
Abstract
Background:
Heterotopic ossification (HO) frequently occurs after treatments for acute acromioclavicular (AC) joint dislocations, and is often considered a complication.
Hypothesis/Purpose:
This study aimed to evaluate and compare HO severity and configuration after single-suture button (SSB) and double-suture button (DSB) stabilization, and nonoperative treatment. It was hypothesized that the extent of HO after Rockwood (RW) type V injuries is associated with increased vertical stability, without substantially impairing clinical results.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients with acute RW type V dislocations treated with SSB (group 1), DSB (group 2), or nonoperatively (group 3) were analyzed with a 2-year follow-up. The exclusion criteria were previous shoulder surgery or concomitant fractures. HO was evaluated on anteroposterior stress radiographs in the conoid ligament area (CLA) and trapezoid ligament area (TLA), graded by severity and configuration. Radiographic parameters (coracoclavicular difference, RW classification, DPT, and osteoarthritis) and clinical outcomes (Constant Score, Subjective Shoulder Value, Taft score (TF), and Acromioclavicular Joint Instability score were assessed. Group differences were tested using the Kruskal-Wallis test, and associations between HO severity and outcomes were assessed using linear regression.
Results:
A total of 85 patients were included (group 1, n = 36; group 2, n = 28; and group 3, n = 21), with a mean age of 39.3 ± 11 and a mean follow-up of 44 ± 21.5 months. HO occurred in 71.3% of cases (CLA) and 58.7% of cases (TLA), with no group differences (P = .390). Severity was predominantly mild across all groups, and the configuration was mostly clavicular. Severity showed no group difference (CLA, P = .703; TLA, P = .132). Configuration differed for the TLA (P = .042), but not for the CLA (P = .178). Severity of HO in the CLA correlated with higher TF scores (B = 0.902; P = .003), whereas TLA severity correlated negatively (B = −0.823; P = .034).
Conclusion:
When present, HO was mostly mild and clavicular, without relevant radiographic or clinical effects. Severity in the CLA correlated with a higher TF, whereas severity in the TLA correlated negatively. Given that the other radiographic and clinical parameters are unaffected, the term complication should be used with caution.
Dislocation of the acromioclavicular (AC) joint is one of the most frequent injuries to the adult shoulder, mostly affecting young, active men. 7 The initial assessment is typically based on physical examination and radiographic imaging, and the extent of injury is classified according to the Rockwood (RW) classification system, 20 ranging from type I to type VI. Nonoperative treatment is recommended for low-grade dislocations (RW type I-II), and surgical therapy is widely recommended for high-grade dislocations (RW type IV-VI), whereas the treatment of RW type III and V dislocations remains controversial.2,4,15 Arthroscopic-assisted procedures and suture-button fixation systems are well-established methods for stabilizing the AC joint, with favorable outcomes compared with open procedures and hardware devices that require secondary removal.21,26 Common complications after various treatment procedures for AC joint dislocations include persistent pain, vertical and horizontal recurrent instability, enlargement of the initial drill holes (tunnel widening), clavicular or coracoidal fractures, or AC joint osteoarthritis.3,5,21,25,26 Additionally, heterotopic ossification (HO) between the clavicle and coracoid is often reported in the literature and is commonly regarded as a complication. However, its specific effect—whether adverse or even beneficial—on this specific type of trauma has yet to be clarified.12,21,22,26 HO is an ectopic formation of lamellar bone in muscle and soft tissues. It is the result of local tissue being affected by oxygen tension, pH (hydrogen ion concentration), available micronutrients, and mechanical impulses, which transform progenitor cells into osteogenic precursor cells.19,27 HO is frequently seen after traumatic injuries, burns, neurological injuries, severe traumatic amputations, and major orthopaedic interventions, and is recognized as a major complication in these cases.19,27,28 HO is most commonly observed after acetabular fractures and hip arthroplasty. 16 Early symptoms include pain, inflammation, and tenderness; over time, it may limit joint mobility, and in the final stage, lead to permanent loss of motion or joint ankylosis.16,27 Computed tomography images and plain radiographs are the primary methods of diagnosing an HO.19,28 The primary objective of this study was to evaluate and compare the severity and configuration of HO after arthroscopic-assisted single-suture button (SSB) or double-suture button (DSB) stabilization, or nonoperative treatment, after acute AC joint dislocation. We hypothesized that the extent of HO after RW V AC joint injuries is associated with increased vertical stability, without substantially impairing clinical results.
Methods
Ethics Approval
This study was approved by the responsible local institutional review board
Patient Selection
A total of 85 patients with acute RW type V dislocation, treated with either an SSB (group 1) or a DSB (group 2) procedure, or nonoperative treatment (group 3), were included in this retrospective cohort study. A RW type V injury was classified based on >100% displacement to the contralateral side, as measured on panoramic anteroposterior (a.p.) stress radiographs, along with horizontal displacement on Alexander view radiographs.1,20 All patients were selected from a local shoulder surgery clinic database and treated between 2010 and 2021. The patients were treated by 5 different certified shoulder surgeons and examined (clinical and radiological assessments) by 2 independent observers (J.P., L.E.) who were not involved in the surgical procedures. The inclusion criteria for this study were as follows: (1) acute presentation, <3 weeks after reported trauma; (2) high-grade AC joint dislocation according to an RW type V injury; and (3) a minimum clinical and radiographic follow-up of 2 years. 20 The exclusion criteria were previous surgery to the same shoulder and concomitant fractures.
Treatment Procedures
The treatment approach, whether surgical or nonsurgical, was determined on an individual basis in accordance with the patient's preferences. Until 2018, the DSB procedure was utilized for surgical interventions, and since then, the SSB procedure has been established as the clinical standard. The arthroscopic-assisted, image-intensifier-controlled SSB and DSB procedures used for the surgical treatment of groups 1 and 2 were performed as described in previous reports, both of which included a diagnostic arthroscopy at the beginning.17,21 For the SSB technique, a 3.0-mm transclavicular-transcoracoidal tunnel was created between the anatomic insertions of the coracoclavicular (CC) ligaments. 17 Through a nitinol suture passing wire, a low-profile TightRope device (Arthrex) was shuttled and secured with a DogBone button (Arthrex) beneath the coracoid. 17 The DSB technique was performed similarly, with the first tunnel placed at the superomedial insertion of the conoid ligament and a second tunnel approximately 2 cm lateral, allowing bicortical fixation with 2 DogBone buttons (Arthrex). 21 In both techniques, a horizontal transclavicular-transacromial cerclage augmentation was added. 17 After both surgical procedures, the same rehabilitation protocol was applied. For the first 6 weeks, an abduction immobilizer was prescribed. During the first 3 weeks, patients were limited to a passive range of motion with flexion and abduction exercises up to 45°; up to the sixth week, with 90°. Free passive and early active range of motion was performed starting in week 7, followed by strengthening exercises beginning in week 10. All nonoperatively treated patients were recommended to wear a sling for 1 to 2 weeks, with permission to perform free range of motion and weightbearing, adapted to the patient's pain.
Radiographic Evaluation
On panoramic a.p. stress radiographs with a 10 kg load on each side, the CC distance was measured on both the affected and unaffected sides preoperatively and reported as the CC difference (in mm). The percentage difference between the sides was indicated as the RW classification in the preoperative measurements and as the RW reclassification in the final follow-up measurement. Preoperatively, all RW type V dislocations display a percentage difference of at minimum 100%, according to the classification. 20 By taking the same value at the final follow-up time point, it was intended to analyze the vertical repositioning loss. Instead of using percentages, the differences were indicated as ratios. Horizontal stability was assessed on Alexander view radiographs, as previously described, by evaluating the dynamic posterior translation (DPT), classified as none, partial, or complete instability.1,14 The occurrence of HO between the clavicle and coracoid was assessed on a.p. radiographs and subdivided into the conoid ligament area (CLA) and trapezoid ligament area (TLA). Severity was analyzed as described before and classified, in reference to the Brooker classification of the hip, as none (not visible; Figure 1), mild (isolated osseous islands; Figure 2), moderate (incomplete osseous bridging; Figure 3), and severe (complete osseous bridging; Figure 4).21,6 Configuration of HO was characterized as originating from clavicular, coracoidal, CC, or as isolated islands. Additionally, the presence of AC joint osteoarthritis was evaluated.

No ossification and a vertically stable acromioclavicular joint after a single suture button stabilization procedure.
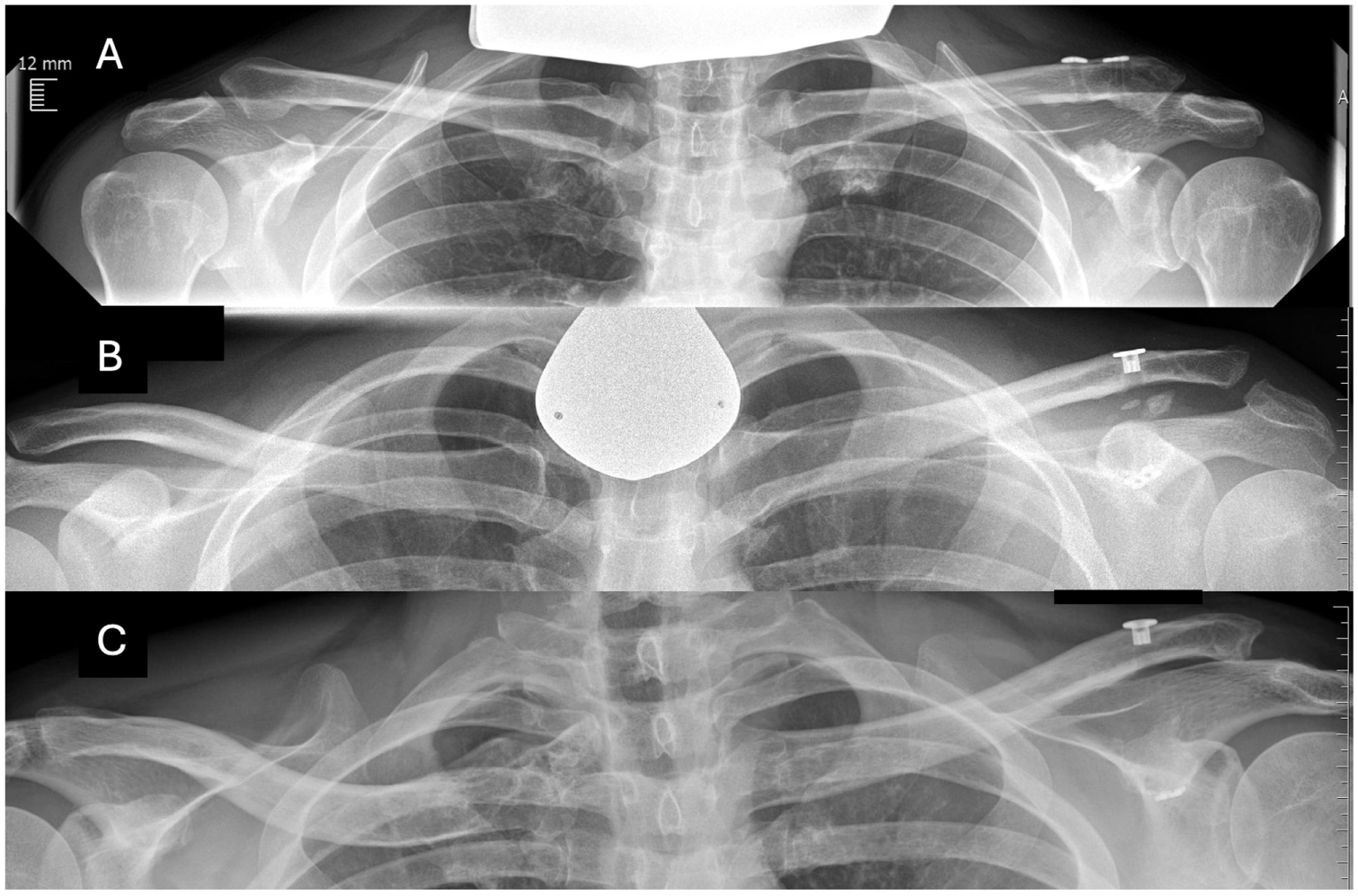
(A) Mild ossification (isolated osseous islands) on the left side in the conoid ligament area, with a clavicular configuration after a double-suture button stabilization procedure. (B) Mild ossification on the left side in the conoid and trapezoid ligament areas, between the clavicle and coracoid (coracoclavicular) after a single-suture button stabilization procedure. (C) Mild ossification on the left side, mainly in the trapezoid ligament area, with a coracoidal configuration.
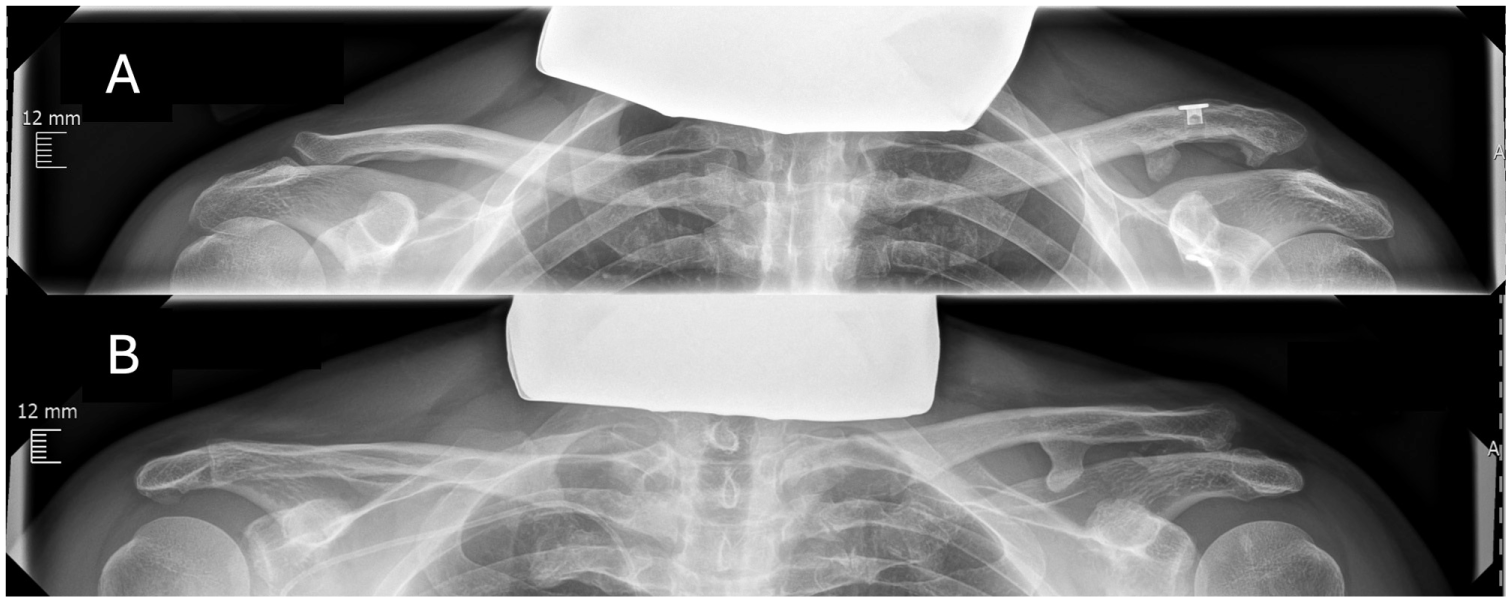
(A) Moderate ossification (incomplete osseous bridging) on the left side in the conoid and trapezoid ligament area, with a clavicular configuration after a single-suture button stabilization procedure. (B) Moderate ossification on the left side in the area of the conoid ligament and mild ossification (isolated osseous islands) in the trapezoid ligament area, both with a clavicular configuration, after nonoperative treatment.
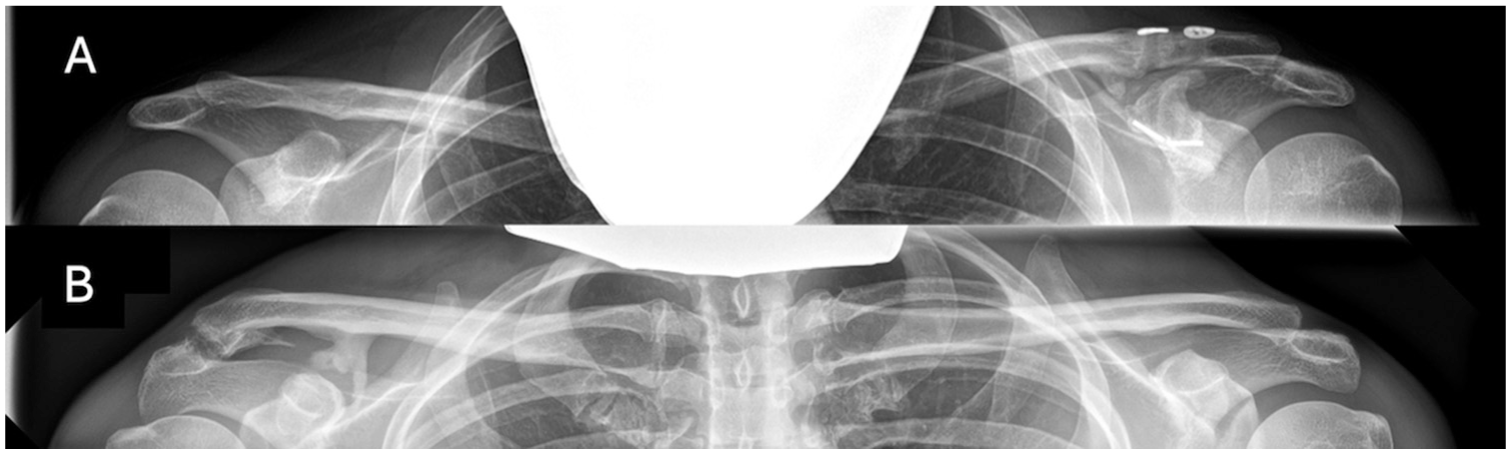
(A) Severe ossification (complete bridging) on the left side after a double-suture button stabilization procedure. (B) Severe ossification on the right side after nonoperative treatment.
Clinical Evaluation
At the final follow-up, all patients underwent a complete physical examination of both shoulders and completed a questionnaire to assess clinical outcomes. Clinical outcome scores included the Constant Score (CS), Taft (TF) score, Acromioclavicular Joint Instability (ACJI) score, and Subjective Shoulder Value (SSV).8,14,23
Statistical Analysis
Statistical analysis of the data was performed using IBM SPSS Statistics Version 20.0.1.0 (IBM Corp). The significance level was set at P < .05, and the confidence interval was set at 95%. The Kolmogorov-Smirnov test was used to assess normality. Results were reported as mean ± standard deviation or as number (percentage). Comparison between groups was conducted using the Kruskal-Wallis test. The chi-square test was used to compare categorical variables. The paired t test was used to analyze differences between preoperative and final follow-up within the same group. A multivariate linear regression was performed with severity of HO in CLA and TLA as exploratory variables and radiographic outcomes (CC difference, RW reclassification, DPT, and AC joint osteoarthritis) and clinical outcomes (CS, TF score, ACJI score, and SSV) as dependent variables at the final follow-up. We controlled for age, sex, preoperative CC difference, and preoperative RW classification in the model.
Results
Baseline Characteristics
A total of 85 patients (group1, n = 36; group 2, n = 28; group 3, n = 21) were included, of which the majority was men (97.6%; P = .24). The mean age of the entire study population was 39.3 ± 11 years and did not differ between groups (P = .20). In 92.4% of the patients the mechanism of injury was a direct trauma, with bicycle accidents accounting for 52.2%. The mean follow-up period until the final clinical and radiographic examination was 44 ± 21.5 months with a significant difference between groups (P = .01). The mean time from trauma to surgery differed between the groups with group 1 averaging 8.2 ± 4.4 days and group 2 averaging 5.8 ± 2.9 days (P = .01). A concomitant glenohumeral injury was observed during diagnostic arthroscopy in 25% of cases in group 1 and 28% of cases in group 2 (P = .42). The preoperative CC difference was 11.8 ± 2.8 mm in group 1, 14.2 ± 3.1 mm in group 2, and 11 ± 3 mm in group 3 (P = .003). The preoperative RW classification was 1.5 ± 0.5 in group 1, 1.9 ± 1.2 in group 2, and 1.5 ± 0.8 in group 3 (P = .79). Detailed baseline patient characteristics are presented in Table 1.
Baseline Patient Characteristics a
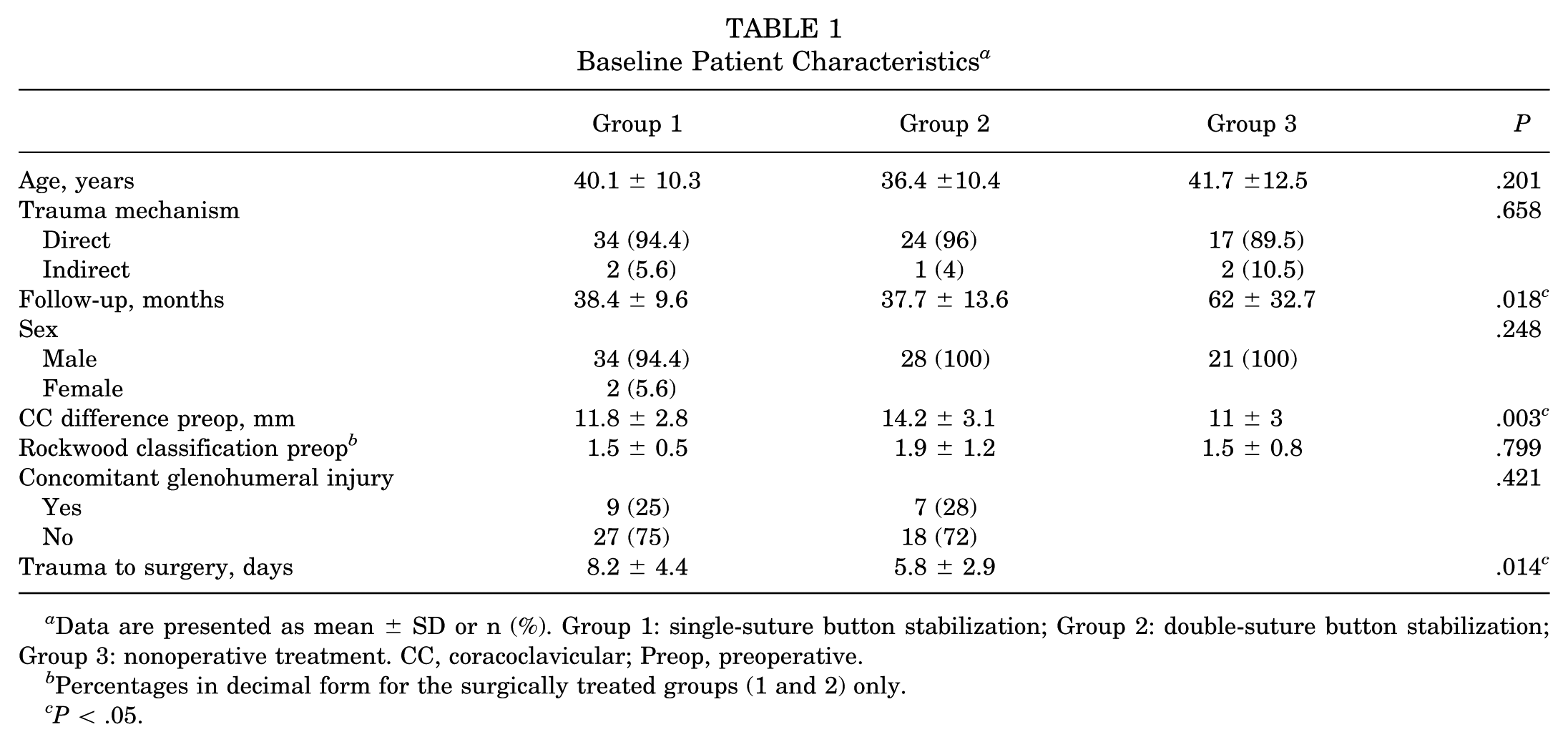
Data are presented as mean ± SD or n (%). Group 1: single-suture button stabilization; Group 2: double-suture button stabilization; Group 3: nonoperative treatment. CC, coracoclavicular; Preop, preoperative.
Percentages in decimal form for the surgically treated groups (1 and 2) only.
P < .05.
Radiographic Analysis
The final CC difference (group 1, 1.78 ± 2.8 mm; group 2, 2.7 ± 2.3 mm; group 3, 6.07 ± 3.7 mm) was significantly different between group 1 and group 3 (P < .001) and between group 2 and group 3 (P < .001). Similarly, the RW reclassification showed significant differences between group 1 and group 3 (P < .001) and between group 2 and group 3 (P < .001). However, neither the CC difference (P = .115) nor the RW reclassification (P = .198) showed significant differences between the surgical groups. CC difference and RW reclassification significantly decreased in all 3 groups from preoperative to the final follow-up timepoint at 44 ± 21.5 months (group 1, P < .001; group 2, P < .001; group 3, P < .001). Overall, DPT (P = .036) differed significantly between groups, with a significant difference between group 1 and 3 (P = .028). No significant difference was observed between group 1 and group 2 (P = .573) nor between group 2 and group 3 (P = .094). No significant differences were observed between the groups regarding osteoarthritis of the AC joint (P = .580). HO in general occurred in 31 patients (83.8%), 21 patients (75%), and 24 patients (88.9%), respectively, with no significant group difference (P = .390). Detailed results are listed in Table 2.
Comparison of Radiographic Results a

Data presented as mean ± SD or n (%). Group 1: single-suture button stabilization; Group 2: double-suture button stabilization; Group 3: nonoperative treatment. AC, acromioclavicular; CC, coracoclavicular; DPT, dynamic posterior translation.
Percentages in decimal form.
P < .001.
Severity And Configuration of HO
Overall, HO was observed in 71.3% of cases in the CLA and in 58.7% of cases in the TLA. It was predominantly mild and most frequently originated from the clavicle. Detailed results and the percentage distribution of severity and configuration are presented in Table 3. The severity of HO showed no difference between groups, neither for the CLA (P = .703) nor for the TLA (P = .132). The configuration of HO did not differ between groups for the CLA (P = .178) but for the TLA (P = .042), where clavicular origin was more common in group 3.
Detailed Findings on the Severity and Configuration of Heterotopic Ossification Between Clavicle and Coracoid a

Data are presented as n (%). Group 1: single-suture button stabilization; Group 2: double-suture button stabilization; Group 3: nonoperative treatment. CLA, conoid ligament area; TLA, trapezoid ligament area.
P < .05.
Clinical Outcomes
After a mean follow-up of 44 ± 21.5 months, the mean overall scores were 10 for the TF score, 87.3 for the SSV, 80.4 for the ACJI score, and 89.1 for the CS. There were no differences in TF (P = .129) and SSV (P = .109) scores across the 3 groups, whereas CS (P = .004) and ACJI (P = .018) scores showed significant differences. The CS score was higher in the nonoperatively treated patients, whereas the ACJI score was higher in the DSB group. Detailed results are listed in Table 4.
Comparison of Clinical Outcomes a

Data are presented as mean ± SD. Group 1: single-suture button stabilization; Group 2: double-suture button stabilization; Group 3: nonoperative treatment. ACJI, acromioclavicular joint injury; CS, Constant Score; SSV, Subjective Shoulder Value; TF, Taft score.
P < .05; c P < .01.
Multivariate Regression Analysis
Severity of HO did not have a statistically significant effect on CC difference, RW reclassification, AC joint osteoarthritis, or the results of CS, ACJI score, and SSV after a mean follow-up of 44 ± 21.5 months. The severity of HO in the CLA and TLA significantly affected TF score results (CLA, B = 0.902; P = .003; TLA, B = −0.823; P = .034). Detailed results are presented in Table 5.
Effect of Severity in the Conoid and TLA on CC Difference and RW Reclassification, AC Joint Osteoarthritis, DPT, CS, TS, ACJI, and SSV a
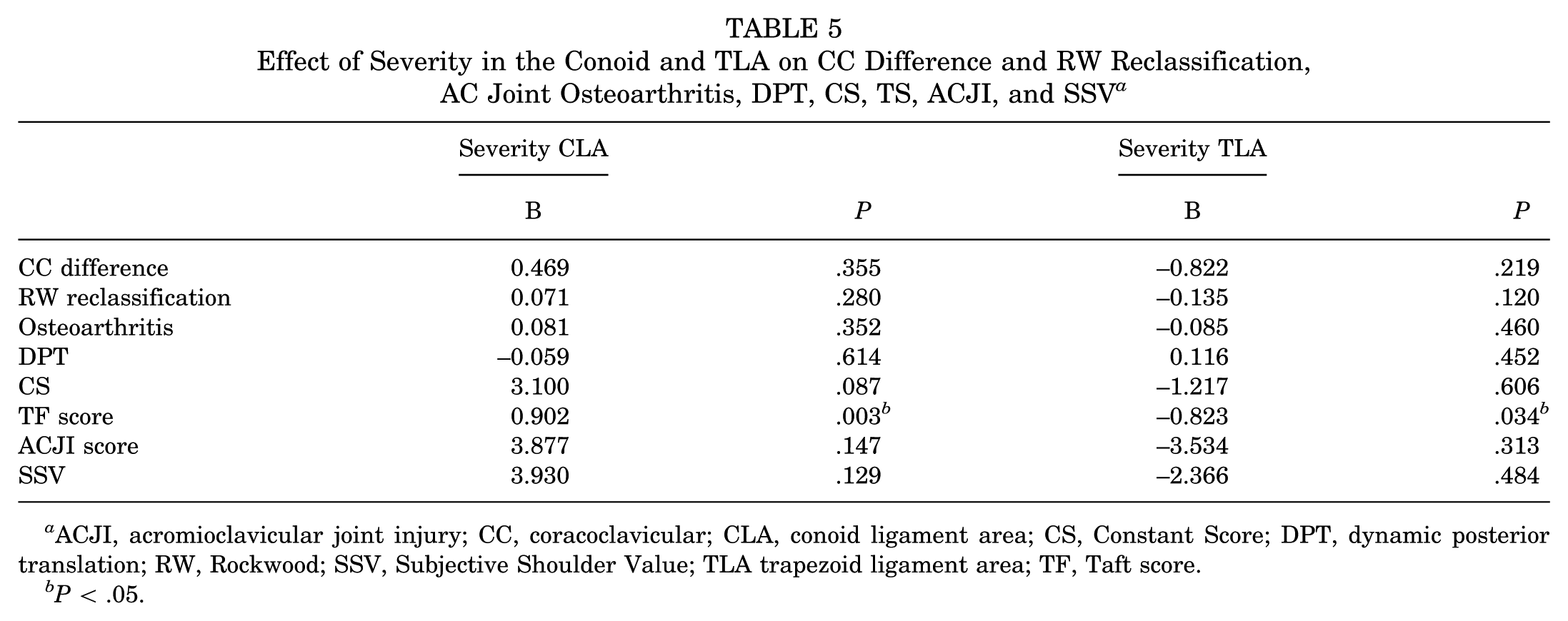
ACJI, acromioclavicular joint injury; CC, coracoclavicular; CLA, conoid ligament area; CS, Constant Score; DPT, dynamic posterior translation; RW, Rockwood; SSV, Subjective Shoulder Value; TLA trapezoid ligament area; TF, Taft score.
P < .05.
Discussion
The primary objective of this study was to assess and compare the severity and configuration of HO after arthroscopic-assisted SSB or DSB stabilization and nonoperative treatment. Additionally, an exploratory objective was to investigate a potential association between HO severity and both radiographic and clinical outcomes. The main findings revealed that the severity of HO after acute AC joint dislocation does not differ between arthroscopic-assisted, SSB, or DSB procedures and nonoperative treatment, and, if present, it is predominantly mild. The severity only affects the TF score results. The configuration of HO was heterogeneous but predominantly clavicular, with no group differences in the CLA, while clavicular origin occurred more frequently in group 3. The other clinical scores, horizontal stability, and AC joint osteoarthritis were not affected by HO. Given the result that HO does not positively or negatively influence clinical outcomes, the term complication when referring to HO after AC joint dislocation should therefore be used with caution. Unlike HO in the hip or elbow, which can severely restrict movement and significantly affect a patient's quality of life, its effect in this context may be less pronounced.16,27 The concept of HO as a complication was most likely adapted for outcome analysis of the AC joint as well, as it has been mentioned as a complication in numerous publications.12,26 The cause of HO is complex, and it remains unclear whether HO occurs after trauma, initiated by various local factors and unknown systemic factors, or is triggered by the release of bone marrow during surgical drilling.19,27 It is possible that the pathomechanism is induced by postoperative bone marrow leakage and subsequent inadequate differentiation of mesenchymal cells and fibroblasts into bone-forming cells based on local factors such as soft tissue edema, local hypoxia, and other as yet unknown systemic factors.13,19,27 According to this scenario, it might be expected that patients treated with the DSB technique and thus with a total of 4 transcoracoidal drillings would show increased ossification, as more bone marrow leaks in proportion than with just 2 drillings. It should therefore be most limited among nonoperatively treated patients without manipulative drilling. However, our results demonstrated no difference in severity between the 3 groups, which argues against the bone marrow leakage theory. Moreover, HO was observed in group 3, in which patients experienced only soft-tissue injury without bone penetration from surgery, further supporting the need to consider alternative pathophysiological mechanisms.
Although risk factors such as male sex or hypertrophic osteoarthritis are often cited, our study found no association between HO and osteoarthritis for AC joint injuries. 27 Additionally, the overall sample size was too small to draw any definitive conclusions regarding the influence of sex. 27 Scheibel et al 21 reported HO in 67.9% of patients and found that high-grade ossifications (partial or complete bridging) were associated with significantly smaller CC distances; however, even severe ossifications did not lead to restrictions in range of motion. 21 Motta et al 18 observed an overall HO rate of 65% and demonstrated that all patients with increased ossification had a stable AC joint without any motion restrictions. As the severity and configuration of HO showed no effect on the CS and ACJI scores, both of which include an explicit query about range of motion, we can also infer that HO has only minimal effects on range of motion.8,14 Ertogrul et al 10 reported ossifications in 37.3% of patients, while the CC distance was also found to be reduced in patients with ossifications compared with those without, and the clinical outcome scores of patients with HO were even better.
Results from the multiple linear regression analysis showed no significant association between HO severity and vertical stability. CLA severity showed a significant effect, indicating that higher severity is associated with higher TF scores. In contrast, TLA severity has a significant negative association with TF score. This difference may be attributed to the different biomechanical functions of these ligaments in stabilizing and providing mobility to the shoulder. Increased ossification of the trapezoid ligament may reduce flexibility and thus the functionality of the shoulder joint. Conversely, increased ossification of the conoid ligament might lead to improved stability, particularly in the vertical plane, which may have functional benefits resulting in improved outcomes.9,11 In this cohort, the presence of HO did not require any further surgical intervention despite severe HO in up to 12.9% of patients. There is an ongoing debate about the necessity of surgical intervention for RW type III and V dislocations. McKee et al 15 demonstrated that after at least 2 years, the results of surgical and nonoperative treatment are equal. Similarly, the results of our study, which included only RW type V dislocations, did not show worse clinical outcomes for patients who received nonoperative treatment, and the CC difference was significantly reduced in all 3 treatment groups after 2 years. When comparing the postoperative CC difference, RW reclassification, and DPT, there was an expected significant difference between nonoperatively treated patients and those treated operatively, consistent with the current literature.5,15,24 Our results also show no difference in TF score and ACJI score, and SSV between surgical and nonoperative therapy. The CS was even improved in favor of the nonoperative therapy group, suggesting that this procedure might be suitable treatment option. Boström et al 5 showed that patients treated surgically exhibited inferior function at the first follow-up examination, as measured by the CS, SSV, and Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) scores, and pain scores at rest and during movement, indicating a slower recovery. Because the CS assesses the dimensions of work, leisure activities, and sleep areas that are typically severely affected during recovery, the higher CS scores in the nonsurgically treated cohort could be attributed to this condition. A prospective multicenter randomized controlled trial by Tauber et al 24 found that surgical treatment of RW type III injuries did not yield superior functional outcomes compared with nonoperative treatment. These findings align with our results, which also demonstrate a significant difference in the final radiographic examination, while clinical outcomes were comparable or even better in patients treated nonoperatively.
Limitations
The present study has several limitations that should be considered when interpreting the results. The retrospective design may introduce selection bias. The inter- and intraobserver reliability of the radiological classifications (intraclass correlation coefficients) was not assessed. In addition, the minimum follow-up period was set at only 2 years, averaging 44 ± 21.5 months, although it is not known when the HO process is completed. Moreover, the follow-up period and the preoperative CC difference showed significant differences between groups, potentially resulting in a biased group comparison. Additionally, the relatively small sample size may influence the statistical power of the study, which was not assessed, potentially making it more challenging to detect significant associations between subgroups. The use of nonsteroidal anti-inflammatory drugs (NSAIDs) for the prevention of HO has been well investigated. 16 NSAIDs remain the most commonly used form of prophylaxis, with various agents demonstrating efficacy. 16 However, because of the retrospective design of this study, reliable data on NSAID use could not be obtained and were therefore not included in the analysis. Another limitation is the difficulty in verifying compliance with the prescribed rehabilitation protocol in the nonoperatively treated group, as well as the fact that the postoperative rehabilitation protocol for surgically treated patients was not strictly aligned with that of the nonoperatively treated group. Moreover, because of the retrospective design, it is no longer possible to reconstruct exactly why a conservative approach was chosen or not. The findings should be interpreted with caution, and a larger cohort should be analyzed to improve the reliability and precision of the results.
Conclusion
When present, HO was mostly mild and clavicular, without relevant radiographic or clinical effect. Severity in the CLA correlated with higher TF scores, whereas severity in the TLA correlated negatively. Given that the other radiographic and clinical parameters are unaffected, the term complication should be used with caution.
Footnotes
Final revision submitted October 12, 2025; accepted October 15, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.S. is a consultant for Arthrex Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ethics Committee of Charité– Universitaetsmedizin Berlin (EA4/231/17).