
Abstract
Background:
Heterotopic ossification (HO) is a common complication after hip arthroscopy that has historically been prophylactically treated with postoperative radiation. Newer prophylactic treatments use nonsteroidal anti-inflammatory drugs (NSAIDs) in place of radiation.
Purpose:
To examine the incidence of HO after hip arthroscopy with and without the use of chemoprophylactic agents.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
PubMed and Scopus electronic databases were queried for all studies published between January 2000 and July 2025 that evaluated HO after hip arthroscopy. Information on study design, the use of exclusive NSAID chemical prophylaxis and regimen, presence of HO, and length of follow-up were collected from all studies. The Brooker classification was used for determining severity of HO. Matched-cohort studies were combined for meta-analysis and analyzed using the DerSimonian and Laird method of random-effects meta-analysis.
Results:
A total of 44 studies including a total of 32,603 patients were included. The incidence of HO in patients who received chemoprophylaxis after hip arthroscopy was 15.3 per 1000 patients per year compared with 80.1 per 1000 patients per year in those who did not receive chemoprophylaxis (P = .01). Patients who received chemoprophylaxis had a higher portion of Brooker 1 grade HO (73.6%) compared with patients who did not receive chemoprophylaxis (63.1%) (X2 = 8.6558; P = .03). Meta-analysis of 6 studies comparing chemoprophylaxis with no chemoprophylaxis had an odds ratio of 0.10 (95% CI, 0.03-0.35; P < .001).
Conclusion:
Postoperative NSAIDs were effective in reducing the incidence and severity of HO after hip arthroscopy. Meta-analysis of matched-cohort studies estimated a 10-fold decrease in the incidence.
Heterotopic ossification (HO) is defined as the abnormal formation of lamellar bone in soft tissue. 1 While the exact cause and mechanism of development are not fully understood, it is postulated that trauma or injury to a region of soft tissue recruits chondro-osseous progenitors, which result in the formation of mature lamellar bone.29,32 HO has been shown to be associated with neurologic injuries as well as tissue damage including burns and surgical sites. The development of HO most commonly presents with local pain, swelling, limited range of motion, and impingement of adjacent joints.17,20 A majority of patients with HO can be managed symptomatically; however, those with severe limitations require surgical intervention. 23
Hip arthroscopy is a common surgical procedure with an 85% increase in incidence, according to recent reports. 38 HO is a common complication after hip arthroscopy, with rates commonly reported between 1% and 12% of cases and some reports as high as 46%.7,14,20,33 To prevent postoperative HO, several prophylactic interventions have been utilized to disrupt chondrogenic signaling pathways to discourage bony formation. 5 Historically, prophylactic options included either radiation or chemoprophylaxis with bisphosphonates or nonsteroidal anti-inflammatory drugs (NSAIDs). 23 NSAIDs are preferred over radiation because of the easier method of administration and no risk of radiation–induced malignancy.
Among the various prophylactic options, NSAIDs are the most frequently utilized chemoprophylactic agents in the perioperative period. 12 The goal of this study was to determine the incidence of HO after hip arthroscopy with and without the use of NSAIDs. We hypothesized that prophylactic NSAIDs would reduce incidence of HO after hip arthroscopy.
Methods
Study protocol for this systematic review was performed following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A meta-analysis was performed on a subset of the included articles.
Search Strategy
PubMed and Scopus electronic databases were searched in July 2025 to identify all studies published between January 2000 and July 2025 that evaluated HO after hip arthroscopy. The following keywords and Medical Subject Headings terms were used in “Heterotopic Ossification” OR “HO” AND “Arthroscopy.”
Study Eligibility
The inclusion criteria were English-language studies reporting the incidence of HO after primary hip arthroscopy. All included studies were required to report if patients did or did not receive chemical prophylaxis; and, when prophylaxis was prescribed, what the prophylaxis regimen was, as well as what the agent used was. Studies were excluded if they included nonhip arthroscopy data, included revision hip arthroscopy, failed to state if chemical prophylaxis was or was not used, and failed to specify which prophylaxis was used. Studies were included if they contained data with all patients receiving prophylaxis. Systematic reviews, review articles, editorials or commentaries, instructional courses, case reports, and publications in languages other than English were also excluded. Two independent reviewers assessed the eligibility of each article (R.M. and D.M.). Reviewer disagreements were discussed, and a third independent reviewer (R.S.D.) was used to achieve consensus. The initial search identified 410 articles, of which 44 were included in the final analysis (Figure 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram demonstrating selection and screening for included papers in study.
Data Extraction and Statistical Analysis
The 44 included studies were evaluated, and data relating to study design, methodology, patient demographics, surgical procedure and indication, prophylactic agent utilized, use, dosing and length of treatment of postoperative prophylaxis, presence of HO adjacent to the operative hip, and length of follow-up. The Brooker classification system was used to determine the degree of HO from postoperative anteroposterior radiographs of the operative hip (Figure 2). 7 Data relating to symptoms from HO, revision surgery, and complications from prophylactic treatments were collected. Patients were grouped in 2 groups: prophylaxis group and no prophylaxis group.
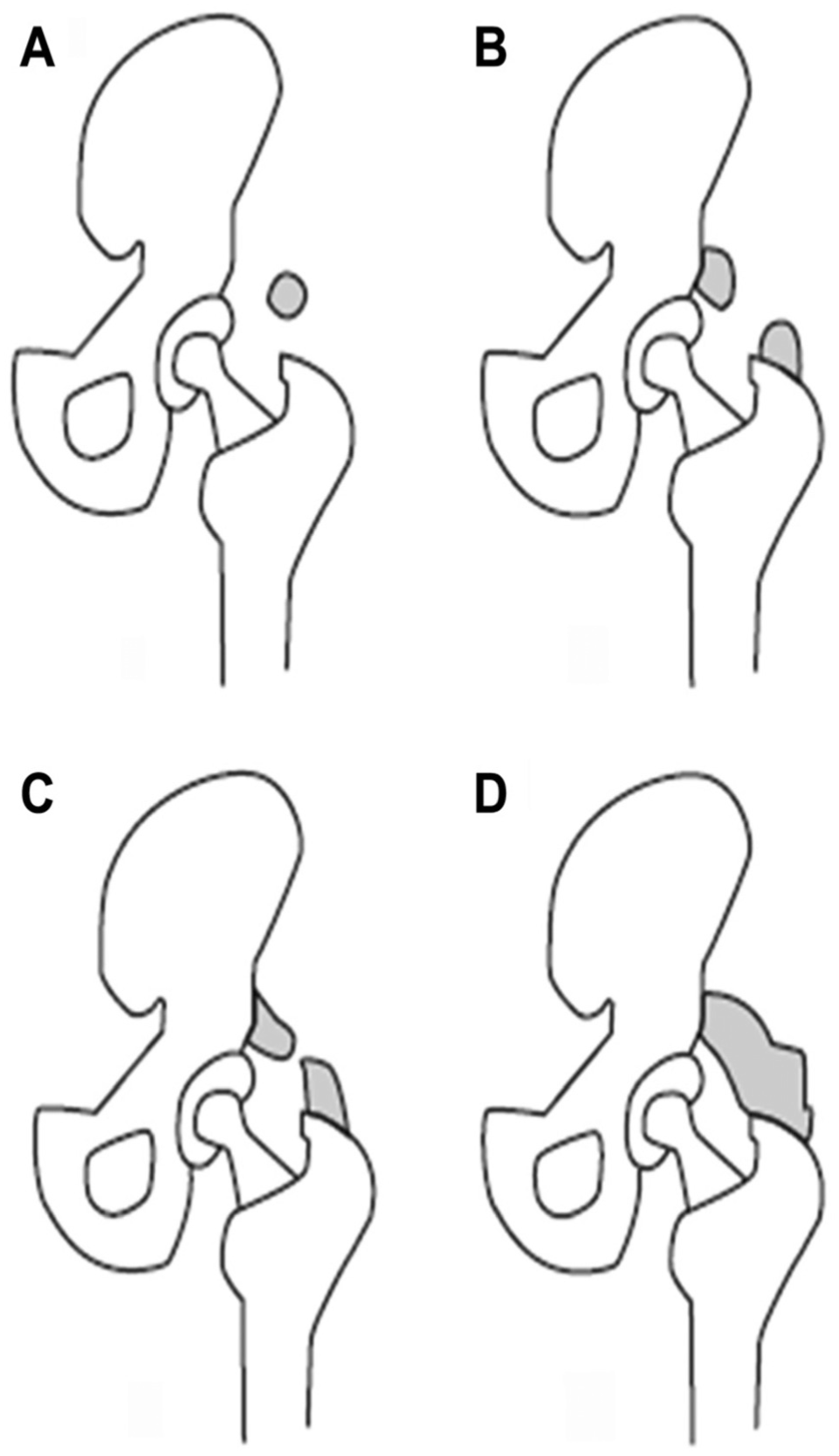
Brooker classification of hip heterotopic ossification. (A) Grade I is isolate bone island, (B) Grade II is bone spurs from acetabulum or greater trochanter with greater than 1 cm distance between ends, (C) Grade III is less than 1 cm between ends, and (D) Grade IV is bridging of the hip joint. Reproduced with permission from Bedi et al. 7
The risk of bias was assessed via the methodological index for non-randomized studies criteria. Higher scores are associated with a lower risk of bias, with a maximum score of 24 for comparative studies and 16 for noncomparative studies.
Descriptive data were listed as mean ± SD when appropriate, and continuous variables were compared using independent t test when normally distributed as determined by Anderson-Darling testing; otherwise, the Mann-Whitney U test was performed. Categorical data were compared using chi-square tests. Meta-analysis was performed on the subset of studies that evaluated HO in both non-prophylaxis and prophylaxis cohorts. The DerSimonian and Laird method of random-effects meta-analysis was used for all extrapolated and pooled outcome data. Heterogeneity between studies was quantified using I2, with values greater than 75% indicating high heterogeneity. Two-tailed P-values < .05 were determined to be statistically significant. All analysis and creation of tables and plots were performed using open-source R software Version 4.4.1. Because included studies recorded both the development of HO after surgery and patient follow-up, the incidence of HO was determined from the combined data.
Results
From the 44 studies, a total of 32,603 patients were included in the combined analysis. Of those, 7971 patients across 19 studies received NSAID prophylaxis postoperatively, whereas 24,632 patients across 30 studies did not receive prophylaxis of any kind.
Demographic factors relating to the combined data set are listed in Table 1. There were significantly more male patients in the prophylaxis group (53.5% vs 41.2%; P < .001). Age, body mass index, and length of follow-up were not statistically significantly different.
Patient Demographics of Included Studies, Compared Between Patients Receiving HO Prophylaxis and Those Who Did Not Receive HO Prophylaxis a
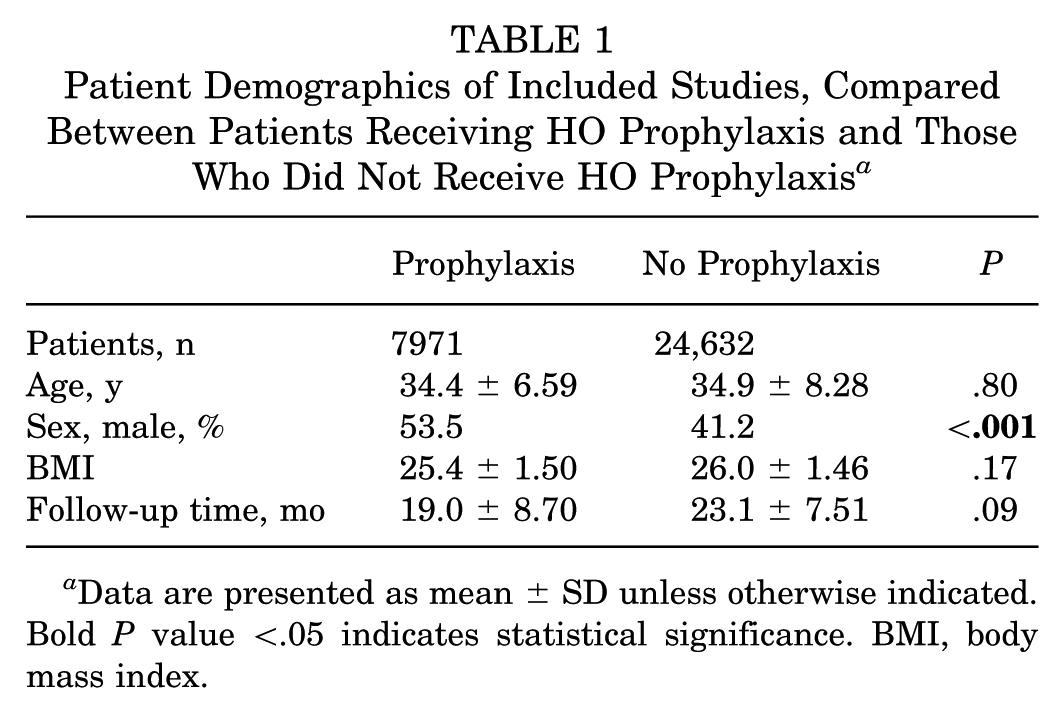
Data are presented as mean ± SD unless otherwise indicated. Bold P value <.05 indicates statistical significance. BMI, body mass index.
All but 27,23 of the included studies reported their indications for hip arthroscopy. The most common indications for hip arthroscopy among the included studies was femoroacetabular impingement (FAI): 7 studies included only those patients who underwent hip arthroscopy for FAI.3,4,9,19,20,22,25 Each of the remaining studies included cohorts made up primarily of FAI patients but also included pathologies such as hip dysplasia, 16 labral lesions, 8 chondromatosis, 28 and snapping hips. 28 Additionally, the most common surgeries performed were labral repair, labral debridement, femoral osteoplasty, acetabular osteoplasty, synovectomy, chondroplasty, microfracture, iliopsoas release.
Table 2 lists the number of patients in each group who developed radiographic HO after hip arthroscopy. Among the included patients, 8.0% of those who did not receive prophylaxis developed HO compared with 2.4% of patients with prophylaxis who developed HO; 22 studies included data relating to the severity of HO using the Brooker classification with a total of 163 patients from the prophylaxis group and 127 patients in the no prophylaxis group. The breakdown by Brooker classification is provided in Table 2. The prophylaxis group had a higher distribution of patients with Brooker 1 HO compared with the no prophylaxis group; this difference was deemed to be statistically significant (χ2 = 8.656; P = .03).
Development of HO Between Patients Who Received HO Prophylaxis and Patients Who Did Not (Severity of HO Subdivided Based on Brooker Classification) a

Data are presented as n (%) unless otherwise indicated. Bold P values indicate statistical significance. HO, heterotopic ossification.
Totals shown are the adjusted number of patients with HO in each group. Percentages are based only on studies that included data on Brooker classification.
χ2 = 8.656, P = .03.
For patients who did not receive prophylaxis, the incidence was 80.1 cases per 1,000 patients per year, which was statistically significantly higher than the incidence of 15.3 cases per 1000 patients per year in the patients who received chemoprophylaxis (P = .01).
Table 3 lists the different prophylactic regimens and the number of patients to receive each treatment. All included studies that used chemoprophylaxis used NSAIDs as the agent; however, there was wide variability in the specific medication used, dosing, and length of prophylaxis with 14 different protocols. The most used protocol overall was naproxen 500 mg twice daily for 3 weeks, which was used on 2760 patients between 5 different studies.5,11,21,28,33 Other NSAIDs used included aspirin, 31 diclofenac, 34 celecoxib,13,15 etodolac, 30 indomethacin,14,21 and etoricoxib. 27 The percentage of patients on each prophylactic regimen who eventually developed HO ranged from 0% to 36%.
Different HO Prophylactic Treatment Medication and Dosing Schedules a

χ2 = 588.487; P < .001. BID, twice a day; HO, heterotopic ossification; qD, once a day; TID, 3 times per day.
Six of the studies in the systematic review included both prophylaxis and no prophylaxis group. These data were pooled and underwent meta-analysis. The odds ratio for developing HO in the prophylaxis groups compared with those without prophylaxis was 0.10 (95% CI, 0.03-0.35; P < .001), indicating a statistically significant decrease in HO among those receiving prophylaxis (Figure 3).

Forest plot showing the individual odds ratios of the 6 studies to compare prophylaxis and no prophylaxis patients. Combined odds ratio with 95% CI as well as heterogeneity are included.
The studies included in this systematic review were inconsistent in reporting complications related to both side effects of NSAIDs as well as reoperations because of symptomatic HO after the initial procedure. Two studies report a total of 25 adverse events in 244 patients receiving HO chemoprophyaxis.5,6 This included 7 with gastrointestinal upset, 2 with heartburn, 3 reporting rash, 1 with acute renal failure, and 1 with acute colitis resulting in a total of 8 patients discontinuing NSAID prophylaxis because of side effects. Seven studies reported results on reoperation for symptomatic HO.6,7,13,14,16,31,36 A total of 228 patients among these studies developed HO with 59 undergoing resection. Among 6 of these studies, 17% of patients who received HO chemoprophylaxis and developed HO required resection (16/92), and 24% of patients who did not receive HO chemoprophylaxis and developed HO required resection (40/167). However, data collection was not sufficient for comparative analysis to determine if prophylactic NSAID use either increases risk related to side effects or decreases revision surgery for symptomatic HO.
Discussion
The primary findings of this study demonstrate that the use of NSAIDs postoperatively significantly decreases the incidence and severity of HO after hip arthroscopy. Despite the variety of NSAID regimens utilized, these medications helped mitigate the risk of developing radiographic HO. While most patients who develop HO will be asymptomatic, some will develop significant pain and stiffness to the point of requiring reoperation. 16 These findings provide surgeons with a pooled reference to justify NSAID prophylaxis for HO after hip arthroscopy.
The incidence of HO in patients without prophylaxis reported in this analysis was 8%, which is similar to previous studies.1,2,26 Comparatively, the incidence with the use of chemoprophylaxis was found to be significantly lower (2.4%). Results of the meta-analysis suggested up to a 10-fold decrease in HO after hip arthroscopy with chemoprophylaxis. NSAIDs have also been used recently in place of radiation for prophylaxis of HO in patients undergoing total hip arthroplasty, and while several meta-analyses show higher rates of HO in hip arthroplasty (9.6%-52.7%) as compared with hip arthroscopy, there is a similar ratio of decrease in incidence within patients who received prophylaxis.18,24,35 Isolated use of NSAIDs for surgical treatment of traumatic fractures, however, has not been shown to significantly decrease the incidence of HO when compared with no prophylaxis.3,22
Among patients who received prophylaxis, there was an additional benefit seen in the severity of HO. Based on Brooker classification, patients with chemoprophylaxis were likely to have lower grade HO. Interestingly, 73.6% of patients who received prophylaxis and subsequently developed HO were classified as Brooker 1, which is associated with no or minimal clinical symptoms. Conversely, 37.0% of patients without prophylaxis had a higher grade of radiographic HO according to the Brooker classification (Table 2). This suggests that NSAIDs prophylaxis not only decreased the incidence of HO formation, but also the severity of extra bone formation in patients who did end up developing HO. This is supported by the predicted role of NSAIDs in interfering with signaling pathways and altering osteoprogenitor cells, which modify the surrounding tissue to create an environment conducive to bone formation.4,9,19,25 In effect, while prophylactic NSAIDs may not entirely prevent HO in some patients, the blunted effect limits the extent of bone formation and potentially reduces clinical symptoms.
Our results indicated that NSAIDs were effective in reducing HO postoperatively, with a wide variability between the specifics of postoperative chemoprophylaxis. The most used prophylaxis method was Naproxen 500 mg twice daily for 3 weeks.5,11,21,28,33 Aspirin 325 mg twice daily for 6 weeks was used for a large number of patients; however, these were all from a large single study. 31 As a result, while NSAIDs overall showed a positive effect, it is difficult to discern whether one NSAID is better than another or if certain dosing regimens are more effective. Six of the included studies used COX-2 inhibitors for prophylaxis.7,10,15,27,30,34 COX-2 inhibitors are favored over other NSAIDs because of decreased side effects. 8 A recent meta-analysis by Zhu et al 37 demonstrated no difference in HO after total hip arthroplasty when comparing selective COX-2 inhibitors with nonselective NSAIDs. This suggests that selective COX-2 inhibitors can be considered when there is a contraindication to nonselective NSAIDs.
Limitations
While this study highlights the effectiveness of NSAIDs as prophylaxis for HO after hip arthroscopy, it is not without its limitations. First, there is significant variability between the postoperative prophylactic regimens. The benefits and risks of each type of NSAID, as well as prolonged NSAID use, should be considered. Further investigation is necessary to determine these effects on HO prophylaxis. The evaluation of HO from radiographs only has a high interobserver variability, and the used Brooker classification was originally designed for hip arthroplasty and later adapted for use in hip arthroscopy. Finally, the presence of HO is a radiographic finding that does not directly reflect patient symptoms after hip arthroscopy, and as such, the impact of HO prophylaxis on patient clinical outcomes is unclear.
Conclusion
HO is a common complication after hip arthroscopy. Postoperative use of NSAIDs is effective in reducing the incidence and severity of HO in the surgical hip. A meta-analysis of matched-cohort studies estimated a 10-fold decrease in incidence. Further evaluation of NSAID dosage and time is necessary to maximize the benefits of prophylaxis while limiting harm from side effects.
Footnotes
Final revision submitted September 23, 2025; accepted November 9, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.C. has received hospitality payments from Zimmer Biomet and Stryker. J.C. has received consulting fees from Arthrex, CONMED Linvatec, Ossur, Smith & Nephew, DePuy Synthes Products, and Vericel and hospitality payments from Stryker and Medical Device Business Services. S.J.N. has received research support from Allosource, Arthrex, Athletico, DJ Orthopedics, Linvatec, Miomed, Smith & Nephew, and Stryker; consulting fees from Stryker and Ossur; IP royalties from Ossur and Stryker; and publishing royalties and consulting fees from Springer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.