
Abstract
Background:
Persistent instability and altered scapular mechanics after acromioclavicular joint (ACJ) reconstruction may stem from inadequate replication of native coracoclavicular (CC) ligament function. However, in vivo data on postoperative CC ligament behavior during dynamic shoulder motion remain lacking.
Purpose:
To assess in vivo functional distance and timing characteristics of the conoid and trapezoid ligaments during active shoulder elevation after ACJ reconstruction, using dynamic stereo x-ray (DSX) imaging and patient-specific 3-dimensional (3D) models.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Twelve participants (10 men and 2 women, mean age 39 ± 10 years, mean body mass 92 ± 17 kg) who had sustained an acute unilateral ACJ disruption (Rockwood classification of 3-5) and undergone anatomic ACJ reconstruction were recruited within 1 to 3 years after surgery. Participants underwent 3D computed tomography (CT) and DSX imaging to capture abduction, scaption, and flexion movements. Patient-specific bone models with digitized CC insertion points were then aligned within each frame of the biplanar radiograph images. From this, the peak functional distance, time at peak, and displacement were measured and compared with the uninjured limb.
Results:
Compared with uninjured limbs, the reconstructed limb demonstrated increased conoid and trapezoid peak distances of 23% and 17% between insertion points, respectively, across abduction, flexion, and scaption. Additionally, the conoid and trapezoid reached these peak distances at later stages of the movement cycle, and experienced increased displacement by 2.7 and 1.8 mm, respectively, in the reconstructed limb.
Conclusion:
This investigation established the methodological feasibility of using DSX combined with patient-specific CT models to quantify in vivo ligament behavior during functional shoulder motion. It further identified significant asymmetries in the functional distance between conoid and trapezoid ligament insertion points when comparing reconstructed and uninjured limbs across multiple shoulder elevation movements.
Keywords
Acromioclavicular joint (ACJ) injuries are among the most common shoulder pathologies, accounting for up to 10% of all shoulder injuries and occurring with particularly high frequency in young athletes engaged in contact sports.8,11,13,20,30 These injuries can compromise the coordinated motion between the clavicle, scapula, and humerus, leading to long-term dysfunction, altered scapular mechanics, and increased risk of secondary pathologies, such as impingement, rotator cuff degeneration, and glenohumeral instability.16,22,24,31,34 While many cases are managed nonoperatively, higher-grade disruptions (Rockwood 3b-5) are often treated with surgical reconstruction to restore joint stability and shoulder function.7,12,25 This underscores the need for improved biomechanical understanding of the ACJ and its supporting ligamentous structures, to restore physiological joint biomechanics and, in turn, optimize functional outcomes. 26
The management of ACJ injuries is typically guided by the Rockwood classification system.7,12,25 While types 1 and 2 are generally treated nonoperatively, types 4 to 6 are considered surgical due to greater displacement and instability. Management of type 3 injuries remains controversial, with recent literature suggesting that this category may be further subdivided into type 3a (stable) and type 3b (unstable with excessive instability) disruptions. 5 Reconstruction is commonly pursued in patients who demonstrate persistent instability, high functional demands, or failed nonoperative therapy. 42 Despite widespread adoption of surgical approaches, outcomes remain variable—highlighting the need for improved understanding of the biomechanical consequences of reconstruction and the factors influencing long-term joint stability.
Understanding the functional roles and biomechanical properties of the acromioclavicular (AC) and coracoclavicular (CC) ligaments is essential for successful surgical reconstruction after ACJ injuries. Isolated reconstruction of the AC ligament complex fails to address both horizontal and vertical instability, which is primarily resisted by the conoid and trapezoid ligaments.28,10,14,35 Effective reconstruction requires anatomic restoration of both ligament complexes to reestablish joint stability. 36 Achieving this requires a precise understanding of their dynamic behavior under physiologic loading conditions.
Cadaveric studies have provided detailed measurements of the coracoid process and distal clavicle, as well as the attachment sites of the conoid and trapezoid ligaments in relation to surrounding bony landmarks.14,17,32,33,35 More recently, in vivo studies using sequential magnetic resonance imaging (MRI) and computed tomography (CT) have investigated the kinematics of the conoid and trapezoid ligaments at rest and during different supported positions of the shoulder abduction.18,19,37 However, these methods are limited in that they do not capture the dynamic behavior of the CC ligaments during active movement. As a result, a gap remains in our understanding of how these ligaments function during muscle-driven activities of the shoulder.
Dynamic stereo X-ray (DSX) imaging, combined with patient-specific 3-dimensional (3D) bone models, may address this gap, enabling high-precision measurement of joint motion under real-life, muscle-driven conditions. Unlike supine CT and MRI studies, this approach allows evaluation in the upright position, providing a more physiologically relevant assessment of ACJ loading from arm weight and dynamic movement. Importantly, DSX does not suffer from the traditional inaccuracies of skin-mounted markers due to movement artifacts from soft tissue and has been shown to achieve validated accuracy of 0.5 mm and 0.5° for the glenohumeral joint. 6 It has further been used effectively to study rotator cuff pathology,3,4 reverse shoulder arthroplasty, 39 and ACJ kinematics. 42 However, to our knowledge, DSX has not yet been applied to evaluate the mechanical constraints of the CC structure in vivo after ACJ reconstruction. Such an evaluation necessitates a direct comparison of the native ligament insertion sites between the reconstructed and uninjured sides to assess the extent to which the structure's kinematics have been restored. This is important, given that the conoid and trapezoid have distinct yet complementary mechanical roles; thus, accurately recreating the native force vectors of both ligaments is essential to restoring normal CC biomechanics.
This study aimed to quantify the displacement and timing of the CC ligament insertion sites across multiple planes of humeral elevation—abduction, scaption, and flexion. We hypothesized that the native CC ligament insertion sites in surgically reconstructed shoulders would exhibit increased displacement and altered temporal profiles compared with the uninjured limb, while showing no difference in static supine measurements. Such knowledge may establish the methodological feasibility of using DSX to explore joint reduction and mechanical dysfunction after surgery. This could offer new insights into optimal graft placement and surgical techniques to reestablish normative CC biomechanics and improve long-term stability.
Methods
Participants
This study was approved by the institutional review board at the University of Texas Health Science Center, Houston (HSC-MS-20-0585). Twelve participants (10 men and 2 women; mean age, 39 ± 10 years; mean body mass, 92 ± 17 kg; mean height, 179 ± 10 cm) were enrolled in this cross-sectional study after providing written informed consent. Given the exploratory nature of this study and the lack of previous data to estimate effect sizes for the outcomes of interest, a formal sample size calculation was not performed. All participants had previously undergone surgical treatment within 17 ± 9 days of a unilateral ACJ disruption classified as Rockwood 3 to 5, 1 to 3 years before enrollment. ACJ reconstructions were performed using anatomic fixation techniques as described below. A total of 8 participants underwent reconstruction of the CC ligaments alone—3 via open surgery and 5 arthroscopically assisted techniques—while 4 participants underwent concomitant reconstruction of the CC ligaments and AC joint capsule (1 open and 3 arthroscopically assisted). Table 1 further details the treatment delay, number of clavicle and coracoid tunnels drilled, graft types used, and the fixation methods employed.
Surgical Procedures a
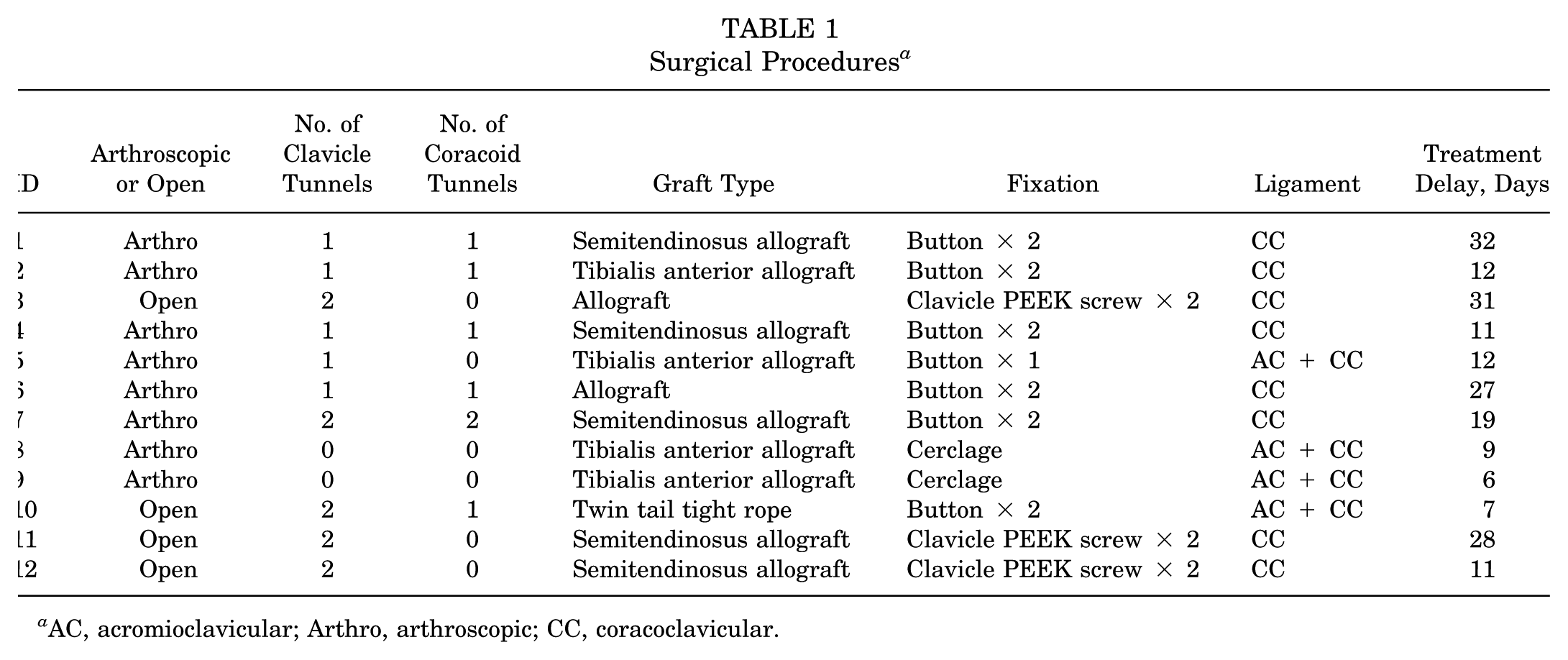
AC, acromioclavicular; Arthro, arthroscopic; CC, coracoclavicular.
Recruitment procedures and results from clinical surveys have been previously described in an earlier publication. 42 To reduce selection bias, participants were screened from 4 separate clinics within the University of Texas Health Science Center to improve generalizability, with clear and consistent inclusion/exclusion criteria employed. Briefly, participants were initially assessed by reviewing clinical notes to determine eligibility and were subsequently contacted to screen for inclusion and exclusion criteria. Participants were included if they had no history of shoulder pathology or bilateral injuries and were free of neuromuscular conditions that could impair shoulder function. They were excluded if lactating/pregnant, had a body mass index >35 kg/m2, suffered from upper-extremity fractures, scapulothoracic dislocations, rotator cuff tears, r-injury to the ACJ, or clinically diagnosed cervical spine pathologies. Additionally, patients did not report any significant issues with their operated shoulder either verbally or within their surveys.
CT Examination
High-resolution CT scans of both shoulders were acquired for each participant (voxel size, 0.6 × 0.6 × 0.6 mm; Cannon, Aquilion One 640, Dual-Energy CT Scanner). Scans encompassed the clavicle and the superior aspect of the shoulder complex, extending distally to include the distal humeral condyles. Patient-specific models of clavicle, scapula, and humerus were generated by segmenting the CT scans in Mimics, Version 25 (Materialise). These models were used to define anatomic coordinate systems, digitize the insertion sites of the conoid and trapezoid ligaments, and enable the registration of each bone with corresponding DSX data. The coordinate system definition followed the recommendations of the International Society of Biomechanics (ISB). 41
CC Insertion Points
Ligament origins and insertions were modeled as single points based on literature-derived coordinates33,35 to standardize measurement and reflect clinically relevant fixation sites used in surgical reconstruction. Clavicular insertion points were identified according to Rios et al, 33 while coracoid landmarks were identified based on Salzmann et al. 35 These studies reported detailed cadaveric measurements that were used to estimate the mean locations of the ligament footprint centers, based on defined distances from well-established anatomic landmarks on the clavicle 33 and coracoid process. 35 Although absolute variations in the origins of CC ligaments were observed, the authors concluded that the ratios of these mean origins relative to the corresponding bony dimensions remain consistent. The specific magnitudes of these ratios and the associated measurement errors are detailed in the following paragraphs.
Clavicular Insertions. A cylinder was fitted to the clavicle; thus, its longitudinal axis encompassed both medial and lateral ends of this bone. The clavicle length was defined as the distance along this axis. The conoid and trapezoid insertion points were estimated as 24% and 17% of the clavicle length, with an expected error of 2.9 and 4.4 mm, respectively, measured from the lateral tip of the clavicle 33 (Figure 1). A second cylinder containing the lateral tip of the clavicle, oriented toward the conoid tubercle, was used to isolate the landmark for accurate identification. Visual inspection confirmed that the insertion points fell within the anatomic boundaries of the conoid tubercle and trapezoid line.

Establishing the location of the conoid (blue) and trapezoid (red) insertion points on patient-specific bone models, using calculations from Rios et al 33 for the clavicle process, and Salzmann et al 35 for the coracoid process. These approximated landmarks were digitized. Clavicular insertions were identified based on proportional distances from the lateral aspect of the clavicle, as described by Rios et al. The insertion sites of the coracoid were derived from anatomic landmark ratios along the longitudinal and transverse axes of the coracoid, as defined by Salzmann et al. These digitized landmarks were utilized in the segmented computed tomography (CT) models to facilitate patient-specific tracking of ligament distances during dynamic motion. Length of clavicle (LC), length of scapular coracoid process (Ls), and width of scapular coracoid process relative to length ratios (Ws).
Coracoid Insertions. For the coracoid process, a cylinder was fit that encompassed the following landmarks: the base, tip, precipice, and medial/lateral coracoidal borders. The coracoid length was then defined as the length of the cylinder's axis, with the longitudinal axis aligned to the base and tip. The location of the conoid and trapezoid along the coracoid's length was calculated as 85% and 72% of the coracoid length, with an expected error of 3.7 and 3.3 mm, respectively. 35 A plane orthogonal to the coracoid's longitudinal axis was then created at each of these respective points, allowing the width of the coracoid to be determined. The locations of the conoid and trapezoid were then calculated as 85% and 65% of the coracoidal width from the medial and lateral borders, with expected errors of 2 and 3 mm, respectively 35 (Figure 1).
All measurements were performed using 3-Matic software (Version 25; Materialize).
Dynamic Stereo X-ray
The DSX system used 2 X-ray sources to acquire high-speed X-ray videos from 2 calibrated, nonoverlapping view angles. Each shoulder was analyzed individually, with the process repeated for both shoulders. The patient was seated upright, with the shoulder remaining within the field of view, at a source-to-detector distance of approximately 180 cm and an interbeam angle of 30° to 45°. Shoulder kinematics were recorded at a frequency of 20 Hz, utilizing a maximum voltage of 85 kVp, a current of 125 mA, and a pulse width of 2 ms. The radiation parameters were adjusted to attain optimal contrast in both tissue and bone while concurrently minimizing exposure. Patients were required to complete a minimum of 3 practice trials for each movement before measurement to ensure consistency and familiarity. Subsequently, 3 repetitions of each movement were recorded: (1) abduction in the coronal plane, (2) 30° of abduction to the coronal plane (scaption), and (3) forward flexion. Movements were performed unweighted and began with the arms positioned to the sides, with patients maintaining an upright posture characterized by a straight back, extended elbows, and palms oriented anteriorly throughout the movement. A trial was completed once the arm had reached a maximum elevation and returned to the starting position. A wooden guidepost and metronome (set at 70 beats per minute) were used to standardize the movement plane and pacing, with the arm required to reach maximum elevation on the first beat and return to the starting position on the successive beat.
Postprocessing
After data acquisition, patient-specific 3D bone models of the clavicle, scapula, and humerus, along with their respective anatomic coordinate systems, were registered to DSX images using DSX-Suite (HAS Motion Inc). Briefly, the bone models’ contours were aligned frame-by-frame to DSX images using previously validated model-based tracking techniques21,42 (Supplementary Video 1). Segmental kinematics were then computed in Visual3D (HAS Motion Inc) using ISB-recommended Euler rotation sequences 41 about the superior/inferior, medial/lateral, and anterior/posterior joint axes (Figure 2). The location of the conoid and trapezoid insertion points on the clavicle and scapula was mapped onto the clavicle and scapula bone models. The functional ligament distance was then estimated by calculating the Euclidean distance between the respective insertion points. These calculations were performed on static measurements taken during the CT scan while the patient lay supine, as well as on dynamic measurements from each DSX trial with the patient seated upright. For each movement repetition, the timepoint at which the arm reached its lowest and highest points was recorded and subsequently normalized to reflect 0% to 100% of the movement cycle.
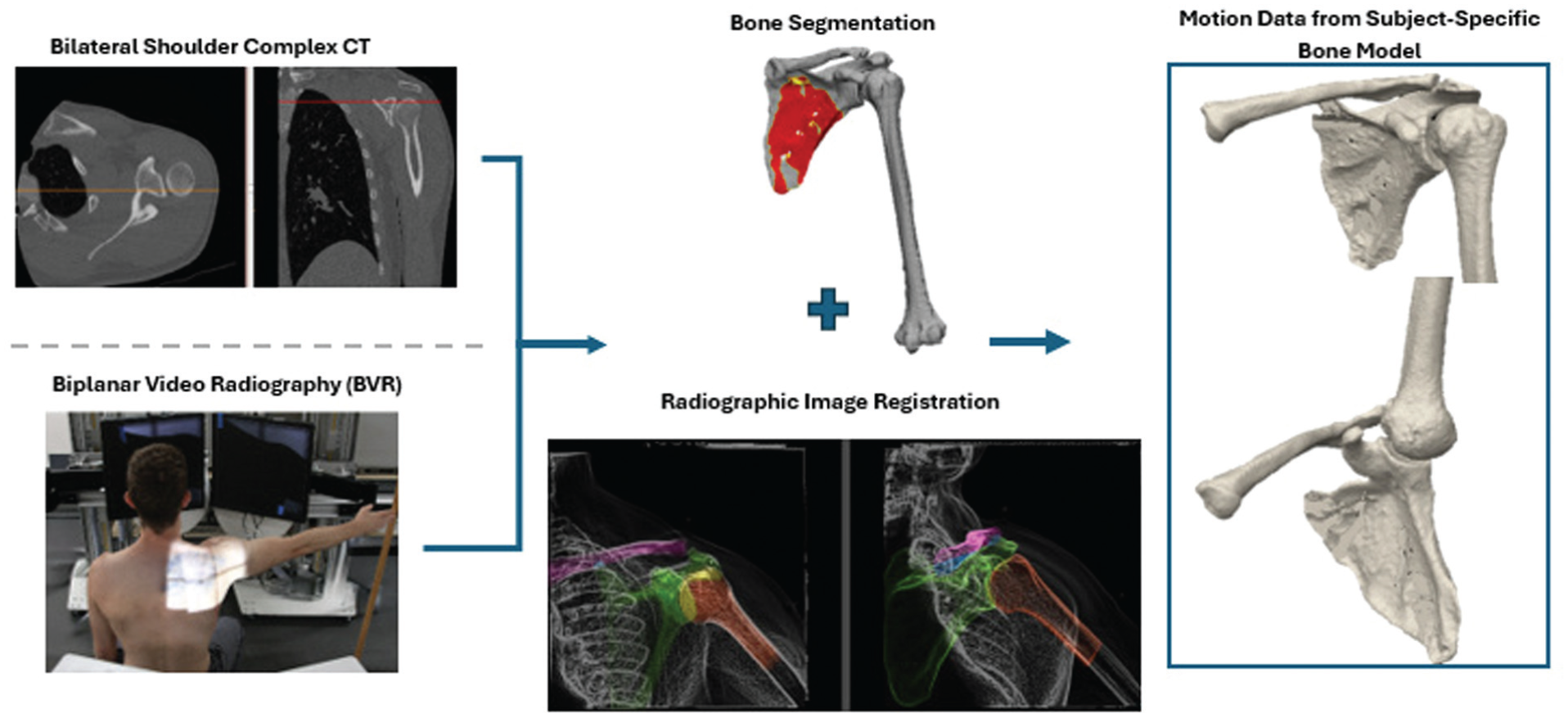
Workflow for generating subject-specific 3D kinematic models from CT and DSX data. High-resolution CT was used to create segmented bone models of the clavicle, scapula, and humerus. These models were then registered to each frame of the biplanar DSX video using model-based tracking, enabling precise estimation of in vivo ACJ motion during active humeral elevation. ACJ, acromioclavicular joint; CT, computed tomography; DSX, dynamic stereo X-ray; 3D, 3-dimensional.
Outcome Measures
To summarize, the following outcome measures were calculated and analyzed as continuous variables, with no categorization performed:
Peak Functional Distance. The maximum distance between ligament insertion points was observed during both the upward and downward phases of each movement.
Time of Peak Functional Distance. The time point at which the peak functional distance occurs, expressed as a percentage of the movement cycle, during both the upward and downward phases. This parameter was used to identify potential temporal asymmetries across movements.
Mean Distance. The mean distance between ligament insertion points throughout the upward and downward phases of each movement.
Displacement. The difference between the maximum and minimum distances between insertion points within each upward and downward phase. This measure approximates the extent of ligament length change during each movement cycle.
Statistical Analysis
A generalized linear mixed model (GLMM) was used to assess the effect of limb (reconstructed/uninjured) and movement types (abduction/flexion/scaption) on peak functional distance, time of peak distance, displacement, and mean length during the upward and downward phases of movements for the conoid and trapezoid ligaments. All outcome measures were analyzed as continuous variables, with no categorization performed. The GLMM was selected to handle repeated-measures data per participant while also modeling trial-level variability. Furthermore, the GLMM can accommodate multiple fixed effects and their interactions, as well as non-Gaussian outcome distributions. Additionally, mean ensemble curves (mean ± standard error) were generated across the full movement cycles for both limb sides. Given the exploratory nature of this study, the use of prespecified and well-defined predictors, the absence of confounding variables, and minimal missing data, no sensitivity analyses were conducted. Furthermore, no analytical adjustments for sampling design or subgroup analysis were necessary. Patients with missing CT scans or suboptimal DSX imaging quality were excluded from the study. Statistical analysis was performed using SPSS Version 29 (SPSS Inc), with significance set at P < .05, with Bonferroni correction applied for multiple comparisons.
Results
The patient recruitment process is outlined in Appendix Figure A1. Of the 82 patients initially screened, 52 met the inclusion criteria. Sixteen patients consented to participate in the study; however, 4 were excluded from the analysis due to either missing their CT scan appointment or suboptimal DSX imaging quality. Descriptive data of the final 12 patients included in the statistical analysis are provided in Appendix Table A1.
CT-based measurements taken while the patient lay in the supine position revealed no significant differences in the functional distances of the conoid and trapezoid between the reconstructed and uninjured sides (Table 2).
Peak Functional Distance, Time at Peak Functional Distance (% of Movement Cycle), Mean Distance, and Displacement of the Conoid and Trapezoid Ligaments During Humeral Elevation (n = 12) a

Data are presented as mean ± SD. Results are reported for the ipsilateral (reconstructed) and contralateral (uninjured) limbs across abduction, flexion, and scaption. CT, computed tomography.
Indicates statistically significant differences between limbs (P < .05).
The functional distance between conoid and trapezoid insertion points, throughout the entire movement phase, including ascension and descension, is presented in Figure 3 for abduction, flexion, and scaption. Both ligaments experience peaks in the upward concentric phase of the movement, as well as the downward eccentric phase. However, the timings of these peaks are observed to occur at different stages for the reconstructed and uninjured limbs throughout all movements. Furthermore, a demonstrable offset between reconstructed and uninjured limbs can be observed throughout the entire motion, with the conoid showing larger differences than the trapezoid.

Ensemble curves showing mean functional length of the (A) conoid and (B) trapezoid ligaments throughout the full cycle of humeral elevation (upward and downward phases) during abduction, flexion, and scaption. Blue lines represent the ipsilateral (reconstructed) limb and red lines the contralateral (uninjured) limb. Shaded areas indicate ± standard error. The reconstructed ligaments consistently demonstrated larger length and altered timing of peak displacement compared with the uninjured side, particularly during abduction and scaption.
During the ascending phase of movements, the conoid ligament exhibited a larger peak distance between insertion points in the reconstructed limb than the uninjured limb across abduction (δ = 0.74), flexion (δ = 0.97), and scaption (δ = 0.66) (P < .001) (Figure 4). The reconstructed conoid reached its peak length in abduction later in the movement cycle (δ = 0.52; P = .021). Furthermore, the reconstructed conoid experienced larger displacement and mean distance across abduction (δ = 0.56; P = .01), flexion (δ = 0.82; P = .001), and scaption (δ = 0.89; P < .001) than the uninjured limb (Table 1).
During ascent, the reconstructed trapezoid ligament demonstrated significantly larger peak insertion distance compared with the uninjured limb during flexion (δ = 0.53; P < .001) and scaption (δ = 0.35; P = .01) (Figure 4). During abduction and scaption, the reconstructed ligament reached peak length later in the movement cycle (δ = 0.61 and 0.56; P < .001 for both). Additionally, displacement between trapezoid insertion points was significantly greater in the reconstructed limb during abduction (δ = 0.56; P = .013), flexion (δ = 0.65; P < .001), and scaption (δ = 0.41; P < .001). The reconstructed trapezoid also exhibited increased mean length during flexion (δ = 0.32; P = .045) and scaption (δ = 0.32; P = .036) (Table 2).

Peak functional distance and timing of peak elongation for conoid and trapezoid ligaments during shoulder elevation movements. Panels show results for the (A) conoid during arm ascent, (B) conoid during descent, (C) trapezoid during ascent, and (D) trapezoid during descent. Bars represent mean values for the ipsilateral (reconstructed) and contralateral (uninjured) limbs across abduction, flexion, and scaption. Asterisks (*) indicate statistically significant differences between limbs (P < .05).
During the descending phase of movements, the reconstructed conoid similarly exhibited a larger peak distance between insertion points compared with the uninjured limb across abduction (δ = 0.68; P = .002), flexion (δ = 0.91; P < .001), and scaption (δ = 0.74; P < .001). Notably, these peaks occurred earlier in the movement cycle during abduction (δ = 0.57; P < .001). The reconstructed conoid also demonstrated significantly greater mean ligament length during abduction (δ = 0.58; P = .009), flexion (δ = 0.76; P = 0.001), and scaption (δ = 0.53; P = .006), as well as greater displacement during flexion (δ = 0.74; P = .002) and scaption (δ = 0.96; P < .001) (Table 2).
Similarly, the trapezoid ligament showed significantly greater peak insertion distance in the reconstructed limb during flexion (δ = 0.52; P < .001) and scaption (δ = 0.39; P = .004) (Figure 4), and reached its peak length earlier in the cycle during abduction and flexion (δ = 0.44 and 0.68; P < .001 for both). The reconstructed trapezoid also demonstrated increased displacement during abduction (δ = 0.49; P < .001) and flexion (δ = 0.62; P = .001), and greater mean length during flexion (δ = 0.45; P = .006) and scaption (δ = 0.34; P = .006) (Table 2).
Discussion
This exploratory study leveraged DSX imaging combined with patient-specific 3D bone models to investigate the functional distance between CC insertion points during various shoulder elevation movements in patients with surgically reconstructed AC joints. The reconstructed limb demonstrated greater peak functional distances, increased displacement of the native ligament insertion sites, and altered timing of peak displacement across abduction, flexion, and scaption. These findings varied by movement type, suggesting that CC ligament mechanics are not uniformly restored across functional shoulder motions. These preliminary results raise important questions about whether current reconstruction approaches adequately replicate native CC ligament function. The observed deviations in conoid and trapezoid displacement patterns may contribute to persistent alterations in scapulothoracic rhythm, potentially predisposing some patients to scapular dyskinesis or secondary impingement syndromes. These findings support the need for further investigation into how different surgical techniques and nonoperative treatment of ACJ disruptions alter CC mechanics and internal contact mechanics, and how these may influence long-term joint function.
An important observation of the present study was the absence of significant differences in peak functional distance in the resting supine position. In contrast, the reconstructed limb exhibited greater functional distance and displacement during both the upward and downward phases of shoulder elevation movements. Additionally, larger distances were observed at the onset of all movements (see Figure 3), likely reflecting ligament loading as the shoulder transitions from a supine position to an upright position. This suggests that static imaging may be insufficient for assessing the restoration of normal CC kinematics during dynamic, muscle-driven activities. As such, previous studies employing sequential MRI and CT to investigate CC kinematics with the shoulder in supported positions18,19,37 can be limited in capturing the dynamic behavior of the CC ligaments during active movement in both the upward concentric and downward eccentric phases.
The conoid insertion points demonstrated a consistent pattern of progressive lengthening during arm elevation, while the trapezoid demonstrated progressive shortening (see Figure 3) (0% to 50% of the movement cycle). These observations of the uninjured limb align with previous findings by Izadpanah et al, 18 who reported that the conoid lengthens by 3 mm during abduction in healthy volunteers using MRI, and with similar elongations when moving from supine to seated postures. 18 Similarly, Seo et al 37 demonstrated that the conoid undergoes a comparable magnitude of elongation between 60° and 180° of abduction, along with a reduction in the trapezoid length in healthy individuals. These converging data suggest that the conoid ligament lengthens during arm elevation, while the trapezoid shortens. This behavior may be attributed to the clavicle's internal rotation relative to the scapula, which itself upwardly rotates and tilts during elevation.23,42
Both the conoid and trapezoid insertion points exhibited larger mean and peak functional distances in the reconstructed limb, accompanied by greater displacements compared with the uninjured side, with flexion and scaption showing the greatest differences (Table 1). Given that the conoid underwent nearly twice the displacement in the reconstructed limb, reaching displacements of up to 6.3 mm compared with 3.4 mm in the uninjured limb, this may indicate clavicular instability in the superior-inferior direction. This is notable because the conoid ligament serves as a critical stabilizer, limiting excessive clavicle elevation during abduction. 29 These findings may be clinically important, due to excessive clavicular elevation being associated with poor cosmetic appearance and shoulder pain. 23 Additionally, increased functional distance and displacement between trapezoid insertion points in the reconstructed limb may indicate posterior instability of the clavicle. Horizontal stabilization appears to be clinically important, as excessive posterior subluxation of the clavicle has been shown to negatively affect clinical outcomes, 9 with persistent anterior-posterior instability being associated with chronic pain. 1 Patients who successfully restore horizontal stability have also been reported to achieve better clinical outcome scores. 9
Larger discrepancies between reconstructed and uninjured limbs were observed at the conoid insertion points compared with those of the trapezoid. This is shown in Figure 3 and supported by the mean lengths reported for abduction, flexion, and scaption in Table 1. Because each shoulder elevation movement primarily involves motion along the inferior-superior axis rather than the anterior-posterior axis, this may explain the greater deficits observed in the conoid ligament. The trapezoid ligament primarily resists shear forces and prevents posterior translation of the clavicle, while also serving as a secondary constraint against superior displacement.14,29 These findings underscore the distinct yet complementary biomechanical roles of the conoid and trapezoid ligaments. Surgical treatment is typically guided by the degree and direction of clavicular translation, which reflects the injury state of the AC and CC ligaments. 40 Techniques that reconstruct the CC ligaments as a single unit may prevent superior translation but often fail to control anteroposterior instability. 2 While it can be challenging to recreate the true initial anatomy, reproducing the native force vectors of both the conoid and trapezoid ligaments may better restore biomechanical function and improve AC joint stability. 27 This may involve positioning the clavicular tunnel for the graft more posteriorly to help reduce posterior clavicular displacement and improve anterior-posterior stability. In addition, optimal placement of the coracoid tunnel is important—it is typically located on the horizontal portion of the coracoid, but not on its posterior aspect. Regardless of the precise graft placement, the methods used in the present study may help determine the extent to which surgical reconstruction restores the mechanical constraints of the CC structure.
With respect to the temporal parameters, our study demonstrated that both the conoid and trapezoid ligaments reached their peak distance between insertion sites later during the ascent and earlier during the descent phase of arm movement. Notably, these peak distances occurred when the humeral angle slightly exceeded 90°, coinciding with the period of maximal upward scapular rotation, 38 particularly during abduction. In addition, previous studies have shown that scapular upward rotation is more pronounced during abduction >60° than other movement planes.15,23 The altered timing of peak CC ligament distances observed in our study may reflect increased posterior and superior translation of the clavicle on the reconstructed side, relative to the uninjured limb, which could suggest compromised ACJ stability. Moreover, such temporal deviations may disrupt normal scapulothoracic rhythm, potentially predisposing individuals to scapular dyskinesis or secondary impingement syndromes.
Limitations
As with many in vivo biomechanical investigations, certain methodological constraints were unavoidable in the present preliminary study. The locations of ligament insertion points were estimated using landmark-based ratios derived from mean attachment sites reported in previous literature, rather than direct measurement from MRI. While this approach may reduce spatial precision to some extent, it is consistent with previously validated methodologies and reflects practical constraints associated with CT- and DSX-based imaging workflows, where MRI acquisition for each subject was not feasible due to logistical and resource limitations. The ligament's repair and continuity were not assessed; however, patients with failed repairs were excluded from the study. Moreover, ligament origins and insertions were modeled as single points rather than anatomic footprints. Although this simplification does not capture the full complexity of the conoid's conical shape or the trapezoid's broad, V-shaped footprint, 33 it allows for consistent, reproducible measurement of functional ligament distances across a range of movements. Moreover, the use of single-point representations for the CC ligaments has been shown to be reproducible and able to be obtained intraoperatively to perform graft fixation through ≥1 discrete single-point bone tunnels in the clavicle and coracoid.33,35
Another limitation arises from the retrospective nature of the study, which precluded control over surgical technique and graft positioning. Notably, the number of coracoid and clavicular tunnels was not consistent, which is precisely why we sought to investigate the constraints of the native ligament insertion sites between reconstructed and uninjured limbs, to determine how the constraints of the CC structure were restored, rather than direct measurement of graft elongation. However, this variability also mirrors clinical reality, enhancing the generalizability of the findings. The following methods can be applied using precisely defined graft placement sites derived from MRI or CT to investigate graft elongation. A final limitation to consider was that the present study did not include any clinical tests or results; however, patients reported no significant issues with their operated shoulder, as confirmed by clinical survey results. Although the sample size was modest, this study was conducted as a preliminary, exploratory effort to assess the feasibility of using CT and DSX imaging for in vivo analysis of CC kinematics. The study's primary aim was to establish a methodological framework and generate pilot data to support the estimation of effect sizes and power calculations for future, larger-scale prospective studies.
Notably, despite these limitations, this study, to our knowledge, represents the first attempt to characterize the in vivo behavior of the CC ligament during active, multiplanar shoulder motion. These findings provide valuable biomechanical insights and lay the groundwork for sample size calculations to design larger-scale investigations aimed at determining how altered CC mechanics influence long-term joint function. Future research should investigate how different surgical approaches influence these mechanics—including graft type and fixation method, single-bundle versus double-bundle CC reconstruction, anatomic versus nonanatomic tunnel placement, the number of tunnels drilled, and employing tunnel-free approaches. Moreover, these methods may be used to investigate how these changes influence joint reduction, subluxation, and internal contact mechanics in both surgical and nonoperatively treated patients. This knowledge could provide valuable insights into optimizing long-term joint health.
Conclusion
This investigation established the methodological feasibility of using DSX combined with patient-specific CT models to quantify in vivo ligament behavior during functional shoulder motion. It further identified significant asymmetries in the functional distance and displacement between conoid and trapezoid ligament insertion points when comparing reconstructed and uninjured limbs across multiple shoulder elevation movements.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251408739 – Supplemental material for Preliminary In Vivo Evaluation of Coracoclavicular Ligament Mechanics During Shoulder Elevation After Acromioclavicular Joint Reconstruction
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251408739 for Preliminary In Vivo Evaluation of Coracoclavicular Ligament Mechanics During Shoulder Elevation After Acromioclavicular Joint Reconstruction by Jason Konrath, Sydney Wheaton, Alonso Figueroa, James Gregory and Payam Zandiyeh in The Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors acknowledge Connor Smith and Jonathon Ross for assistance with BVR tracking and Erica Lee for research coordination.
Final revision submitted October 15, 2025; accepted November 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health under Award Number R01AR083471. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. J.G. has received consulting fees from Stryker, Arthrex, and Wright Medical Technology; nonconsulting fees from Arthrex and Wright Medical Technology; education payments from MedInc of Texas; and hospitality payments from Zimmer Biomet Holdings. AOSSM checks author disclosures against the Open Payments Database (OPD).
AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The University of Texas Health Science Center at Houston (reference no. HSC-MS-20-0585).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.