
Abstract
Background:
Arthroscopic anterior cruciate ligament (ACL) primary repair (ACLPR) has reemerged as a treatment option for select proximal ACL tears. However, concerns persist regarding its ability to restore knee stability adequately to support meniscal healing after concurrent meniscal repair.
Purpose:
To evaluate the clinical outcomes after medial and/or lateral meniscus repair in patients undergoing ACLPR, compared with isolated ACLPR (ACLPR-only) and ACLPR with partial meniscectomy (ACLPR-PME).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Consecutive patients with complete, proximal modified Sherman type 1 and 2 ACL tears who underwent ACLPR between 2008 and 2021 with a minimum 2-year follow-up were included. Patients were categorized into 3 groups: ACLPR-only, ACLPR with meniscal repair (ACLPR-MR), and ACLPR-PME. The primary outcome was the International Knee Documentation Committee (IKDC) Subjective Knee Form score. Secondary outcomes consisted of meniscal repair and ACLPR failure, overall reoperation rates, anterior tibial translation side-to-side difference (ATT SSD), clinical outcomes (Lachman test and pivot-shift test results), and patient-reported outcome measures (PROMs) including the Lysholm score, Forgotten Joint Score–12, Anterior Cruciate Ligament Return to Sport after Injury score, and Tegner activity scale score.
Results:
A total of 276 patients (ACLPR-only: n = 131; ACLPR-MR: n = 76; ACLPR-PME: n = 69) with a mean age of 39.7 ± 10.7 years (50.4% female) and mean follow-up of 2.9 ± 1.0 years were included (7.4% lost to follow-up). The mean IKDC scores demonstrated no significant difference between groups (ACLPR-only: 89.4 ± 10.3 [95% CI, 87.2-91.6]; ACLPR-MR: 86.7 ± 12.9 [95% CI, 83.6-89.8]; ACLPR-PME: 89.2 ± 9.9 [95% CI, 86.6-91.9]; P = .27). Eight patients (10.5%) in the ACLPR-MR group experienced recurrent meniscal injury. ACLPR failure occurred in 28 patients (10.1%), with no significant difference between groups (P = .62). Younger age was a significant predictor of ACLPR failure (P < .01), but not meniscal repair failure (P = .77). No group differences were observed in ATT SSD (ACLPR-only: 0.8 ± 1.3 mm; ACLPR-MR: 1.1 ± 1.2 mm; ACLPR-PME: 1.2 ± 1.4 mm; P = .34), overall reoperations, Lachman test results, pivot-shift test results, and PROMs (all P > .05).
Conclusion:
Meniscal repair with ACLPR is not associated with inferior clinical and patient-reported outcomes at the 2-year follow-up when compared with ACLPR-only and ACLPR-PME, with ACLPR-MR demonstrating a meniscal reinjury rate of 10.5%. These findings suggest that ACLPR provides sufficient knee stability to support clinically successful meniscal healing.
Meniscal tears commonly accompany anterior cruciate ligament (ACL) injuries, occurring in 49% to 61% of cases. 39 Surgical repair of traumatic meniscal tears is recommended to preserve meniscal integrity, improve anteroposterior and rotational knee stability, 52 reduce ACL graft failure risk, and protect articular cartilage to mitigate the progression of posttraumatic osteoarthritis.42,80 Concomitant meniscal repair at the time of ACL reconstruction (ACLR) is well established, with survival rates of 80% to 90%.12,66,77,90
However, residual laxity after ACLR, particularly with hamstring autografts,45,58 and persistent ACL deficiency have been linked to a higher risk of meniscal reinjury and impaired healing. 41 Similar concerns apply to ACL primary repair (ACLPR), which has reemerged as an alternative to ACLR in selected proximal tear patterns.11,19-21,48,73 Although biomechanical and clinical studies suggest that ACLPR restores stability with outcomes comparable to those of ACLR, a meta-analysis reported mixed findings, with some studies reporting greater residual laxity after ACLPR.19,21,61 Whether ACLPR provides sufficient stability to support meniscal healing remains unclear. Limited evidence exists, including a small cohort (n = 12) showing that meniscal repair with ACLPR may not be inferior to ACLR. 24 Additionally, recent findings have suggested that medial meniscus injuries are particularly associated with proximal ACL tears, typically suited for ACLPR, contradicting earlier reports.72,81 This highlights the clinical relevance and the need to clarify if meniscal tears can be addressed with ACLPR, or if concomitant meniscal injuries represent a relative contraindication.
Therefore, this study aimed to evaluate clinical outcomes after medial and/or lateral meniscus repair in patients undergoing ACLPR, compared with isolated ACLPR (ACLPR-only) and ACLPR with partial meniscectomy (ACLPR-PME). It was hypothesized that ACLPR with meniscal repair (ACLPR-MR) would yield comparable patient-reported outcomes to ACLPR-only and improved outcomes compared with ACLPR-PME at the 2-year follow-up.
Methods
Study Design
This study received institutional board approval before initiation (2017-0404), and informed consent was obtained by each patient in the study. Of the 646 consecutive patients with a complete ACL tear who underwent surgery between January 2008 and October 2021 and were prospectively enrolled in an institutional registry, 276 patients underwent ACLPR and completed a minimum 2-year follow-up (Figure 1). Outcomes on part of this cohort have been previously published.11,33,81,87 Patients were excluded if they received ACLR or ACLPR with autograft augmentation, had ipsilateral multiligamentous or contralateral injuries that required surgical intervention, or were skeletally immature. The surgical indication for ACL surgery was based on clinical examination, including the presence of subjective instability, an ATT SSD >3 mm measured using a Lachmeter (digital Rolimeter; Aircast Europa), and an ACL tear confirmed by magnetic resonance imaging.11,78,82,84 Indication for anatomic double-suture anchor ACLPR60,79 required a proximal, modified Sherman type 1 or 2 ACL tear location and good to excellent tissue quality (sufficient tissue integrity to hold sutures). 82 The decision to proceed with ACLPR was a multifactorial process. 48 While patient age, activity level, surgical delay, sex, body mass index (BMI), and concomitant cartilage or meniscal injuries were all considered during the indication process, 61 in this cohort, none of these were thought to be absolute contraindications or exclusion criteria in this study.
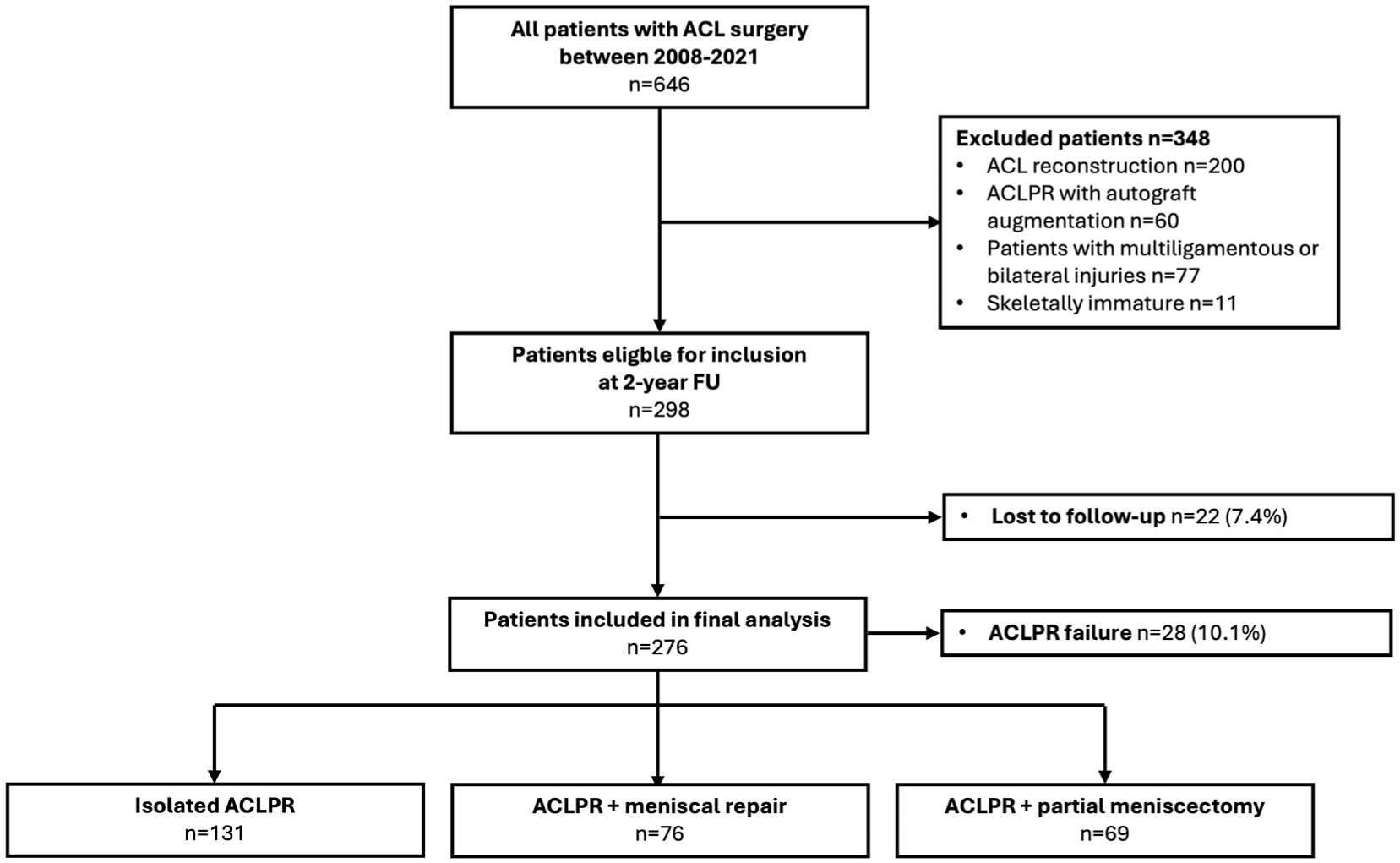
Study flowchart. ACL, anterior cruciate ligament; ACLPR, ACL primary repair; FU, follow-up.
To assess the success of meniscal repair, patients were divided into 3 groups according to meniscal treatments received: (1) ACLPR-only, (2) ACLPR with medial and/or lateral meniscus repair (ACLPR-MR), and (3) ACLPR with medial and/or partial meniscectomy (ACLPR-PME).
Treatment Algorithm and Surgical Technique
After informed consent from patients, all surgeries were performed by the senior author (G.S.D.). Intraoperative procedures began with the treatment of concomitant injuries including meniscal tears. 3 After initial debridement, traumatic meniscal lesions in the posterior or midsegment were addressed, in most cases using all-inside suture techniques, with 6 cases requiring inside-out repair. 88 In the case of radial tears, suture-based all-inside double vertical repair and horizontal suture anchor repair were the preferred techniques. 40 In particular, if the radial tear was located close to the meniscus root, “hash-tag” all-inside double vertical repair was performed. 40 Tears affecting the meniscus roots were addressed by transosseous root repair by placing luggage tag sutures into the root of the meniscus using an arthroscopic suture passer (Knee Scorpion; Arthrex).8,68 Next, the meniscus root guide was used to drill up into the root insertion. Using a lasso, we retrieved the meniscal repair stitches down and out the anterior tibia for later cortical fixation.8,68 Vertical tears were stabilized by placing horizontal all-inside suture anchors (Fast-Fix; Smith & Nephew) every 5 to 7 mm to sufficiently reduce the meniscal tear. 3 Ramp lesions were addressed primarily through a posteromedial portal with direct sutures using a suture hook and, if required, augmented with front-to-back all-inside suture anchor repair. 75 Traumatic horizontal meniscal tears were treated using either vertical all-inside suture repair or the vertical hay bale technique.5,7 In the case of bucket-handle tears, the meniscal fragment was first reduced, before being stabilized with often >6 horizontally placed all-inside suture anchors. 92 To address complex tears with various tear directions, the main tear component was first repaired, while small flaps, not suitable for repair, were removed. The repaired meniscus was assessed with the probe for sufficient stability. Meniscal repairs were not augmented with biological procedures. Degenerative tears, small radial tears, flap tears, and horizontal tears in the white-white zone or unstable tears after unsuccessful repair were treated with partial meniscectomy. 2
Arthroscopic anatomic ACLPR was performed using dual-suture anchor fixation (4.75-mm BioComposite SwiveLock suture anchor; Arthrex) and an arthroscopic suture passer to repair both ACL bundles individually with a Bunnell-type suture pattern.15,47,60 Beginning in 2015, suture augmentation using FiberTape (Arthrex) was selectively applied in high-risk patients and later adopted routinely.60,85 The augmentation suture was loaded into the anteromedial bundle suture anchor, passed through a 2.4-mm tibial drill hole in the anterior third of the distal ACL footprint, and independently tensioned in full extension to avoid overconstraint of the knee. 60
Rehabilitation
Full weightbearing as tolerated with unrestricted passive range of motion (ROM) was permitted immediately after surgery for patients undergoing ACLPR-only or ACLPR-PME. In cases of concomitant meniscal repair, weightbearing was limited to toe-touch (approximately 20% weightbearing) with an ROM limited to 0° to 90° for the first 4 weeks. A brace locked in extension was recommended until patients could comfortably perform 20 consecutive straight leg raises without lag (typically within 2-4 weeks), after which the brace was unlocked and gradually weaned until unrestricted walking was achieved. Rehabilitation followed a milestone approach, while return to pivoting sports was not recommended before 6 to 9 months. Return-to-sport decisions were based on standardized testing, including a required leg symmetry of at least 85%, in addition to other functional measures.
Clinical Outcome Assessment
Patients underwent routine postoperative clinical follow-up at 1, 4, and 8 weeks, as well as at 3, 6, 9, and 12 months. Follow-up extended for research purposes between a minimum of 2 and maximum of 5 years postoperatively, with all clinical examinations carried out by the senior author, including ATT SSD measurements, ROM, and Lachmann and pivot-shift grading. A standardized interview was used to assess for repair failure, reoperations, and subjective recurrent instability. ACL repair failure was defined as objective laxity (ATT SSD ≥3 mm, Lachman grade ≥2, and/or pivot-shift grade ≥2) or a symptomatic subjective feeling of instability. 11 Meniscal repair failure was defined as reoperation due to clinically symptomatic retear of the previously repaired meniscus. Patient-reported outcome measures (PROMs) included subjective International Knee Documentation Committee (IKDC) score, 26 Lysholm score, 37 Forgotten Joint Score–12 (FJS-12), 4 Anterior Cruciate Ligament Return to Sport after Injury (ACL-RSI) score, 89 and Tegner activity scale score. 74 Study-specific follow-up was not continued for patients who experienced ACLPR failure since ACLPR failure defines a study endpoint and these patients were subsequently treated nonoperatively or with surgical revision including ACLR or revision ACL repair.
Outcome Measures
The primary outcome measure at the 2-year follow-up was the IKDC score, which has been shown to be the most responsive outcome metric after meniscal surgery. 67 Secondary outcome measures consisted of meniscal and ACLPR failure, overall reoperation rates, ATT SSD, clinical outcomes (Lachmann and pivot-shift test results), and PROMs (Lysholm score, FJS-12, ACL-RSI score, and Tegner score).
Statistical Analysis
Normality of distribution of the samples was tested using the Shapiro-Wilk test. Normally distributed data in this study are expressed as mean with standard deviation or median with interquartile range. Two-way analysis of variance for nominal scaled data or the Pearson chi-square test and Fisher exact test for ordinal data were used (P < .05) to test for between-group differences in primary and secondary outcome measures. For the primary outcome measure, 95% confidence intervals and Cohen d were calculated for pairwise comparisons. Cox regression analysis was conducted to evaluate the relationship between patient age, BMI, surgical delay, postoperative Tegner score, and postoperative ATT SSD with the likelihood of meniscal repair failure as well as ACLPR failure. Based on the retrospective study design, all available data were analyzed and missing values, if any, were reported in results. As part of the study design, a sample size calculation was performed for comparing mean IKDC scores between 2 groups at a 2-year follow-up. Sample size calculation revealed that, based on the established MCID (IKDC score 10 ) of 11.5 points, an expected standard deviation of 15 points, a significance level of α = .05 (1-sided), a power of 0.9, and a group ratio of 2:1, 44 patients in the repair group and 22 patients in the control group were required. The sample size of the final cohort, as in a previous study, 21 was increased to allow potential subgroup analyses. Statistical analyses were performed using BlueSky Statistics (Version 10.3.4; R package Version 8.95).
Results
Of the 276 included patients, 131 underwent ACLPR-only, 76 underwent ACLPR-MR, and 69 underwent ACLPR-PME. The overall mean age was 39.7 ± 10.7 years, with 50.4% female patients. The mean follow-up was 2.9 ± 1.0 years for PROMs and 2.6 ± 1.0 years for clinical outcome measures. Follow-up data were unavailable for 22 of 298 patients (7.4%), who were consequently classified as lost to follow-up. An overview of baseline patient and clinical characteristics is provided in Table 1, and a detailed description of meniscal injury patterns and repair techniques is presented in Table 2.
Baseline Patient and Clinical Characteristics a

Data are presented as n (%) or mean ± SD unless otherwise indicated. Bold values denote statistical significance (P < .05). ACLPR, anterior cruciate ligament primary repair; ACLPR-MR, ACLPR with meniscal repair; ACLPR-PME, ACLPR with partial meniscectomy; ATT SSD, anterior tibial translation side-to-side difference; BMI, body mass index; NA, not applicable.
Post hoc analysis showed the following significant differences: ACLPR-only versus ACLPR-PME and ACLPR-MR versus ACLPR-PME.
Data is presented as median (interquartile range).
Post hoc analysis showed the following significant differences: ACLPR-MR versus ACLPR-PME.
Post hoc analysis showed the following significant differences: ACLPR-only versus ACLPR-MR and ACLPR-MR versus ACLPR-PME.
Meniscal Injury Patterns and Repair Data a

Overall 145 out of 276 patients (Groups ACLPR-MR+ACLPR-PME) had a meniscus injury (Table 1). Of the 145 patients, 37 had both menisci injured resulting in 182. Data are presented as n (%) or mean ± SD. Bold values denote statistical significance (P < .05). ACLPR, anterior cruciate ligament primary repair; ACLPR-MR, ACLPR with meniscal repair; ACLPR-PME, ACLPR with partial meniscectomy; NA, not applicable.
Tear type classification of the lateral meniscus was not feasible in 2 cases in the ACLPR-MR cohort and in 5 cases in the ACLPR-PME group.
Outcome Measures
At a minimum 2-year follow-up, IKDC scores demonstrated no significant differences between groups (ACLPR-only: 89.4 ± 10.3 [95% CI, 87.2-91.6]; ACLPR-MR: 86.7 ± 12.9 [95% CI, 83.6-89.8]; ACLPR-PME: 89.2 ± 9.9 [95% CI, 86.6-91.9]; P = .27) (Figure 2). Effect size analysis revealed only small differences between groups (Cohen d, 0.02-0.26). New meniscal injuries (no previous tear of the affected meniscus) occurred in 2 patients (2.3%) in the ACLPR-only group and 1 patient (1.4%) in the ACLPR-PME group (P > .37). In contrast, 8 patients (10.5%) in the ACLPR-MR group and 2 patients (2.9%) in the ACLPR-PME experienced meniscal reinjury (P = .10). In the ACLPR-MR group, the medial meniscus was affected in 6 of 8 cases (tear location: midbody, 3/6; posterior horn, 3/6; tear types: complex, 4/6; radial 1/6; flap, 1/6) and the lateral meniscus in 2 of 8 cases (tear location: midbody, 2/2; tear types: radial, 1/2; vertical 1/2). In the ACLPR-only group, 1 patient (0.8%) underwent medial meniscus repair, and 1 (0.8%) underwent combined medial and lateral partial meniscectomy at a mean of 3.8 ± 0.6 years postoperatively. In the ACLPR-MR group, 6 patients (7.9%) underwent medial and 2 (2.6%) lateral partial meniscectomies at a mean follow-up of 2.3 ± 1.5 years, while 2 patients (2.9%; 1 patient with a fresh medial meniscus tear and a reinjury of the lateral meniscus) in the ACLPR-PME group underwent additional partial meniscectomy. The surgical technique (with or without suture augmentation) did not have a significant effect on IKDC scores (P = .76) or meniscal repair failure rate (P = .42).

Box plot diagram of the subjective International Knee Documentation Committee (IKDC) score after isolated anterior cruciate ligament (ACL) primary repair (ACLPR-only), ACLPR with meniscal repair (ACLPR-MR), and ACLPR with partial meniscectomy (ACLPR-PME). X indicates mean value.
Kaplan-Meier survival analysis graphically presents a meniscal repair survival rate of 89.5% at the maximum follow-up of 4.9 years (Figure 3). During the 2- to 5-year follow-up period, Cox regression survival analysis revealed no significant covariates associated with meniscal repair failure (all P > .22) (Table 3). However, younger age was a significant and independent predictor for ACLPR failure (P < .01).

Kaplan-Meier survival analysis of meniscal repair in anterior cruciate ligament primary repair.
Cox Regression Analysis for Time to Meniscal Repair Failure With Covariate Adjustment a

Cox regression after adjusting for age, body mass index (BMI), surgical delay, postoperative anterior tibial translation side-to-side difference (ATT SSD), and postoperative Tegner score.
ACLPR failure occurred in 28 patients (10.1%), with no significant difference between groups (ACLPR-only: 9.9%; ACLPR-MR: 8.0%; ACLPR-PME: 12.9%; P = .62). However, patients with ACLPR failure were significantly younger (32.6 ± 9.3 years vs 40.5 ± 10.5 years; P < .01). ATT SSD measurements at the 2-year follow-up were available for 138 of 276 cases (50.0%) and demonstrated no significant differences (ACLPR-only: 0.8 ± 1.3 mm; ACLPR-MR: 1.1 ± 1.2 mm; ACLPR-PME: 1.2 ± 1.4 mm; P = .34). The surgical technique (with or without suture augmentation) did not have a significant effect on ACLPR failure rate (P = .17).
Contralateral ACL injuries were reported in 1 patient each from the ACLPR-only and ACLPR-MR groups, and in 2 patients from the ACLPR-PME group (P = .48). A single contralateral meniscal injury occurred in both the ACLPR-only and ACLPR-PME groups (P > .99). Other reoperations (overall reoperation rate: 8.0%, 22/276) consisted of <3 patients per group and were comparable across groups (overall: chondroplasty, 3/22; lysis of adhesions, 3/22; hardware removal, 2/22; all P > .37).
PROMs were available in 241 cases and clinical measures in 213 of 248 cases at the 2-year follow-up. No significant group differences were observed in ROM (P = .46), negative Lachman test rates (ACLPR-only: 91.0%; ACLPR-MR: 90.0%; ACLPR-PME: 84.3%; P = .21), negative pivot-shift tests (ACLPR-only: 93.3%; ACLPR-MR: 94.0%; ACLPR-PME: 84.3%; P = .31), or PROMs including the Lysholm score, postoperative Tegner level, Tegner difference (preoperative vs postoperative; ACLPR-only: –0.3 ± 0.9 ; ACLPR-MR: –0.6 ± 1.2 ; ACLPR-PME: –0.3 ± 1.0; P = .13), FJS-12, and ACL-RSI score (all P > .05) (Table 4).
Patient-Reported Outcome Measures a
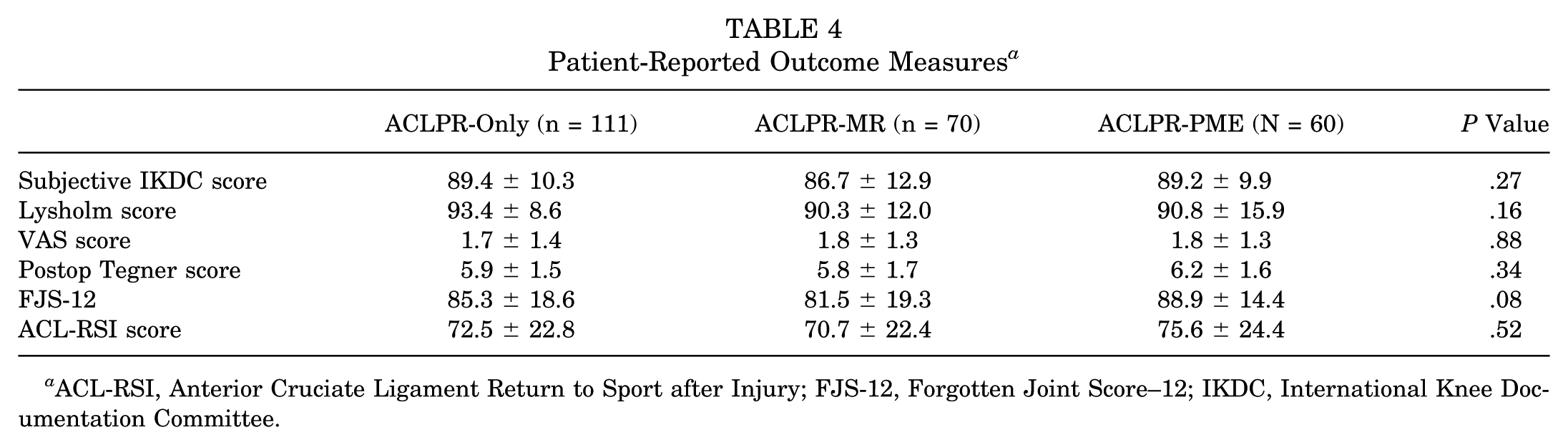
ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury; FJS-12, Forgotten Joint Score–12; IKDC, International Knee Documentation Committee.
Discussion
The most important finding of this study was that simultaneous meniscal repair with ACLPR did not negatively affect clinical and patient-reported outcomes at a minimum 2-year follow-up when compared with ACLPR-only and ACLPR-PME. Meniscal repair in the setting of ACLPR demonstrated an acceptable absence of clinical signs of meniscal reinjury in 89.5% of cases at a follow-up of 4.9 years. Interestingly, younger age was a significant predictor of ACLPR failure, but not of meniscal repair failure. Additionally, ATT SSD measurements and complication rates did not differ significantly across groups. These findings are clinically meaningful, as they suggest that ACLPR provides sufficient knee stability to support possible meniscal healing and that outcomes after meniscal repair with ACLPR are comparable to those reported for meniscal repair performed in conjunction with ACLR.
The failure rate of isolated meniscal repairs varies depending on tear type and timing of intervention, with reported rates ranging from 10% and 20% at the 2-year follow-up.12,18,55,65,66 Comparative studies have demonstrated that meniscal repairs performed concurrently with ACLR are associated with lower failure rates, suggesting an enhanced healing environment when combined with ACLR.31,90 It has also been suggested that concomitant meniscal tears in ACL-injured knees may exhibit distinct tear patterns, potentially influencing their reparability and healing response. 53 Importantly, there is limited research on meniscal repair performed simultaneously with ACLPR. In a small comparative study with 10 ACLPRs, Garside et al 24 observed no significant differences in meniscal repair failure rates and PROMs between ACLPR and ACLR. The meniscal repair failure rate of 10.5% observed in this study is comparable to those previously reported in ACLR,16,17,32,57,90 suggesting that ACLPR may offer adequate biomechanical stability to support meniscal healing in the setting of concomitant meniscal injury. Additionally, Conner-Rilk et al 11 reported no significant differences in reoperation rates after ACLPR between the 2- and 5-year follow-up (6.2% vs 7.5%; P = .71), with only 4.6% of patients requiring secondary meniscal procedures at a mean follow-up of 6 years. Studies assessing outcomes 5 years after dynamic intraligamentary stabilization (DIS), including ACL injuries with and without concomitant meniscal injuries, have reported reoperation rates ranging from 12% to 38% (secondary meniscal injury: 3%-4%).25,28 Reoperation rate due to meniscal reinjury after Bridge-Enhanced ACL Restoration (BEAR) occurred in 11% to 18%.23,50,91 Utoyo et al 76 reported a cumulative incidence of subsequent meniscal injuries of 7%, based on a meta-analysis of various repair techniques. In contrast, failure rates for meniscal repair in ACL-deficient knees have been reported to be as high as 27% to 37%,35,38 highlighting the importance of addressing instability in promoting meniscal healing.
Furthermore, this study found no significant differences in PROMs or knee laxity at a 2-year follow-up between patients who underwent meniscal repair and those who underwent partial meniscectomy, with a meniscal reinjury rate of 10.5% after repair. Importantly, as demonstrated by Ronnblad et al, 63 patients with failed meniscal repairs may experience worse outcomes than those with meniscal injuries, which were left untreated, which could explain the slightly lower FJS-12 and ACL-RSI scores observed in the ACLPR-MR group, despite overall comparable PROMs between groups in this study. This ACLPR-MR group included patients with failed meniscal repairs, potentially contributing to outcomes in this cohort. Unlike findings from biomechanical studies that assessed meniscus-deficient knees,36,52 in the present study, patients underwent only partial meniscectomy, which may explain the comparable knee stability observed between ACLPR-MR and ACLPR-PME. While partial meniscectomy often provides short-term symptom relief and carries a lower risk of reoperation,55,70 meniscal repair has been associated with improved long-term outcomes and a reduced incidence of posttraumatic osteoarthritis.44,56
Several factors, including anatomic reduction, favorable biological environment, and adequate compression, are considered fundamental for successful healing after meniscal repair.27,80 In the setting of ACL injury, further procedure-related factors such as the release of growth factors through tunnel drilling, 14 delay of surgery, and improved joint stability after ACL surgery may influence the healing potential of meniscal tears.54,56 Patient age is considered a risk factor for ACL reinjury, which is confirmed in the current study.29,61 Therefore, it can be proposed that the higher mean age may have been protective for contralateral ACL injury. 71 However, the preservation of proprioception with primary repair of the ACL contributes to a more natural gait pattern, where patients are less aware of their operated knee, which may in turn reduce the incidence of contralateral ACL injury as well.6,30,86 As in previous studies,57,62 the current analysis found that patient age did not significantly affect meniscal repair outcomes. Younger patients are often thought to have a higher risk of failure due to increased activity levels and a greater likelihood of reinjury.29,58,62,64 In contrast, older patients may face a higher risk due to diminished biological healing potential.43,62 A significant advantage of ACLPR over ACLR is that ACLPR is typically performed within 4 weeks of injury to preserve the likelihood of repairability of the native ACL. 81 This has several advantages as early surgery is associated with (1) a lower incidence of meniscal injuries,13,46 especially ramp lesions, as these can occur with ongoing instability; (2) a higher likelihood of repairable meniscal tears69,77; and (3) a higher likelihood of healing of repaired meniscal lesions.77,83 In contrast to ACLPR, surgeons often prefer to delay ACLR to reduce the risk of arthrofibrosis, but this has the abovementioned disadvantages.1,34 As ACLPR is often preferred in the early phases after injury to avoid ligament retraction, 51 this might explain why our noted failure rate of 10.5% is relatively low compared with the failure rates of meniscal repair in the ACLR setting. The overall low rate of arthrofibrosis (1.1%) despite early ACLPR suggests that early intervention may be both safe and beneficial in preserving meniscal integrity.11,91
The research question in this study is clinically relevant, as concerns remain regarding whether ACLPR provides sufficient anteroposterior and rotational stability to support meniscal healing. However, clinical time-zero and biomechanical studies have demonstrated that ACL repair techniques, using single- or double-suture anchor fixation or cortical fixation, can achieve anterior knee stability comparable to the ACL intact state and ACLR.9,49,59 Clinical evidence has been provided by a recent meta-analysis finding no significant difference in ATT SSD between ACLR and ACL repair techniques, differentiated for ACLPR, DIS, and BEAR. 61 Another meta-analysis pooling various ACL repair techniques found significantly higher residual laxity for ACL repair; however, subgroup analysis revealed that this was primarily driven by studies involving DIS and the internal brace technique, while studies investigating suture anchor fixation and BEAR showed no significant difference compared with ACLR. 76 In the present study, the observed mean ATT SSD of 1.1 ± 1.2 mm in the ACLPR-MR group, which is well below the clinical threshold of 3 mm, supports these findings. Interestingly, ATT SSD in the ACLPR-PME group was slightly higher, although not significantly, suggesting that meniscal repair may contribute to reduced ATT SSD. This aligns with the results of Fithian et al 22 and biomechanical studies.36,54
Limitations
This study has limitations. First, although this study demonstrates that meniscal repair performed concurrently with ACLPR can yield favorable outcomes, there is no direct comparison with ACLR with meniscal repair, although many studies in the literature have previously assessed this.31,58,90 Second, the rationale behind the decision to repair or not repair certain tears remains unclear and may be influenced by potential confounding variables such as patient age and BMI. A matched-pair analysis may strengthen conclusions of future studies. Third, the retrospective study design, the high median age of the patients, and the single-surgeon design may limit the generalizability of the findings and may have biased the results. Fourth, the lack of postoperative imaging to objectively confirm meniscal healing limits the ability to comprehensively evaluate the success of meniscal repair with simultaneous ACLPR. Fifth, the absence of objective ATT SSD measurements for some patients may compromise the validity of conclusions related to joint stability. Sixth, the short-term follow-up does not allow evaluation of the long-term benefits of meniscal repair compared with partial meniscectomy on PROMs.
Conclusion
Meniscal repair with ACLPR is not associated with inferior clinical and patient-reported outcomes at 2-year follow-up when compared with ACLPR-only and ACLPR-PME, with ACLPR-MR demonstrating a meniscal reinjury rate of 10.5%. These findings suggest that ACLPR provides sufficient knee stability to support clinically successful meniscal healing.
Footnotes
Final revision submitted November 4, 2025; accepted November 10, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.D. receives royalties, owns stock, and is a paid consultant for Zimmer Biomet; receives royalties from Arthrex; received stock options, provides consulting services, and participates in funded research with Miach Orthopaedics; and receives stock options and provides consulting services for OSSIO. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional review board (2017-0404).