
Abstract
Background:
Although the posterior tibial slope (PTS) has been identified as a key factor influencing anterior cruciate ligament (ACL) graft biomechanics and clinical outcomes, little is known regarding which plateau has the greater effect on mechanics of the ACL-reconstructed knee. There are differences in slopes of the medial and lateral tibial plateaus, but this difference has yet to be biomechanically investigated in an ACL-reconstructed setting.
Purpose:
To investigate the individual effects of medial and lateral PTS differential modifications on ACL graft force, anterior tibial translation (ATT), and internal tibial rotation in a cadaveric model.
Study Design:
Controlled laboratory study.
Methods:
Twelve fresh-frozen human cadaveric knees (mean age, 61.6 years) were tested. Native PTS was measured using computed tomography. ACL reconstruction was performed, followed by individual anterior closing-wedge osteotomies of the medial and lateral compartments to achieve a 0° slope. Each compartment was then adjusted in 5° increments with 3-dimensional printed wedges and secured with an external fixator. Biomechanical testing consisted of a 500-N axial load and a 1-N⋅m axial torque across 8 medial-lateral PTS states: native/native, 5°/10°, 5°/5°, 10°/5°, 10°/10°, 10°/15°, 15°/15°, and 15°/10°. ACL graft force, ATT, and internal tibial rotation at full extension were recorded. Linear mixed modeling was used to evaluate the effect of medial and lateral slopes on the outcome variables.
Results:
The lateral tibial slope contribution had a greater effect on ACL graft force and ATT than the medial tibial slope contribution. Each 1° increase in lateral slope was associated with a 4.9-N (11.1%) increase in graft force and a 0.63-mm (25.2%) increase in ATT (P < .001). Each 1° increase in medial slope was associated with a 1.9-N (4.3%) increase in graft force and a 0.48-mm (19.2%) increase in ATT (P < .001). Internal tibial rotation was not significantly affected by either lateral or medial PTS.
Conclusion:
Although both slopes significantly affected ACL graft force and ATT, lateral PTS had a greater effect on ACL graft force and ATT compared with the medial PTS and may warrant primary consideration for a slope-correcting osteotomy.
Clinical Relevance:
While correction of both medial and lateral slopes is important, the lateral PTS contributes more significantly to ACL graft forces and ATT.
Anterior cruciate ligament (ACL) injuries are prevalent among active individuals and athletes, often necessitating surgical reconstruction of the ACL to restore knee stability and function. Despite advancements in surgical techniques, a significant proportion of patients experience suboptimal outcomes, including graft failure and persistent rotational instability. Recent studies have highlighted the role of the posterior tibial slope (PTS) in influencing ACL graft biomechanics.8,16,17 An increased PTS has been associated with elevated anterior tibial translation (ATT) and elevated forces on the ACL graft, potentially compromising surgical outcomes. 16
Biomechanical analyses have demonstrated that variations in the PTS can significantly affect the forces transmitted through the ACL graft.7,15 Specifically, an increased lateral PTS has been linked to increased ATT and internal rotation (IR), thereby escalating the mechanical demands on the reconstructed ACL. 7 Conversely, reducing the PTS through anterior slope-reducing osteotomies has been proposed as a strategy to mitigate these forces and enhance graft longevity. 15
While the influence of the lateral PTS on ACL graft stress has been extensively studied, the independent and combined effects of medial and lateral PTS alterations remain less understood. A morphological study of 1090 tibiae found that the mean medial PTS is 1.2° higher than the lateral PTS. 19 Current operative techniques for slope-reducing osteotomies do not account for the difference in medial and lateral tibial slopes, instead reducing the slopes by the same degree. This study aimed to investigate the individual effects of medial and lateral PTS modifications on ACL graft force, ATT, and tibial IR using a controlled cadaveric model. We hypothesized that the lateral PTS would have a greater effect on ACL graft force, ATT, and tibial IR compared with the medial PTS.
Methods
Specimen Preparation
Twelve fresh-frozen human cadaveric knees were tested in this study (mean age, 61.6 years; age range, 38-75 years; 8 males, 4 females). Under donor consent, specimens were previously donated to a tissue bank designated for medical research and purchased by the research team for biomechanical research usage. Institutional review board (IRB) approval was not required as studies utilizing decedent cadavers are IRB exempt. All specimens underwent diagnostic arthroscopy before inclusion. Specimens aged 18 to 65 years, with no osteoarthritis, no cancer to bone, no previous surgeries, or other joint pathology were included. Specimens were excluded if they demonstrated grade >2 chondromalacia in the medial or lateral compartments, meniscal deficiency, prior meniscal surgery, ligamentous deficiency, hypoplastic lateral femoral condyle, significant joint line obliquity, or significant varus or valgus malalignment.
Computed Tomography Measurements
Computed tomography (CT) scans were acquired of each specimen, and the native PTSs were measured of the medial and lateral compartments according to a protocol similar to that of Hudek et al 10 (Figure 1). To calculate the medial slope, a sagittal slice of the center of the specimen, oriented from the center of the tibial plateau to the center of the most distal point on the tibial shaft, was captured, and a sagittal CT slice of the medial compartment, in the same orientation as the slice of the tibial shaft and halfway between the medial margin of the tibial plateau and the medial margin of the tibial spine, was captured. These images were spliced to create an image where both the anterior portion of the tibial shaft and the medial tibial plateau could be observed together. The longitudinal axis of the specimen was estimated by creating a line between the most distal point on the anterior tibia as seen on the CT image and the most anterior point on the medial tibial plateau (the longitudinal axis line). A line from the most anterior point of the medial plateau and the most posterior point of the medial plateau was created (medial slope line). The angle between the medial slope line and the longitudinal axis line was defined as the tibial slope. To calculate the lateral slope, a sagittal CT slice of the lateral compartment and a sagittal slice of the center of the specimen were sliced to create an image where both the anterior portion of the tibial shaft and the lateral tibial plateau could be observed together. The longitudinal axis line was overlaid onto this image, and a line from the most anterior point of the lateral plateau and the most posterior point of the lateral plateau was created (lateral slope line). The angle between the lateral slope line and the longitudinal axis line was defined as the tibial slope.
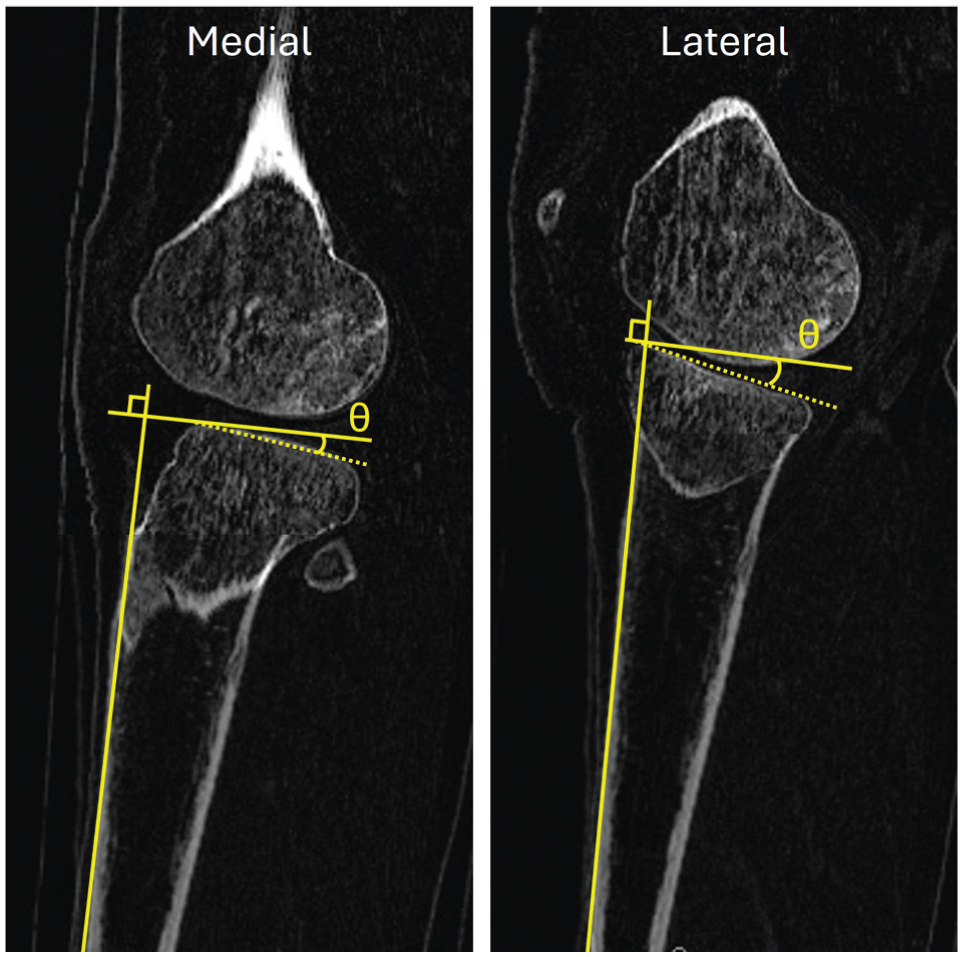
Measurement of the medial posterior tibial slope (left) and lateral posterior tibial slope (right).
ACL Reconstruction
The specimens were thawed 24 hours before dissection with removal of skin and all subcutaneous tissue. All ligamentous structures were left intact with the exception of the native ACL, which was resected. The proximal femur and distal tibia and fibula were then potted in polymethyl methacrylate 25 cm superior to the joint line and 15 cm inferior to the joint line. A bone–patellar tendon–bone (BTB) graft was harvested by first incising 10 mm of the central third of the patellar tendon per the methodology by Wilding et al. 20 Next, 20- to 25-mm × 10-mm patellar and tibial bone blocks were harvested with a micro-oscillating saw cutting to a depth of 10 mm. The BTB bone blocks were contoured with a rongeur to fit into a 10-mm tunnel in the femur. Sutures were placed on each bone block for tunnel navigation. Open ACL reconstruction (ACLR) was then completed. The knee was flexed to 90° and the femoral footprint was marked with a surgical pen. First, a 7-mm anteromedial portal offset guide (Arthrex) was placed in the ACL femoral anatomic footprint. A guide wire was then passed through the guide. A 10-mm acorn reamer was used and drilled to a depth of 25 mm to create the femoral bone tunnel. Next, the tibial tunnel, centered on the tibial footprint, was created utilizing a tibial drill guide (Arthrex). The graft was then passed through the tibial tunnel and into the femoral tunnel. The tibial tunnel traversed the medial plateau osteotomy site, and direct visualization confirmed that the graft did not contact the wedges or adjacent bone. The femoral bone block was fixed with an 8-mm titanium interference screw (Arthrex), and the tibial bone block was left unrestrained to be secured to a force sensor.
Anterior Slope-Reducing Osteotomies
Anterior-wedge slope-reducing osteotomies were performed on the medial and lateral compartments independently following a modified technique described by Zsidai et al 21 using a custom cutting guide (Figure 2A). The medial and lateral compartments were isolated utilizing a sagittal cut just medial and just lateral to the tibial spines, allowing for independent slope reductions of the medial and lateral tibial plateaus. Measurements of the slope-reducing osteotomy cutting guides were based off the medial-lateral slope measurements and printed utilizing a 3-dimensional (3D) printer (X1-Carbon; Bambu Labs). The cutting guides were all designed to have a resultant 0° slope, for normalization of testing states. Two 10-mm Kirshner wires were used to secure the custom-made cutting guide to the anterior tibial edge. Anterior-posterior bone cuts were made utilizing an oscillating saw (Figure 2, B and C). After the osteotomy, custom-made 3D-printed wedges were made to change the slopes of the medial lateral compartment from the native state to each testing state (Figure 2, D and E). All ACLRs and anterior slope-reducing osteotomies were performed by the same 2 fellowship-trained orthopaedic surgeons (E.A.W. and B.B.R.). Radiographs were obtained before and after loading, and measurements of bony contours and external fixator pins were obtained to ensure no micromotion or bone collapse occurred at the osteotomy site. After the desired slope was achieved, external fixators (X-Fix; KLS Martin) were utilized to stabilize the tibial plateau.

(A) Anterior slope-reducing osteotomy with custom cutting guide. (B) Schematic of cutting methodology of native state of slope, θ°. (C) Schematic of slope-reduced state with an external fixator providing construct stability. (D) Representative photograph of testing state where lateral slope is adjusted to 10°. (E) Representative photograph of testing state where lateral slope is adjusted to 15°.
Biomechanical Testing
Figure 3 shows the biomechanical testing setup. Each specimen was tested in 8 states in random order (Table 1).

Specimen mounting and experimental setup.
Testing States

The femur was secured to the actuator of the load frame (Instron ElectroPuls E10000) such that the axis of the end effector was aligned to the femoral potting. With the knee in full extension, the potted tibia was secured to the base of the load frame using a custom fixture on a sliding track that allowed anterior-posterior translation without medial-lateral translation or distal tibial IR. The sliding tibial track was aligned such that tibial translation was along the anterior axis of the knee joint. A time-of-flight laser sensor was placed at the base of the fixture perpendicular to the track to measure ATT (Keyence). Knee joint IR was measured along the axis of the load frame via the testing rig. An S load cell was attached via sutures to the tibial side of the ACLR graft to measure graft force, and the graft was pretensioned to 50 N. Biomechanical testing consisted of a 500-N axial load with a 1-N⋅m IR torque, during which ATT, tibial IR, and ACL graft force were continuously recorded. 17 Coronal alignment was measured for each testing state using a goniometer. To ensure accurate medial-lateral slope changes between states, sagittal radiographic images were acquired for every testing state using a C-arm, and sagittal alignment was measured from each image by a board-certified orthopaedic surgeon (E.A.W.).
Statistical Analysis
The lateral and medial PTSs were assessed for their independent and/or joint effect on ACL graft force, ATT, and tibial IR using linear mixed-effects modeling. 17 Random intercepts were used to allow a different baseline force for each specimen, and to account for the repeated-measures nature of the experimental design. It was hypothesized a priori that the effect of the lateral PTS may depend on the medial PTS and vice versa, so interaction terms were assessed for inclusion in each model using the Bayesian information criterion (BIC). 4 When the BIC was selected for the main-effects model, the interaction term was dropped from the model and effect estimates were interpreted as the effect of changing that specific variable while holding the other factor constant. Comparisons of estimated marginal means were reported, and the Tukey method was used to make pairwise comparisons among the experimental states while controlling the type 1 error rate. 13 P values <.05 were interpreted as statistically significant. Residual diagnostics were performed to confirm model assumptions and model fit. The statistical computing software R Version 4.0.5 (R Foundation for Statistical Computing) was used for all analyses. 12
Results
Comparing the main-effects model to the interaction model showed that any difference seen in ACL graft force, ATT, or tibial IR was not dependent on the interaction between the lateral and medial PTSs. Therefore, the linear main-effects model was used for statistical analyses of the data for both PTSs. The mean native medial tibial slope was 10.6°± 2.3° (range, 6.2°-14.7°). The mean native lateral tibial slope was 9.8°± 2.5° (range, 4.9°-15.8°).
ACL Graft Force
Graphical displays of ACL graft force data can be found in Figure 4. Increased lateral and medial PTSs revealed a linear and statistically significant increase in ACL graft force (P < .001). In full extension, each 1° increase of lateral PTS reduction was significantly associated with an increased ACL graft force of 4.9 N (11.1%). Each 1° increase of medial PTS was significantly associated with an increased ACL graft force of 1.9 N (4.3%).

Box plot of anterior cruciate ligament (ACL) graft forces with individual data points presented per combination of lateral and medial posterior tibial slopes (PTSs) (left). Fitted linear mixed-effects model of ACL graft force as a function of medial PTS (top right) and lateral PTS (bottom right). The mean ACL graft force is labeled with an “x.”
Anterior Tibial Translation
A graphical display of ATT data can be found in Figure 5. Increased lateral and medial PTSs revealed a linear and statistically significant increase in ATT (P < .001). In full extension, each 1° increase of lateral PTS reduction was significantly associated with an increased ATT of 0.63 mm (25.2%). Each 1° increase of medial PTS was significantly associated with an increased ATT of 0.48 mm (19.2%).

Box plot of anterior tibial translation (ATT) with individual data points presented per combination of lateral and medial posterior tibial slopes (PTSs) (left). Fitted linear mixed-effects model of ATT as a function of medial PTS (top right) and lateral PTS (bottom right). The mean ATT is labeled with an “x.”
Internal Rotation
A graphical display of tibial IR data can be found in Figure 6. Increased lateral and medial PTSs had no effect on tibial IR.
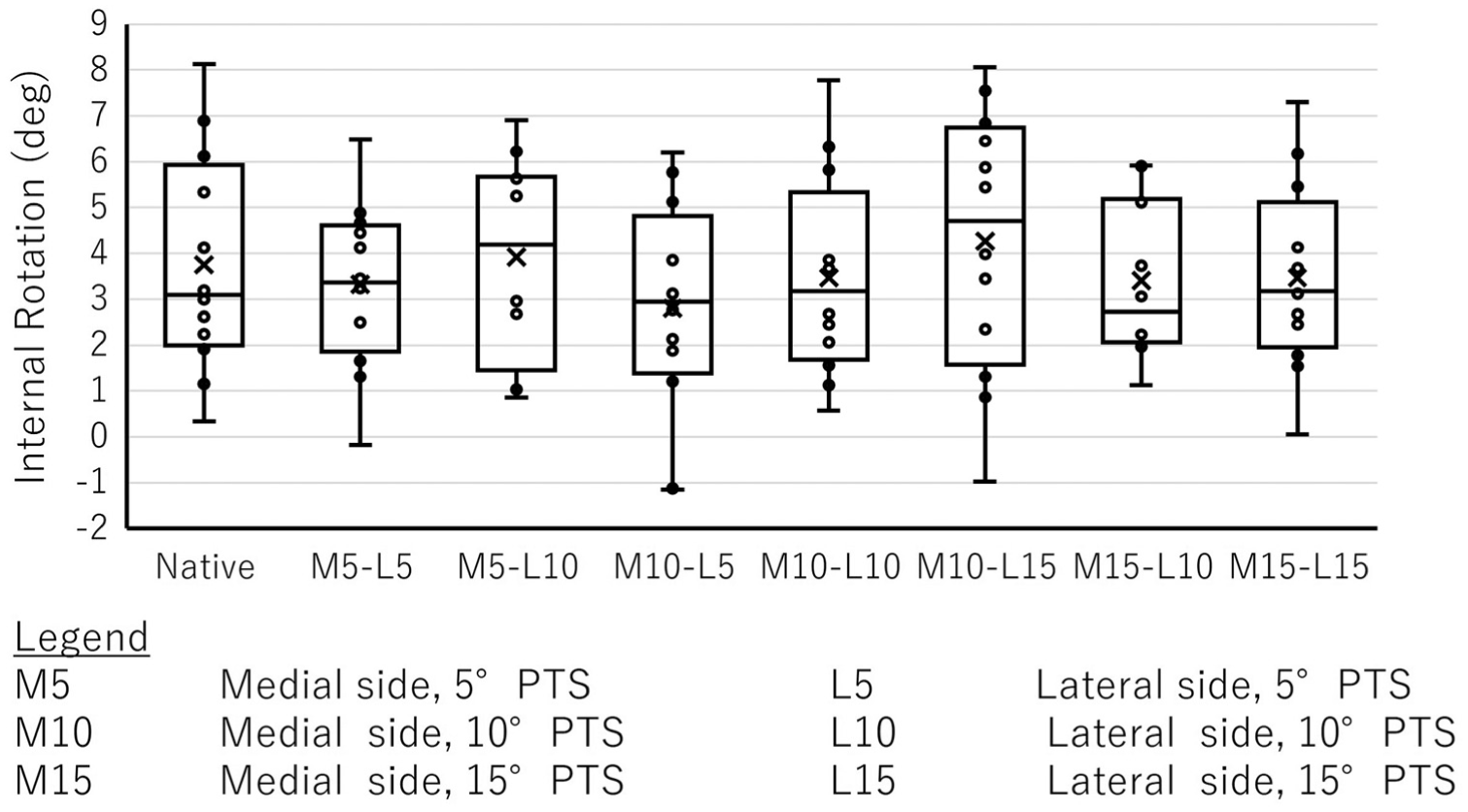
Box plot of tibial internal rotation (IR) with individual data points presented per combination of lateral and medial posterior tibial slopes (PTSs). The mean IR is labeled with an “x.”
Discussion
In the current study, medial and lateral PTSs independently and linearly influenced ACL graft force and ATT in ACL-reconstructed knees. Specifically, each 1° increase in lateral PTS was associated with a 4.9-N increase in graft force and a 0.63-mm increase in ATT, while each 1° increase in medial PTS corresponded to a 1.9-N increase in graft force and a 0.48-mm increase in ATT. These findings align with prior clinical and biomechanical studies, reinforcing the role of tibial slope as a modifiable risk factor in ACLR outcomes. Moreover, these results suggest that when planning a slope-reducing osteotomy, the surgeon may preferentially correct the PTS based on the lateral PTS versus the medial PTS.14,16
Although the changes in graft force and ATT were modest, this is likely attributable to the static loading and constrained boundary conditions used in the current model. The absence of dynamic loading states and the evaluation only at full extension may have limited the magnitude of observed differences. Under physiological dynamic conditions and across multiple flexion angles, greater variations in graft loading and tibial translation would be expected due to the combined influence of shear, compressive, and rotational forces acting on the reconstructed knee. Future studies incorporating dynamic muscle loading and multiplanar stress states will be critical to fully characterize the biomechanical implications of medial and lateral slope asymmetry under in vivo conditions.
Increased PTS has been consistently associated with increased anterior tibial shear forces, leading to heightened stress on the ACL graft. Bernhardson et al 2 demonstrated that ACL graft force increases linearly with PTS, emphasizing the biomechanical implications of slope variations. Ni et al 16 identified steep PTS and excessive ATT as predictive risk factors for primary ACLR failure, highlighting the clinical relevance of these anatomic features. Similarly, Pearce et al 17 reported that increased tibial slope correlates with higher ACL graft forces, underscoring the importance of slope considerations in surgical planning.
While both medial and lateral PTSs contribute to ACL graft loading, the lateral slope appears to have a more pronounced effect. Kataoka et al 11 found that a steeper lateral PTS and greater lateral-medial slope asymmetry correlated with a greater preoperative pivot shift, a relationship not found with increasing medial PTS. Christensen et al 5 found that increased lateral tibial slope was associated with early ACL graft failure, while Hinz et al 9 found that increased medial tibial slope was not associated with increased graft failure. Webb et al 18 further supported this by demonstrating a higher incidence of graft rupture in patients with a tibial slope >12°, particularly emphasizing the role of the lateral slope. Taken together, these studies suggest a greater biomechanical impact of the lateral tibial slope as compared with the medial slope. This greater effect of the lateral PTS may also apply to primary ACL failures, as found by 1 meta-analysis. 6 Our findings align with these studies, where lateral slope reduction resulted in a more significant decrease in graft force and ATT.
Interestingly, our data demonstrate that the changes in medial and lateral tibial slopes had no effect on tibial IR when the knee was positioned in full extension. Tibial IR control prevents the pivot-shift mechanism from occurring when the knee is flexed, and given that both the medial and lateral osteotomies are a pure sagittal slope change, it would follow that the ATT would be more affected than the tibial IR when the knee is fully extended. Using a computational model to determine the effect of a slope-reducing high tibial osteotomy on knee kinematics, Amirtharaj et al 1 found that a compressive load only increased ATT, while combined compressive and valgus forces were needed to increase tibial IR. Furthermore, the current study was specifically designed to avoid altering the coronal alignment by using medial or lateral spacers. However, combined changes in coronal and sagittal alignment may influence IR. Further research is necessary to determine if the IR is affected at higher flexion angles or by changes to coronal alignment.
Given the influence of PTS on ACL graft biomechanics, slope-reducing osteotomies have been utilized clinically with the correct indications. Bosco et al 3 conducted a systematic review and meta-analysis, concluding that anterior closed-wedge high tibial osteotomy is a viable option for patients with a high PTS undergoing ACLR. Our study supports this approach while going a step further by demonstrating that independently reducing the PTS of the medial and lateral plateaus can effectively decrease graft force and ATT, thereby potentially lowering the risk of graft failure. Additionally, our results demonstrate that the lateral slope has more influence on ACL graft loading, which may suggest that surgeons planning slope-reducing osteotomies with current techniques should preferentially aim to correct the lateral side. Further biomechanical testing is needed to stimulate modern operative techniques for slope-reducing osteotomy with preference given to the lateral PTS. These future studies should incorporate dynamic muscle loading and multiple knee flexion angles to better simulate in vivo joint mechanics during daily activities and athletic tasks.
Limitations
While our cadaveric model provides a controlled biomechanical model, the model only included static loading with the knee in full extension, does not account for dynamic muscle forces, does not account for long-term biological responses, and does not include multiplanar dynamic forces at varying flexion angles that place the ACL at increased risk of failure physiologically. Moreover, the mean age of the cadaveric specimens is 61.6 years, and the extensor mechanism and anterior capsule were dissected. Although older specimen age is common in cadaveric studies, this does not reflect the young athletic population with ACL injuries, and substantial differences in tissue quality exist in older populations that would not be seen clinically. Additionally, while the measurement method of medial and lateral slopes was modified from a validated method, 10 the method utilized in this study has not been validated, and alternative approaches to measuring PTS are commonly used in both clinical and biomechanical settings. Additionally, the technique for the osteotomy and fixation of the plateau, as described in this study, would be difficult to use clinically and needs further development for clinical translation. Finally, the study included a limited number of slope states and assumed a linear relationship between PTS and biomechanical outcomes, which may not fully capture potential nonlinear effects.
Conclusion
Although both slopes significantly affected ACL graft force and ATT, the lateral PTS had a greater effect on ACL graft force and ATT compared with the medial PTS and may warrant primary consideration during surgical intervention.
Footnotes
Final revision submitted November 10, 2025; accepted November 19, 2025
One or more of the authors has declared the following potential conflict of interest or source of funding: A.F.V. has received consulting fees from Arthrex and Stryker Corp, honoraria from Vericel Corp, speaking fees from Smith & Nephew, hospitality payments from BodyCAD USA, and support for education from Gemini Mountain Medical. M.T.P. has received royalties from Arthrex, Arthrosurface, Responsive Arthroscopy, and Anika Therapeutics; consulting fees from Arthrex, Joint Restoration Foundation (JRF), Zimmer Biomet Holdings, and Arthrosurface; grants from the Department of Defense (DoD), the National Institute of Health (NIH), and the DJO; and honoria from Flexion Therapeutics; is an editorial board or governing board member for SLACK; and board or committee member for AANA, AAOS, AOSSM, ASES, SDSI, and SOMOs; and served on the medical board of trustees for the Musculoskeletal Transplant Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.