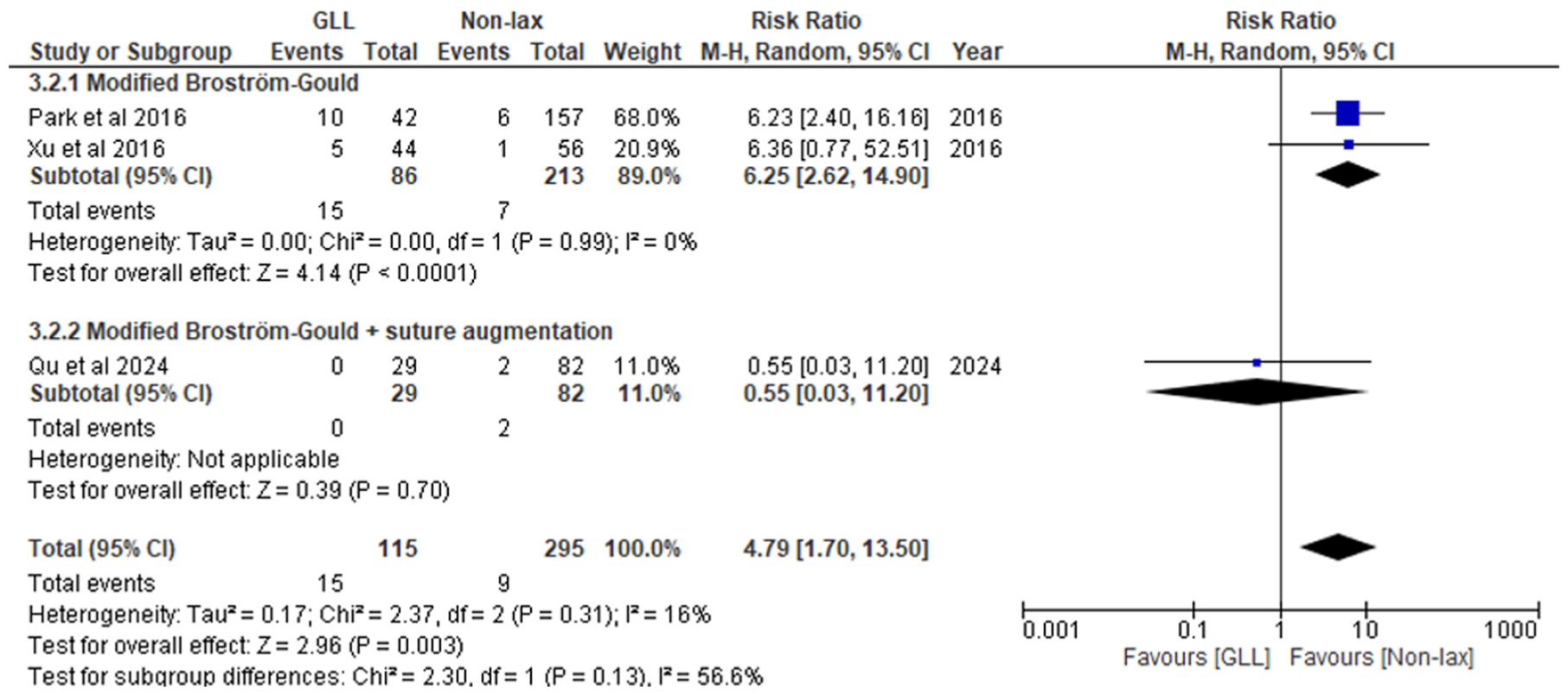
Meta-analysis of failure rates between generalized ligamentous laxity (GLL) patients and patients without ligamentous laxity. M-H, Mantel-Haenszel; non-lax, non-laxity.

Meta-analysis of total complications between generalized ligamentous laxity (GLL) patients and patients without ligamentous laxity. M-H, Mantel-Haenszel; non-lax, non-laxity.
Discussion
The most important finding of this systematic review and meta-analysis is that GLL patients who underwent modified Broström-Gould without suture augmentation demonstrated significantly higher postoperative talar tilt angle and total complications compared with patients without ligamentous laxity. Furthermore, for all GLL patients, there was a significantly higher failure rate following Broström-Gould compared with patients without ligamentous laxity. Both cohorts of patients showed improvements in radiographic parameters and clinical outcomes following ATFL repair.
Complications are an inherent possibility when undergoing surgery, as no operative intervention is entirely without risk. For GLL patients who underwent ligament augmentation reconstruction system (LARS), Porter et al 16 found an overall complication rate of 8%. In the current study, GLL patients who underwent modified Broström-Gould had a higher overall complication rate of 21.4%, compared with 5.4% for patients without ligamentous laxity. In comparison with reconstruction techniques such as LARS, repair techniques such as the modified Broström-Gould heavily rely on the patient's native ligaments for surgical success. In GLL patients, the reduced tissue quality and weaker ligaments may be more susceptible to surgical stress or delayed healing, contributing to higher complication rates found in this patient population. 4 In addition to increased risk of complications following surgery, ligamentous laxity also predisposes patients to higher failure rates. Failure rates can be as high as 43% for a range of orthopaedic procedures. 23 GLL increases failure rates in orthopaedic surgeries due to inherently hyperlax ligaments that are more susceptible to elongation, compromising graft or repair stability compared with patients without ligamentous laxity. Previous research has shown that patients with GLL who underwent ACL reconstruction had autograft failure rates as high as 30%. 10 In the current systematic review and meta-analysis, the failure rate was significantly higher in GLL patients undergoing modified Broström-Gould (17.2%) compared with patients without ligamentous laxity (2.4%). Overall, GLL patients experienced a significantly higher risk of both complications and failures after undergoing modified Broström-Gould repair compared with patients without ligamentous laxity.
In regard to ATFL repair for patients without ligamentous laxity, previous literature has demonstrated that suture augmentation may not influence the biological healing of the ligament itself and may not improve clinical outcomes for patients.3,12 Suture augmentation may restrict the natural mobility of the ankle joint, altering normal biomechanics and potentially limiting clinical improvement in patients who undergo the procedure. However, in patients with ligamentous laxity, additional support provided by suture augmentation may help offset their inherent weakness and poor tissue quality. 15 For this patient population, suture augmentation enhanced mechanical stability and reduced the risk of recurrent injuries. In the current systematic review and meta-analysis, patients who received modified Broström-Gould without suture augmentation had statistically significantly more complications than patients without ligamentous laxity. Interestingly, a statistically significant difference was not found when including GLL patients who also received suture augmentation. GLL patients who underwent modified Broström-Gould repair without suture augmentation also demonstrated significantly greater postoperative talar tilt angles compared with patients without ligamentous laxity. The hyperlax ligaments in GLL patients provided less restraint to the talus, ultimately resulting in radiographic instability. Incorporating suture augmentation reinforces the repair and may lead to better outcomes, demonstrated by the absence of significant difference in postoperative talar tilt angles when patients with augmented repairs were included in the statistical analysis. These findings suggest that suture augmentation may be pertinent to limit complications and radiographic instability in GLL patients who undergo modified Broström-Gould for ATFL repairs. Unlike complications and postoperative talar tilt, where inclusion of augmented GLL patients in pooled analyses altered statistical significance, the failure data were limited and lacked direct comparative cohorts. While suture augmentation may be beneficial in regard to complication rates or radiographic stability, its role in failures among GLL patients remains undetermined. When counseling GLL patients preoperatively, it is important to explain the potential benefits of suture augmentation, as well as the uncertainty regarding its ability to provide sufficient structural support and prevent repair failure in this patient population.
A previous systematic review by Tang et al 22 evaluated outcomes of modified Broström repairs in patients with GLL, finding a significantly higher recurrence of instability in this cohort. While their 2021 study provided valuable preliminary insights, the current systematic review and meta-analysis addressed key limitations and offered more comprehensive evidence for GLL patients undergoing ATFL repair. First, we included additional studies published since 2021, increasing the overall sample size and thus improving statistical power to detect meaningful differences between patients with and without GLL. Second, while Tang et al only conducted pooled analyses for postoperative angles and recurrent instability, our study also evaluated patient-reported outcomes, such as the Karlsson score, to better establish functional results between both cohorts. Importantly, a pooled analysis of total complications was not examined in the prior review, an outcome highly relevant to surgical decision-making. Third, although Tang et al acknowledged the potential importance of suture augmentation, they did not evaluate its impact statistically. In contrast, the current systematic review and meta-analysis differentiated outcomes between patients who underwent modified Broström-Gould repair with and without suture augmentation, providing a clinically important context. Finally, while Tang et al suggested that GLL may not be a contraindication to ATFL repair, our study provided definitive quantitative risk estimates, demonstrating a 4.79 times higher failure rate and 2.95 times higher complication rate in GLL patients. Furthermore, this study demonstrated the difference in statistical significance when incorporating patients who received suture augmentation. Therefore, these methodological improvements allow the present systematic review and meta-analysis to provide an up-to-date and clinically meaningful understanding of outcomes following modified Broström-Gould repair in patients with GLL.
Limitations
This systematic review and meta-analysis has several limitations. First, the availability of high-quality prospective studies was limited, as all the included studies were LOE 3 to 4 and retrospective in nature, introducing the possibility of selection and reporting bias. Second, there was heterogeneity in data reporting, such as variation in follow-up duration and patient age. Although most studies defined GLL using a minimum Beighton score ≥4, 2 studies provided alternative criteria that contribute to the heterogeneity in the classification of GLL across studies. These factors may have influenced the clinical outcomes by affecting the likelihood of detecting longer-term complications and other adverse outcomes for this study population. Third, while an exploratory pooled analysis of multiple patient-reported outcome measures was performed using standardized mean differences, the inclusion of overlapping cohorts may have introduced bias and should be interpreted with caution. Furthermore, formal subgroup analyses or metaregression comparing augmented versus nonaugmented repairs, as well as analyses by Beighton threshold, age, or BMI, were not performed because of the small number of available studies and minimal variability in these parameters, limiting the feasibility of meaningful stratified analysis. Finally, studies published in databases that were not searched in this systematic review and meta-analysis were not evaluated.
Conclusion
Patients with GLL experience significantly higher rates of complication and failure following modified Broström-Gould repair compared with patients without ligamentous laxity. Suture augmentation may lower complication rates in GLL patients, but its effect on failure rates remains undetermined, as no studies directly compared augmented and nonaugmented GLL patients. Importantly, both GLL patients and patients without ligamentous laxity experienced clinical improvements from the modified Broström-Gould repair. While GLL increases the risk of mechanical complications, it should not be considered a contraindication to undergoing the modified Broström-Gould procedure. However, suture augmentation may be beneficial for GLL patients to reduce the risk of complications after undergoing ATFL repair.
Footnotes
Appendix
Final revision submitted November 20, 2025; accepted December 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.G.K. is a consultant for Arthrex and receives financial support from Mr. Winston Fisher, Ms. Tatiana Rybak, and the Ohnell Family Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.