
Abstract
Background:
Acromioclavicular joint (ACJ) reconstruction has been widely studied; however, the methodological quality of its most cited research remains uncertain. Citation-based analyses have emphasized the influence of frequently cited studies.
Purpose:
To (1) identify the 50 most cited original studies on ACJ reconstruction and assess their methodological quality using established scoring systems, and (2) explore correlations between study quality, citation count, and citation density.
Study Design:
Cross-sectional study.
Methods:
A Web of Science search (1946-August 2024) identified publications on ACJ reconstruction. The 50 most cited articles were analyzed for bibliographic details, citation metrics, and level of evidence (LOE). Clinical studies were assessed using the Modified Coleman Methodology Score (MCMS), Methodological Index for Non-Randomized Studies (MINORS), and Methodological Quality for Clinical Studies of Radiologic Examinations (MQCSRE). Cadaveric studies were evaluated using the Biomechanics Objective Basic Science Quality Assessment Tool (BOBQAT).
Results:
The 50 most cited articles garnered 5918 citations, with a mean of 118 ± 62 citations per article. Most articles were published in the American Journal of Sports Medicine, accounting for 56% of the total (n = 28). Clinical studies accounted for 66% (n = 33) of the articles, while cadaveric studies comprised 34% (n = 17). The United States was the leading contributor (44%; n = 22), followed by Germany (22%; n = 11). Significant correlations were observed between citation counts and the MINORS (r = 0.37; P < .05) scores and LOE (r = −0.37; P < .05). No significant correlations were found between citation counts and the MCMS (r = 0.24; P > .05), MQCSRE (r = 0.20; P > .05) or BOBQAT (r = −0.22; P > .05). Analysis of citation density indicated that recent decades (2011-2020) showed increased values, showing trends in research activity.
Conclusion:
Study quality was partially correlated with citation counts among highly cited clinical studies on ACJ reconstruction. The overall methodological quality was moderate, highlighting the need for higher-level evidence. This article serves as a reference for key literature.
Acromioclavicular joint (ACJ) instability is a common injury in young and active individuals, particularly athletes.11,31 Recommendations for the management of these injuries are typically nonsurgical for Rockwood types 1 to 3, while contemporary evidence still supports a surgical treatment of high-grade (Rockwood type 4-6) injuries in specific cases.3,6 Regarding operative treatment, various surgical techniques have been developed to restore ACJ function.8,14,16,25 In addition, the development of new implant materials has advanced surgeons' reconstruction efforts and strategies over the last decades.15,27,36
Given the enormous interest in ACJ injuries, a plethora of clinical and biomechanical studies have examined reconstruction techniques.15,34,37 More specifically, >2000 articles have been published concerning the ACJ since 1912 on the National Center for Biotechnology Information PubMed, half of which have been published over the last 10 years. As the overwhelming number of studies may introduce complexity and confusion to the readership, bibliometric analysis offers a valuable tool for identifying critical influential articles by focusing on citation metrics.1,2,18,19,20,33 Such analyses not only give an overview of the essential works, research trends, and centers of competence in the field but also provide a rough estimate of the study quality, as frequently cited articles tend to reflect those that have significantly shaped clinical practices or research directions.22,33 However, citation counts do not always directly correlate with methodological quality, making it even more important to assess the quality of these highly cited papers.4,21
Thus, this study aimed to (1) identify the 50 most cited papers on ACJ reconstruction along with their bibliographic metrics, and (2) assess the correlation between study quality, citation count, and citation density among these studies. It was hypothesized that citations would not correlate with the study quality.
Methods
Literature Search
A thorough examination of the Clarivate Analytics Web of Science (WoS) database was conducted in August 2024 by 1 reviewer (H.J.C.). All studies published from 1946 until 8 August 2024, identified by applying the search term acromioclavicular joint with accessible English-language abstracts, were included. The results were then refined based on citation count and ranked in descending order. A data sheet was used to record all identified studies and bibliometric details—such as author name, publication year, journal, title, abstract, total citations (across all databases), and language. A comparison with Elsevier's Scopus database revealed almost identical results for the search term acromioclavicular joint; thus, no further extraction was conducted. Additionally, a PubMed search using the same term (acromioclavicular joint) was performed, which revealed no additional highly cited studies beyond those identified in WoS and Scopus. This confirmed the dataset's completeness and reliability.
Inclusion and Exclusion Criteria
The following inclusion criteria were applied to the 2038 identified studies: Only English-language studies published in international, peer-reviewed journals from 1946 to August 2024, with acromioclavicular joint in the title or abstract, were initially considered. The abstracts of all studies were screened to identify those relevant to acromioclavicular joint reconstruction. Records were then ranked in descending order of citation count, and the last 1939 studies were excluded, leaving the top 99 most-cited studies for further screening. Studies published in journals unrelated to the medical field or the topic of ACJ reconstruction were excluded. Subsequently, articles primarily focused on reviews, meta-analyses, or surgical techniques were excluded since this research specifically emphasizes original work. The detailed selection process for the study is shown in Figure 1.
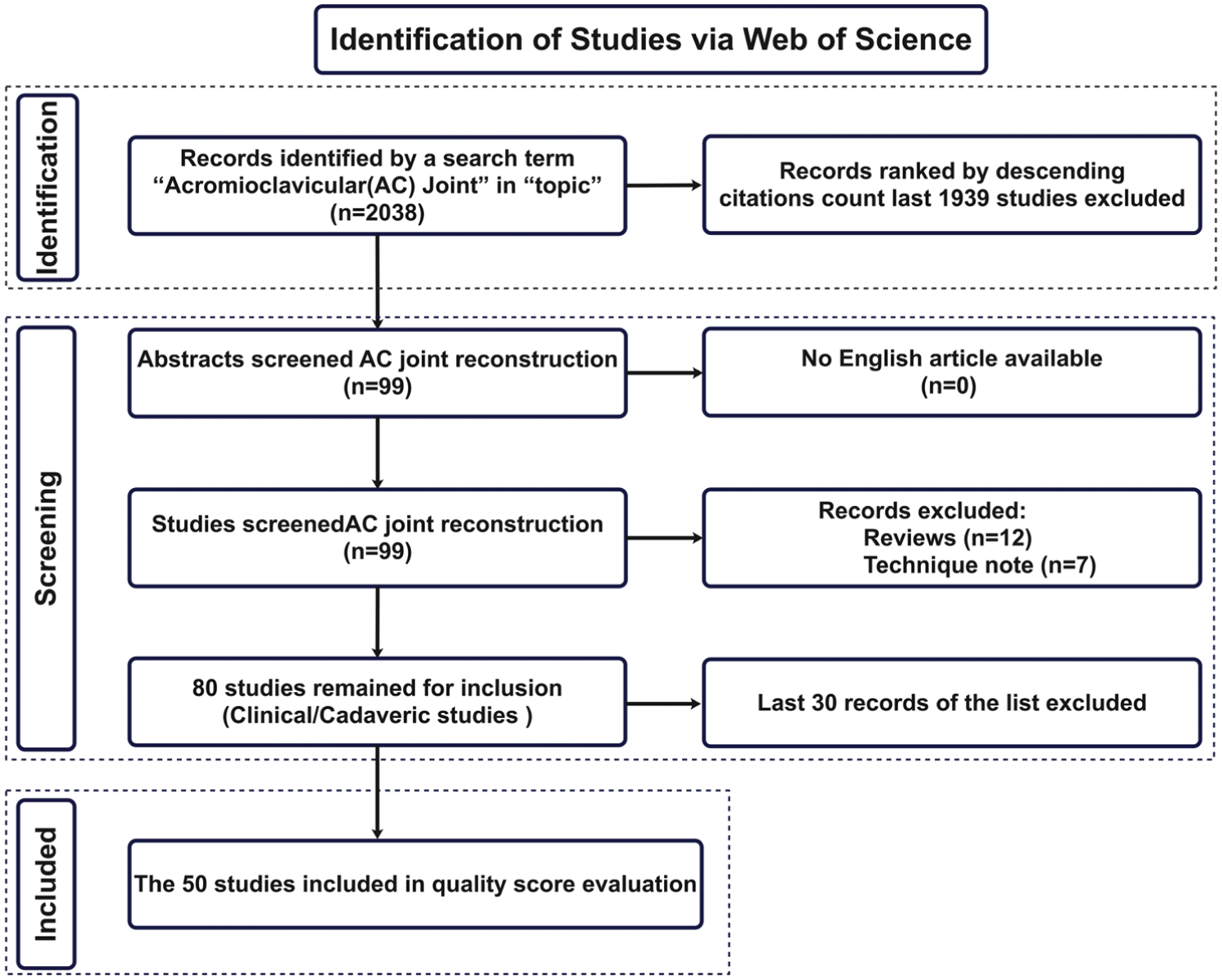
PRISMA flowchart demonstrating the article selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data Assessment
Three authors (H.J.C., R.V., and A.P.) comprehensively evaluated the included studies—including the total citation count, journal and Journal Impact Factor (JIF), study type, country of origin of the institution where the study was performed, and year of publication. To account for the tendency of older studies to accumulate more citations, citation density (total citations divided by the number of years since publication) was also provided. Additionally, the temporal distribution of citations was analyzed by grouping studies into publication periods and calculating the total citations for each period to identify trends over time.
Quality assessment of the 50 most-cited studies was conducted using the Level of Evidence (LOE) rating. 23 For clinical studies, the Modified Coleman Methodology Score (MCMS) 9 and the Methodological Index for Non-Randomized Studies (MINORS) 29 were obtained. The MCMS (range, 0-100 points) particularly focuses on adequate sample size, follow-up rates, diagnostic approaches, and well-defined rehabilitation protocols. The MINORS score can be divided into 2 parts: The first part (range, 0-16 points) is obtained for all clinical studies, and the optional second part (range, 16-24 points) is further obtained for comparative studies.
The Methodological Quality for Clinical Studies of Radiologic Examinations (MQCSRE) 5 was used to assess the quality of radiological studies (range, 0-30 points). Finally, the recently published and validated Biomechanics Objective Basic Science Quality Assessment Tool (BOBQAT) 12 was used to assess biomechanical studies (range, 0-100 points). This quality score evaluates elements such as specimen preparation, the reproducibility of the testing setup, and, if appropriate, whether biomechanical measures are performed. Each scoring tool was applied according to its intended study type. The MCMS, MINORS, and MQCSRE were used for clinical studies, whereas the BOBQAT was applied to biomechanical cadaveric studies. As these instruments assess different methodological domains, their scores are not directly comparable.
Statistical Analysis
Statistical analysis was performed using SPSS, Version 31.0 (IBM Corp). Graphical representations and figure preparation were conducted using GraphPad Prism, Version 10.0 (GraphPad Software), and R software, Version 4.3.0 (R Foundation for Statistical Computing). Because of the study design, the sample size was limited to the 50 most-cited studies on ACJ reconstruction. The Shapiro-Wilk test was used to assess whether the data were normally distributed. As none of the variables exhibited normal distribution, comparisons of citation count or citation density between different journals, study types, scales, and countries were conducted using the Mann-Whitney U test or the Kruskal-Wallis test for comparisons involving >2 groups. Statistical significance was set at P < .05. Two independent raters (H.J.C. and A.P.)) assessed the methodological quality of the included studies using 4 scoring systems: MCMS, MINORS, MQCSRE, and BOBQAT. The correlation between citation counts and quality scores was analyzed using the Spearman rank correlation coefficient. Interrater reliability was evaluated using the intraclass correlation coefficient (ICC) for these continuous scores, with interpretation based on the guidelines by Koo and Li 13 : ICC <0.5 indicates poor, 0.5-0.75 moderate, 0.75-0.9 good, and >0.9 excellent reliability.
Results
The studies were published in 10 journals, with the majority in the American Journal of Sports Medicine (Am J Sports Med), accounting for 56% (n = 28) (Figure 2). The mean JIF among publishing journals was 4.4 ± 0.8 (range, 2.1-5.4). While the majority of studies (56%) were published in Am J Sports Med, 78% appeared in journals with a JIF ≥4.5.

Distribution of the top 50 studies by journal of publication and 2024 Journal Impact Factor (2024 JIF): Am J Sports Med, American Journal of Sports Medicine; Ann Biomed Eng, Annals of Biomedical Engineering; Arch Orthop Trauma Surg, Archives of Orthopaedic and Trauma Surgery; Arthroscopy, Arthroscopy: The Journal of Arthroscopic and Related Surgery; Clin Orthop Rel Res, Clinical Orthopaedics and Related Research; Eur J Med Res, European Journal of Medical Research; J Bone Joint Surg Am, Journal of Bone and Joint Surgery American Volume; J Shoulder Elbow Surg, Journal of Shoulder and Elbow Surgery; Knee Surg Sports Traumatol Arthrosc, Knee Surgery Sports Traumatology Arthroscopy; Orthop Traumatol Surg Res, Orthopaedics & Traumatology: Surgery & Research.
Among the 50 most cited studies, 2 main study types were identified: clinical studies accounted for 67% (n = 33), and cadaveric studies comprised 33% (n = 17). In the clinical studies, 11 (33%) were prospective, while 22 (67%) were retrospective. Additionally, 10 studies (30%) were classified as comparative and 23 (70%) as noncomparative, based on study design criteria. The remaining 17 studies (34%) were designed as cadaveric biomechanical studies (Figure 3A). Regarding the LOE, 21 studies were classified as level 4 (42%), followed by level 3 (n = 10; 20%) and level 2 (n = 2; 4%) (Figure 3B). The 50 most cited articles were collectively published by institutions from 13 countries. The United States contributed the largest number of studies, accounting for 22 (44%), followed by Germany with 11 (22%), Switzerland with 3 (n = 6%), and the Republic of Korea with 3 (6%) (Figure 4A). Other countries—including the United Kingdom, Hungary, the Netherlands, Australia, Spain, Italy, France, and Greece—each contributed 1 study (2%) to the top 50 list. The continental distribution is shown in Figure 4B.

(A) Distribution by study types is as follows: clinical comparative (Clin Comp); clinical non-comparative (Clin Non-Comp); prospective (Clin Pros); retrospective (Clin Retro); and cadaveric studies. The numbers represent the counts of studies by type, not the total number of included studies. (B) Distribution by level of evidence (LOE).

The top 50 studies, sorted by (A) country and (B) continent of origin. Others include the United Kingdom, Hungary, the Netherlands, Australia, Spain, Italy, and Greece. North America (NA), Europe (EU), Oceania (OC), and Asia (AS).
Study Quality
A comprehensive list of the 50 most cited studies, along with their corresponding quality scores (MCMS, MINORS, MQCSRE, LOE, and BOBQAT), is provided in Table 1. In clinical studies, the mean MCMS 9 score was 66.6 ± 7.4 (range, 50-81), indicating moderate methodological quality. For noncomparative studies, the mean MINORS 29 score was 11 ± 1.8 (range, 8-14), and comparative studies scored a mean of 18.3 ± 2.7 points (range, 13-22), indicating high-quality standards. For studies with a radiological focus, the mean MQCSRE 5 score was 19 ± 2.8 (range, 14-24). For biomechanical studies, the mean BOBQAT 12 score was 77.9 ± 13.8 (range, 33- 94), highlighting the high study quality across these studies (Table 2).
Comprehensive List of the 50 Most Cited Studies on ACJ Reconstruction a
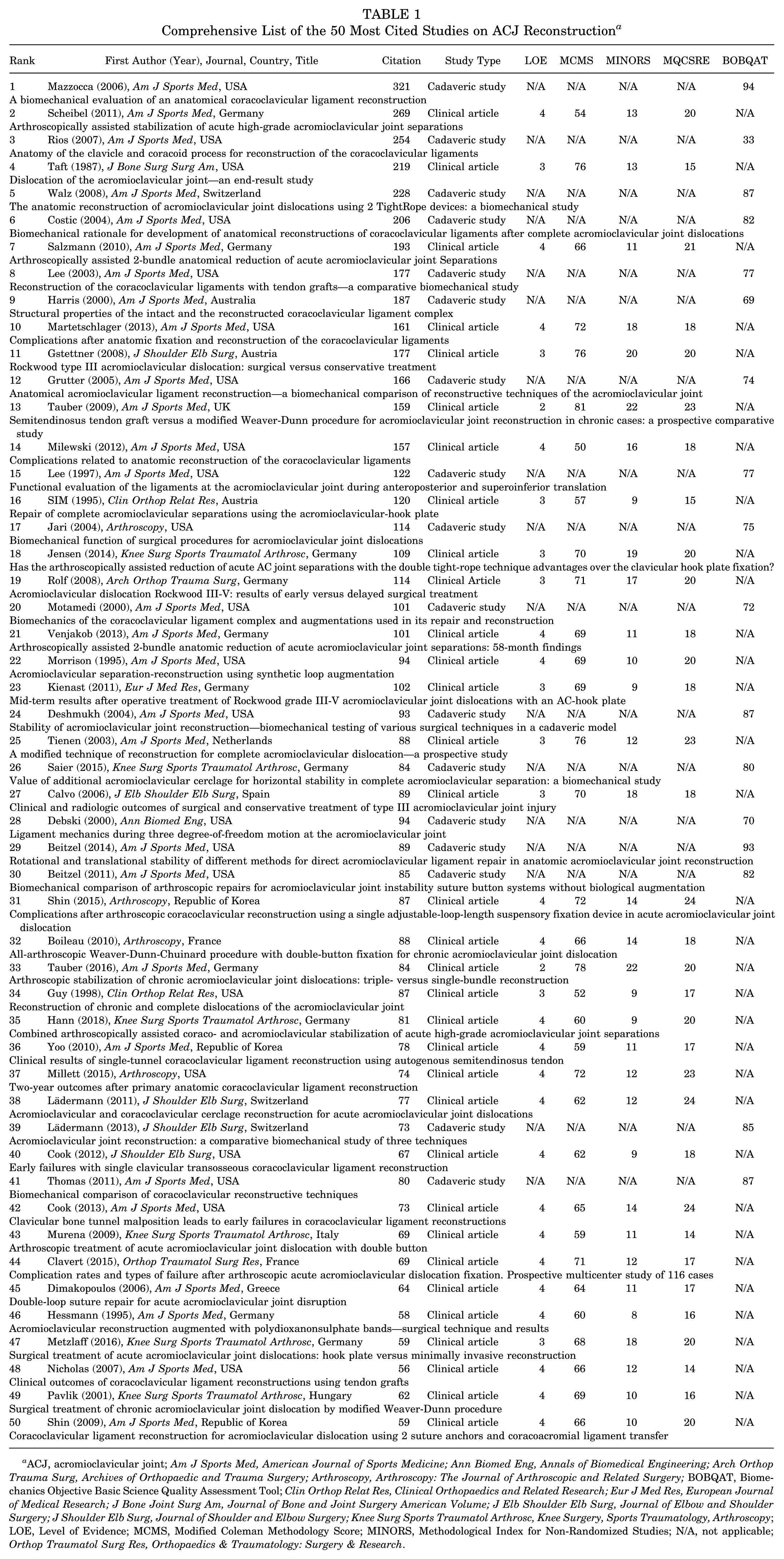
ACJ, acromioclavicular joint; Am J Sports Med, American Journal of Sports Medicine; Ann Biomed Eng, Annals of Biomedical Engineering; Arch Orthop Trauma Surg, Archives of Orthopaedic and Trauma Surgery; Arthroscopy, Arthroscopy: The Journal of Arthroscopic and Related Surgery; BOBQAT, Biomechanics Objective Basic Science Quality Assessment Tool; Clin Orthop Relat Res, Clinical Orthopaedics and Related Research; Eur J Med Res, European Journal of Medical Research; J Bone Joint Surg Am, Journal of Bone and Joint Surgery American Volume; J Elb Shoulder Elb Surg, Journal of Elbow and Shoulder Surgery; J Shoulder Elb Surg, Journal of Shoulder and Elbow Surgery; Knee Surg Sports Traumatol Arthrosc, Knee Surgery, Sports Traumatology, Arthroscopy; LOE, Level of Evidence; MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-Randomized Studies; N/A, not applicable; Orthop Traumatol Surg Res, Orthopaedics & Traumatology: Surgery & Research.
Mean Quality Scores of the Top 50 Most Cited Articles a
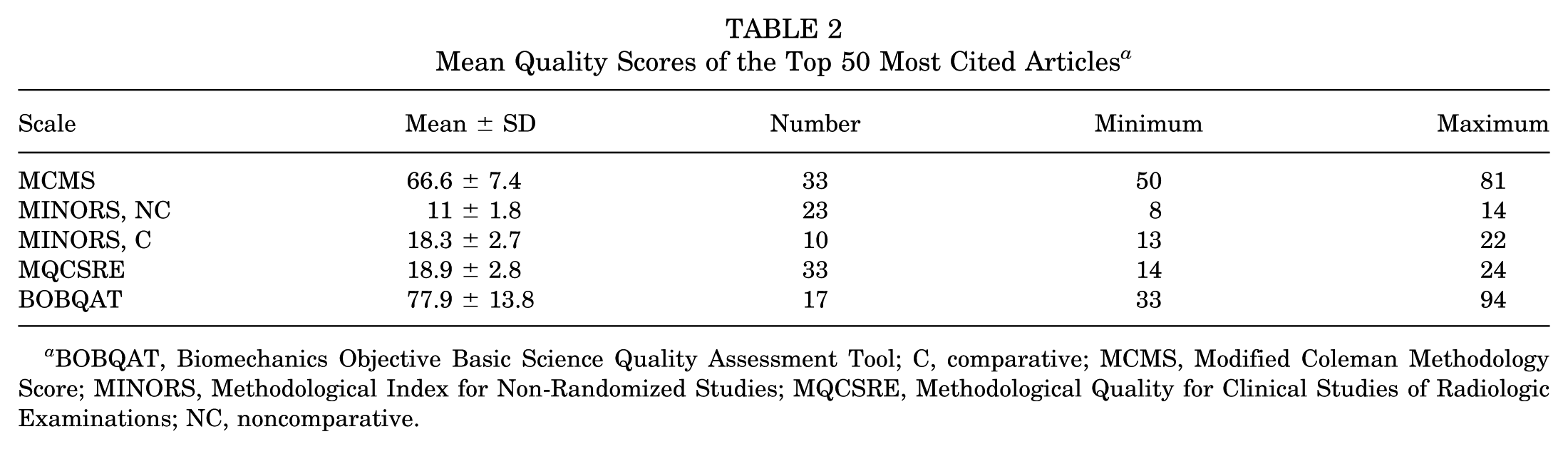
BOBQAT, Biomechanics Objective Basic Science Quality Assessment Tool; C, comparative; MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-Randomized Studies; MQCSRE, Methodological Quality for Clinical Studies of Radiologic Examinations; NC, noncomparative.
Interrater reliability between the 2 independent assessors (H.J.C. and A.P.) was evaluated using the ICC for each scoring system. The mean of the measured ICCs indicated good to excellent reliability across all 4 quality assessment tools. Specifically, the ICC was 0.883 (95% CI, 0.737-0.945) for the MCMS, 0.780 (95% CI, 0.559-0.891) for the MINORS, 0.802 (95% CI, 0.501-0.912) for the MQCSRE, and 0.913 (95% CI, 0.762-0.968) for the BOBQAT. All ICC values were statistically significant (P < .001), indicating high consistency among raters.
Citation Analysis
The total citation count for the 50 most cited studies on acromioclavicular (AC) joint and coracoclavicular (CC) ligament reconstruction was 5918, with a mean of 118.4 ± 62.1 citations per article. Of these, the Am J Sports Med accounted for the largest portion, contributing 64.3% (3803 citations), followed by the J Shoulder Elbow Surg, with 8.2% (483 citations), and Knee Surg Sports Traumatol Arthrosc, with 7.8% (464 citations), and Arthroscopy, with 6.1% (363 citations) (Figure 5A). Am J Sports Med had the highest citation density at 8.7 ± 4.9 citations per year, followed by Knee Surg Sports Traumatol Arthrosc (8.1 ± 4 per year) and Eur J Med Res (7.9 per year) (Figure 5B).

(A) Total citations and (B) citation density of journals that published the 50 most cited studies on AC and CC joint reconstruction. (C) Sum of citations distributed by decade of publication. (D) Citation density by decade of publication. Am J Sports Med, American Journal of Sports Medicine; Ann Biomed Eng, Annals of Biomedical Engineering; Arthroscopy, Arthroscopy: The Journal of Arthroscopic and Related Surgery; Arch Orthop Trauma Surg, Archives of Orthopaedic and Trauma Surgery; Clin Orthop Rel Res, Clinical Orthopaedics and Related Research; Eur J Med Res, European Journal of Medical Research; J Bone Joint Surg Am, Journal of Bone and Joint Surgery American Volume; J Shoulder Elbow Surg, Journal of Shoulder and Elbow Surgery; Knee Surg Sports Traumatol Arthrosc, Knee Surgery Sports Traumatology Arthroscopy; Orthop Traumatol Surg Res, Orthopaedics & Traumatology: Surgery & Research.
When analyzing the sum of citations by publication year (Figure 5C), the period 2001-2010 had the highest number of citations, totaling 2855. Additionally, studies published during 2011-2020 collectively recorded 1981 citations, representing a decline compared with the previous decade but still maintaining a significant citation count. However, the mean citation density per study was highest among papers published in the most recent decade (2011-2020), with a mean density of 9.5 ± 3.7 citations per year. This was closely followed by the period 2001-2010, with a citation density of 7.9 ± 4.4. The earlier periods (1991-2000 and 1981-1990) exhibited much lower citation densities of 4.2 ± 1.7 and 5.9 ± 0, respectively (Figure 5D).
When comparing study types, biomechanical studies were significantly more frequently cited than clinical studies (145.5 ± 73 vs 104.4 ± 51.4; P = .014) (Figure 6A). The citation density did not differ significantly between the 2 study types, with clinical studies averaging 7.6 ± 4.2 and cadaveric studies 8.4 ± 4 (P = .390) (Figure 6B). Comparing prospective and retrospective studies, there was no statistically significant difference in citation counts (123.2 ± 64.9 vs 94.9 ± 41.7; P = .204) (Figure 6C). However, citation density was significantly higher in prospective studies compared with retrospective studies (10.1 ± 4.9 vs 6.4 ± 3.2; P = .032) (Figure 6D).
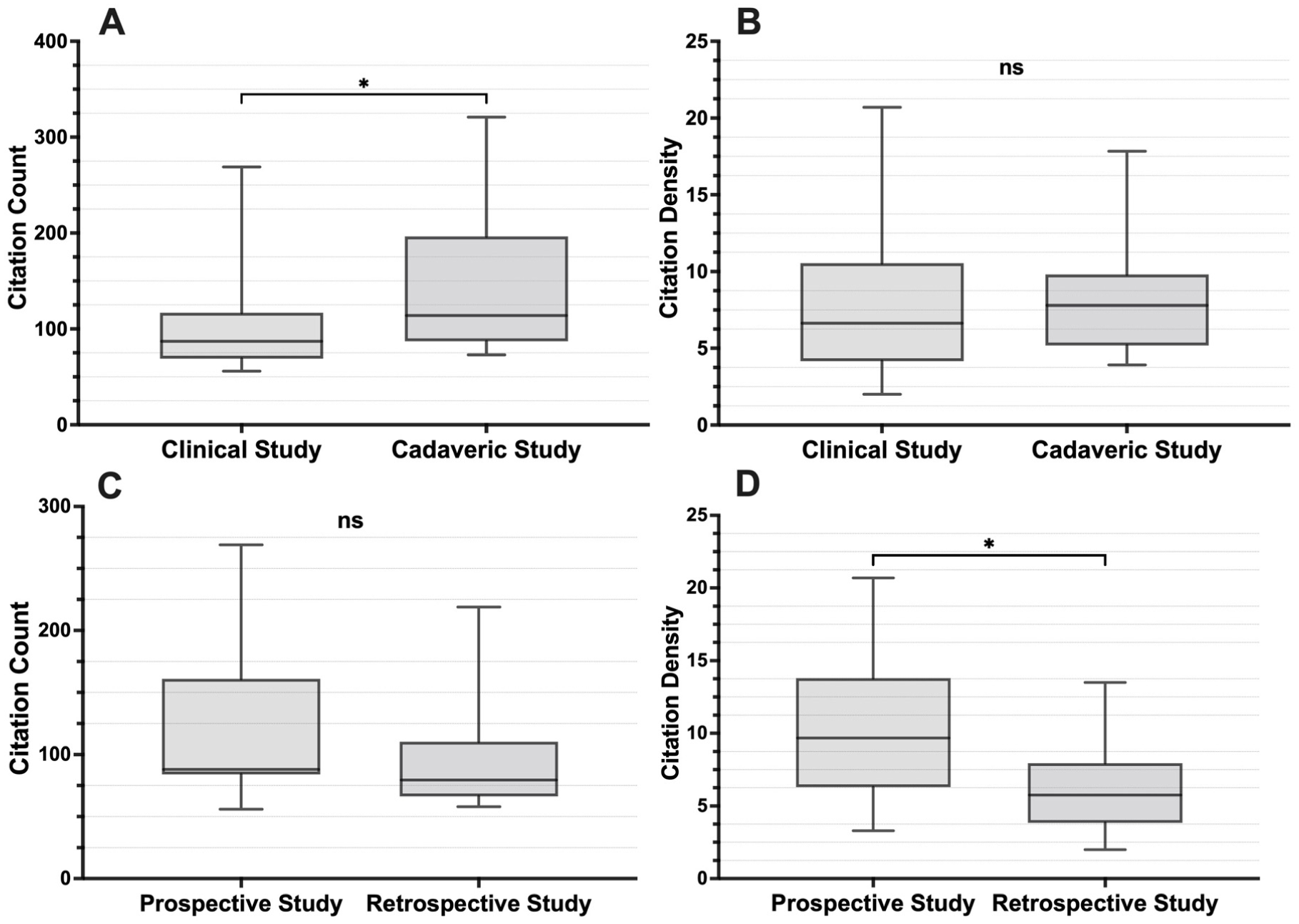
Comparison of citation metrics of the 50 most cited studies in ACJ reconstruction between (A and B) clinical and cadaveric studies and between (C and D) prospective and retrospective studies. Statistically significant differences (P < 0.05) are indicated by an asterisk (*), while ns denotes nonsignificant differences (P≥ .05).
Correlation analysis of citation counts and quality assessment scores (MCMS, MINORS, MQCSRE, LOE, and BOBQAT) and country of origin for the top 50 most cited studies is shown in Table 3 and Figure 7. Among them, the MINORS score showed a statistically significant positive correlation with citation count (r = 0.37; P = .036) (Figure 7B). Similarly, the LOE demonstrated a significant negative correlation with citation count (r = −0.37; P = .032), indicating that studies with higher levels of evidence (ie, lower LOE score) were more frequently cited (Figure 7D). No statistically significant correlation was observed between citation count and the MCMS (r = 0.24; P = .180) (Figure 7A), MQCSRE (r = 0.20; P = .256) (Figure 7C), or BOBQAT (r = −0.22; P = .399) scores (Figure 7E). Regarding regional distribution, North America shows the highest citation counts with broad distribution; Europe and Oceania have moderately concentrated citations; and Asia has the lowest and narrowest distribution (Figure 7F).
Correlation of Citation Count and Methodological Quality Scores a

Bold P values indicate statistical significance. BOBQAT, Biomechanics Objective Basic Science Quality Assessment Tool; LOE, Level of Evidence; MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-Randomized Studies; MQCSRE, Methodological Quality for Clinical Studies of Radiologic Examinations.

Scatter plots demonstrating the correlation between citation count and each methodological quality score. (A) MCMS, (B) MINORS, (C) MQCSRE, (D) LOE, (E) BOBQAT score. (F) This boxplot illustrates the citation counts of articles from 4 continents: North America, Europe, Oceania, and Asia. Correlation coefficients and P values were determined using the Spearman rank correlation. Significant associations were found between citation count and the MINORS score (P = .036) and LOE (P = .032). No significant correlations were observed for the MCMS, MQCSRE, or BOBQAT. BOBQAT, Biomechanics Objective Basic Science Quality Assessment Tool; LOE, Level of Evidence; MCMS, Modified Coleman Methodology Score; MINORS, Methodological Index for Non-Randomized Studies; MQCSRE, Methodological Quality for Clinical Studies of Radiologic Examinations.
The Sankey diagram (Figure 8) illustrates the allocation of the 50 most-cited articles in ACJ reconstruction research. The data flow starts with study types (Cadaveric Study and Clinical Article), then passes through journal abbreviations, decades, countries, and ends with continents. The width of the flow lines represents the quantity in each category, highlighting the relationships between study types, journal preferences, temporal trends, and geographic origins.
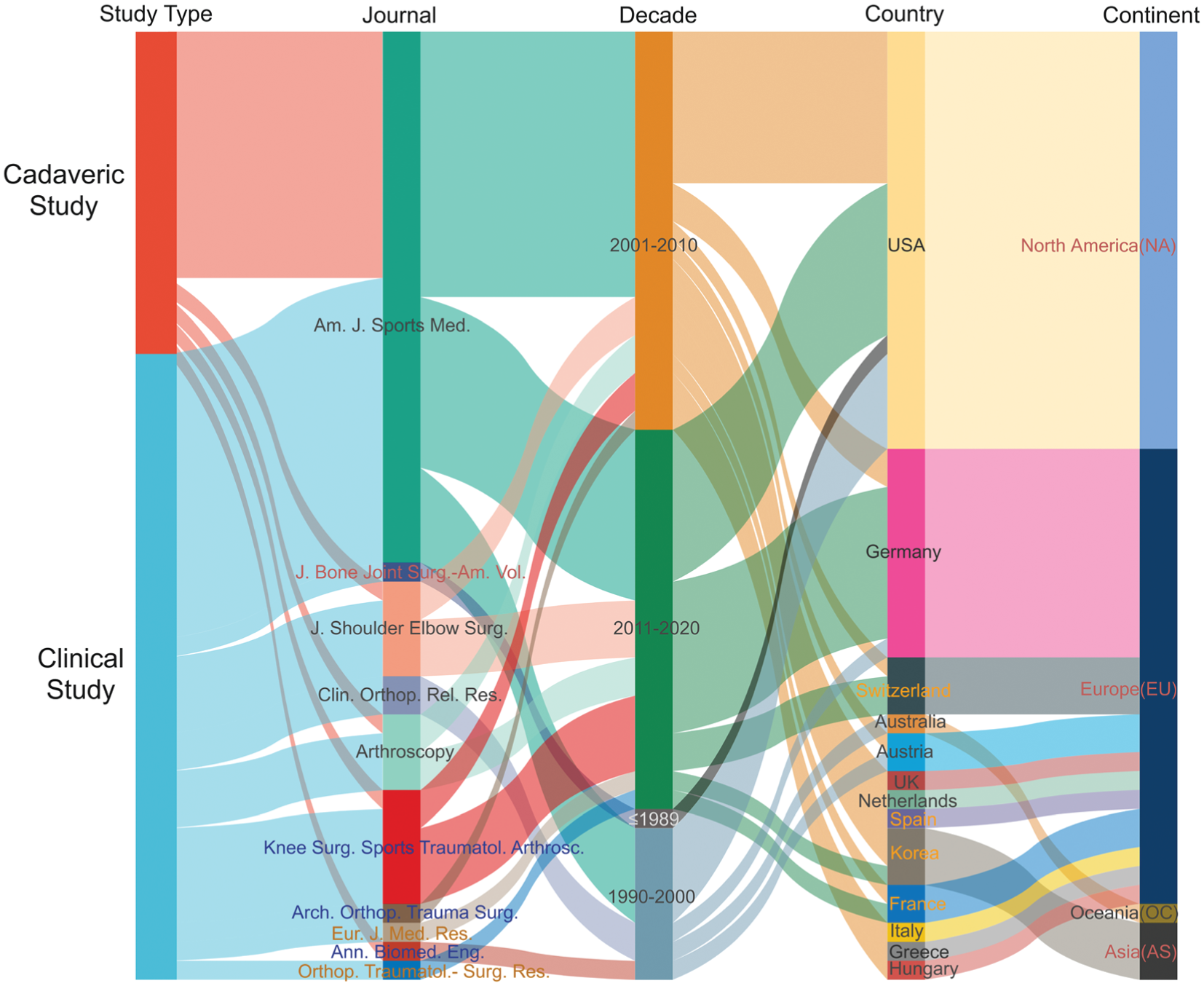
The Sankey diagram visualizes the distribution of the 50 most-cited articles in ACJ reconstruction research. Am J Sports Med, American Journal of Sports Medicine; Ann Biomed Eng, Annals of Biomedical Engineering; Arch Orthop Trauma Surg, Archives of Orthopaedic and Trauma Surgery; Arthroscopy, Arthroscopy: The Journal of Arthroscopic and Related Surgery; Clin Orthop Rel Res, Clinical Orthopaedics and Related Research; Eur J Med Res, European Journal of Medical Research; J Bone Joint Surg Am, Journal of Bone and Joint Surgery American Volume; J Shoulder Elbow Surg, Journal of Shoulder and Elbow Surgery; Knee Surg Sports Traumatol Arthrosc, Knee Surgery Sports Traumatology Arthroscopy; Orthop Traumatol Surg Res, Orthopaedics & Traumatology: Surgery & Research.
Discussion
The most important finding of this study was that the 50 most-cited articles on ACJ reconstruction exhibited overall moderate methodological quality. Citation count was statistically positively correlated with MINORS scores, indicating that studies with better reporting quality tended to be cited more. Conversely, a statistically significant negative correlation was found between citation count and LOE, suggesting that higher levels of evidence (ie, lower LOE numbers) were generally associated with greater academic impact. Although several studies with lower evidence levels (LOE = 4) achieved high citation counts, these appeared to be exceptions rather than the norm. No significant correlations were observed for the MCMS, the MQCSRE, or the BOBQAT. These findings suggest that, while certain methodological criteria such as those captured by the MINORS score may enhance a study's visibility, not all quality assessment tools show a consistent relationship with citation frequency.
The most frequently cited studies 17 predominantly focused on biomechanical optimization and clinical innovation in ACJ reconstruction. The most cited article, a cadaveric biomechanical analysis, demonstrated the superiority of anatomical CC reconstruction over the modified Weaver-Dunn procedure, emphasizing the importance of methodological precision and experimental rigor. Similarly, a highly cited prospective clinical study, 28 using the double TightRope technique for high-grade ACJ separations, highlighted how innovative surgical methods and structured clinical design can attract academic attention. Another frequently cited anatomical investigation 24 identified key landmarks for tunnel placement, illustrating how clinically relevant anatomical guidance contributes to surgical accuracy and enduring impact. 7 Collectively, these examples suggest that both technical innovation and methodological robustness—whether biomechanical or clinical—are key drivers of citation impact. However, high citation counts should not be interpreted solely as indicators of methodological superiority, as visibility, novelty, or widespread clinical applicability may also influence academic recognition.
The predominance of retrospective and case-control designs among the 50 most cited studies reflects the inherent challenges of conducting prospective trials in surgical research. Despite their inherent bias, these designs remain valuable for exploring hypotheses and guiding future prospective studies. The overall low LOE (mainly Level 3-4) highlights the need for more robust clinical investigations. Interestingly, biomechanical cadaveric studies, despite their experimental nature, often achieved high methodological scores on the BOBQAT scale, suggesting that rigorous experimental design may, to some extent, compensate for the absence of higher-level clinical evidence. Future research should therefore prioritize prospective randomized controlled studies to enhance the quality of evidence and refine treatment strategies for ACJ reconstruction. 35
Temporal analysis indicates a dynamic evolution of research focus in ACJ reconstruction: earlier decades were dominated by foundational biomechanical and technical studies, whereas more recent years emphasize advanced surgical techniques and clinical outcomes. Because citation counts naturally accumulate over time and may also be influenced by visibility, controversy, or academic popularity rather than methodological rigor, citation-based analyses tend to favor older publications and may underrepresent recent high-quality research. Accordingly, citation counts in this study should be interpreted as indicators of academic influence rather than direct measures of methodological quality.
This growing research interest can be attributed to several clinical and scientific factors, particularly the increasing demand to reduce complication and failure rates reported in earlier studies on ACJ reconstruction.3,10 This trend is also driven by the need to optimize patient outcomes through a better understanding of surgical techniques and patient-specific factors.26,32 Additionally, recent studies emphasize the importance of imaging and detailed patient-reported outcomes in evaluating treatment success. 30
The majority of highly cited studies on ACJ reconstruction were published in leading sports medicine journals, particularly those with broad international readership, such as Am J Sports Med. Most originated from institutions in the United States and Germany, reflecting the strong research infrastructure and long-standing academic focus on shoulder surgery in these regions. This concentration in high-impact journals and specific geographic areas underscores the influence of established research networks and resources on academic visibility. Encouraging greater international collaboration and multicenter studies could help diversify contributions and advance global understanding in this field.
The limitations of this study require careful consideration. Although 4 validated scoring systems were applied to ensure comprehensive assessment, they evaluate different dimensions of quality. Specifically, the BOBQAT reflects biomechanical rigor rather than clinical applicability, whereas the MCMS, the MINORS, and the MQCSRE assess clinical methodological strength. These differences were considered when interpreting the results. While these scoring systems are effective for evaluating methodological rigor in both clinical and biomechanical studies, they do not necessarily capture factors that determine clinical relevance or patient outcomes. Moreover, differences in study design and publication characteristics may influence the observed relationships between methodological scores and citation counts, as citation frequency can be affected by factors such as visibility, reputation, or author networks. Finally, older studies have had more time to accumulate citations, which may affect citation density analysis. Furthermore, the observed correlations between citation counts and quality scores should be interpreted cautiously. Given the limited sample size and the methodological diversity among the included studies, these correlations likely indicate a weak association rather than a direct relationship between citation frequency and study quality.
Conclusion
Study quality scores showed only a weak correlation with citation counts among the 50 most cited studies on ACJ reconstruction. This finding indicates that citation frequency may reflect academic visibility more than methodological rigor. Overall study quality was moderate, highlighting the ongoing need for well-designed, higher-level studies to strengthen the evidence base in this field. Nevertheless, these findings provide a concise overview of the most influential studies, serving as a valuable reference for future research and clinical practice in ACJ reconstruction.
Footnotes
Final revision submitted October 11, 2025; accepted November 6, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.S. has received consulting fees from Arthrex GmbH, KLS Martin Group, and medi GmbH & Co. B.S. has received consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.