
Abstract
Background:
Reverse shoulder arthroplasty (RSA) requires deliberate preoperative planning and evaluation of glenoid deformity. The shoulder β and RSA angles, as described by Mauer and Boileau, respectively, are of value for preoperative planning for RSA.
Purposes:
To evaluate differences in relevant glenoid markers, such as the β and RSA angles, between plain radiographs and computed tomography (CT) scans and to further introduce and evaluate a novel measurement, the inferior glenoid bony resection depth (BRD), which is the resection distance required for placement of a baseplate in 0° of superior inclination.
Study Design:
Cohort study (Diagnosis); Level of evidence, 3.
Methods:
Patients with both plain radiographs and CT scans of the shoulder performed at the same institution within 3 months were reviewed. The shoulder β and RSA angles and BRD were assessed using radiographs and 2-dimensional CT scans. All radiographic measures were compared based on imaging modality (radiographs vs 2-dimensional CT scan). A subgroup analysis was conducted to evaluate differences between male and female patients.
Results:
In total, 41 patients were included. The mean β angle on radiographs was greater than when measured using CT (78.8° vs 76.9°, P = .02). The average resection depth was higher on radiographs as well (7.32 mm vs 5.86 mm, P < .001). Furthermore, men had a higher average β angle than women (81.6° vs 75.8°, P = .001).
Conclusion:
Plain radiographs may overestimate shoulder β angle and inferior glenoid resection. In addition, inferior glenoid resection depth necessary to achieve a neutral baseplate, as measured on both radiograph and CT, would lead to overresection of the glenoid, putting patients at risk for implant subsidence. We further found that there may be differences in glenoid inclination based on patient sex.
Reverse shoulder arthroplasty (RSA) is an effective and versatile treatment for osteoarthritis, rotator cuff tear arthropathy, and proximal humerus fractures. Annual volume of RSA is increasing in the United States as indications have expanded and surgeon familiarity has increased. 11 The optimal placement of the baseplate to restore function and facilitate durable bony ingrowth remains controversial. There are noted differences between placement of the glenoid component between total shoulder arthroplasty (TSA) and RSA. Specifically, in TSA, the glenoid component is generally centered in the glenoid vault, while the RSA glenosphere component is optimally positioned more inferiorly. 13 Inferior placement of the glenosphere distalizes the center of rotation, lengthens the deltoid, and helps limit impingement and subsequent scapular notching and prosthetic dislocation.2,9,13 In addition to inferior placement, neutral or inferior inclination relative to the supraspinatus fossa is preferred. Superior inclination is associated with failure of the glenoid baseplate and prosthetic instability and may be linked to numerous complications, including impingement, polyethylene wear, scapular notching, and diminished range of motion.5-8 Furthermore, overcorrection of superior inclination can lead to subsidence due to loss of subchondral bone. The global inclination of the glenoid can be described using the β angle, an angle between the floor of the supraspinatus fossa and the glenoid fossa. 10 This angle is most relevant to preoperative planning for anatomic TSA. 1 As such, Boileau et al 1 described the RSA angle to better account for the inferior positioning of the RSA glenosphere baseplate. The RSA angle is the angle created by a line perpendicular to the floor of the supraspinatus fossa and another through the inferior aspect of the glenoid fossa. 1
Placement of the glenoid baseplate perpendicular or with inferior inclination to the supraspinatus fossa can be achieved through inferior glenoid reaming, incomplete backside coverage, bone grafting, and/or the use of augmented baseplates. To determine the best approach, it is important to reliably and accurately measure a patient's native superior inclination, as defined by their β or RSA angle. Boileau et al 1 found significant differences between plain radiographs and 2-dimensional (2D) computed tomography (CT) scans, with an average RSA angle of 25° on radiographs versus 20° on 2D CT. Differences in the measurement of RSA preoperatively and intraoperatively will lead to variation in glenoid baseplate inclination and therefore differing amounts of inferior glenoid bone resection during reaming. To date, there are limited data regarding the optimal depth of glenoid bony resection. Similarly, there is a paucity of data regarding when an augmentation or bone grafting should be considered based on a patient's native superior inclination deformity.
The purpose of this study was to investigate systematic differences in β angle and RSA angle when measured using plain radiographs (radiographs) versus 2D CT scans. Next, we used radiographs and CT to compare the amount of planned inferior glenoid bony resection necessary for placement of a base plate perpendicular to the supraspinatus fossa. Given differences in projection on radiograph, we hypothesized that radiographs would overestimate the β angle, RSA angle, and resection depth needed to achieve a neutral or inferiorly tilted glenosphere.
Methods
Patient Selection and Demographic Data Collection
After institutional approval, the electronic imaging database was queried to identify 54 consecutive patients ≥18 years of age who had both plain radiographs and a noncontrast CT scan of the shoulder performed within 3 months of one another. Imaging studies were performed between 2019 and 2024. Exclusion criteria were any previous shoulder arthroplasty, bony surgery on the glenoid, and any fracture of the scapula. All imaging studies were completed at our institution's radiology department. All radiographs were reviewed to ensure that appropriate quality was met before a patient's inclusion in the study. Specifically, true anteroposterior (Grashey) views were analyzed to ensure that a tangential view of the glenohumeral joint space was clearly visible. Similarly, CT scans were reviewed before a patient's inclusion in the study. All included patients’ scans had axial, sagittal, and coronal cuts, and the images were evaluated to ensure appropriate formatting in the scapular plane.
After radiographic review, 6 patients were excluded due to insufficient quality plain radiographs, with the most frequent reason for exclusion being that no true anteroposterior (Grashey) view of acceptable quality was available. Seven patients were excluded because their axial CT scans were not formatted in the scapular plane. Patient demographic data were collected from the electronic medical record, including patient age, sex, and the primary shoulder diagnosis for which the CT scan was obtained.
Imaging Analysis and Measurements
Radiographs and CT scans were reviewed, and the shoulder β angle, RSA angle, and inferior glenoid bony resection depth (BRD) were measured.1,10 All measurements were performed using our institution's electronic imaging software (Synapse PACS; Fujifilm). Each patient was measured by 2 reviewers (B.M.L. and M.J.O.). The Grashey view of the shoulder was used for all radiographic measurements. The β angles were measured as previously described by measuring an angle between a line drawn through the supraspinatus fossa and a second line from the superior to inferior edge of the glenoid fossa (Figure 1). 1 RSA angles were measured according to the previously described technique by Boileau et al. 1 This includes drawing a line through the supraspinatus fossa and creating an angle with 1 line perpendicular to this line, starting at the inferior edge of the glenoid and another line extending from the inferior edge of the glenoid to the point on the glenoid fossa at which the line through the supraspinatus fossa transects the glenoid (Figure 2). 1 The β and RSA angles were measured on a coronal CT slice that was centered on the floor of the supraspinatus fossa identified on the sagittal view. We then obtained a novel measurement, the BRD. This was done by drawing a line perpendicular to the floor of the supraspinatus fossa and then using the ruler function to mark the distance from a point 4 mm superior to the inferior edge of the glenoid to the mark for the 0°β angle (Figure 3). The measurement was made 4 mm superior to the inferior edge of the glenoid to avoid being overly biased by the inferior glenoid morphology, calcified labrum, or the presence of inferior osteophytes. When analyzing an initial sample of radiographs and CT scans for 10 patients in the cohort, we found that 4 mm superior to the apparent inferior edge of the glenoid was most appropriate for approximating the native glenoid inferior margin, as inferior osteophytes and calcified labrum morphology were frequently encountered, particularly in patients with degenerative disease. Because these osteophytes may be removed at the time of surgery before glenoid baseplate placement, we elected to measure the BRD using the 4-mm correction to better approximate the resection of the native glenoid necessary to achieve a neutral baseplate. Patient glenoid morphology was also classified according to the Walch classification using axial CT cuts. 17

Shoulder β angle.

Reverse shoulder arthroplasty angle.
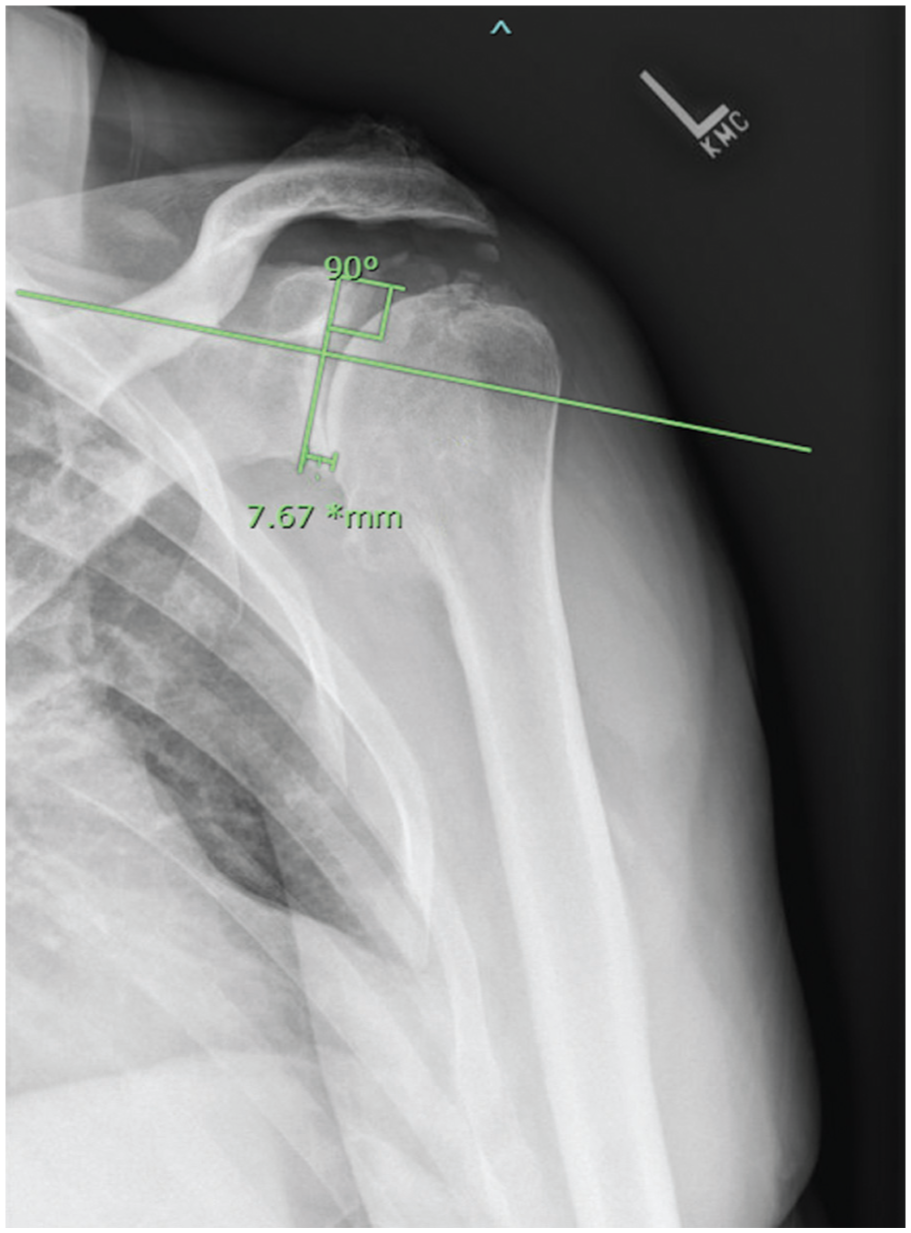
Shoulder bony resection depth.
Statistical Analysis
Descriptive statistics were used for patient demographic data using Stata (StataCorp). All radiographic measurements were collected by 1 reviewer and then repeated by a second reviewer for all patients. The mean of the 2 reviewers’ values was used for statistical analysis. A 2-tailed t test was used to compare measurements between radiographs and CT scans. We then identified outliers where the radiographic and CT measurements differed by >10° or where the BRD differed by >2 mm. Interobserver and intraobserver reliability were assessed using intraclass correlation coefficients (ICCs) with the ICC (2,k) form. To calculate intraobserver reliability, each of the 2 reviewers performed repeat radiographic measurements on 10 randomly selected participants, with ICCs calculated for each reviewer. Finally, we analyzed differences in radiographic measurements between male and female patients. We further calculated the absolute percent difference between male and female patients for each variable using female patients as the reference. Statistical significance was set at P < .05 for all analyses.
Results
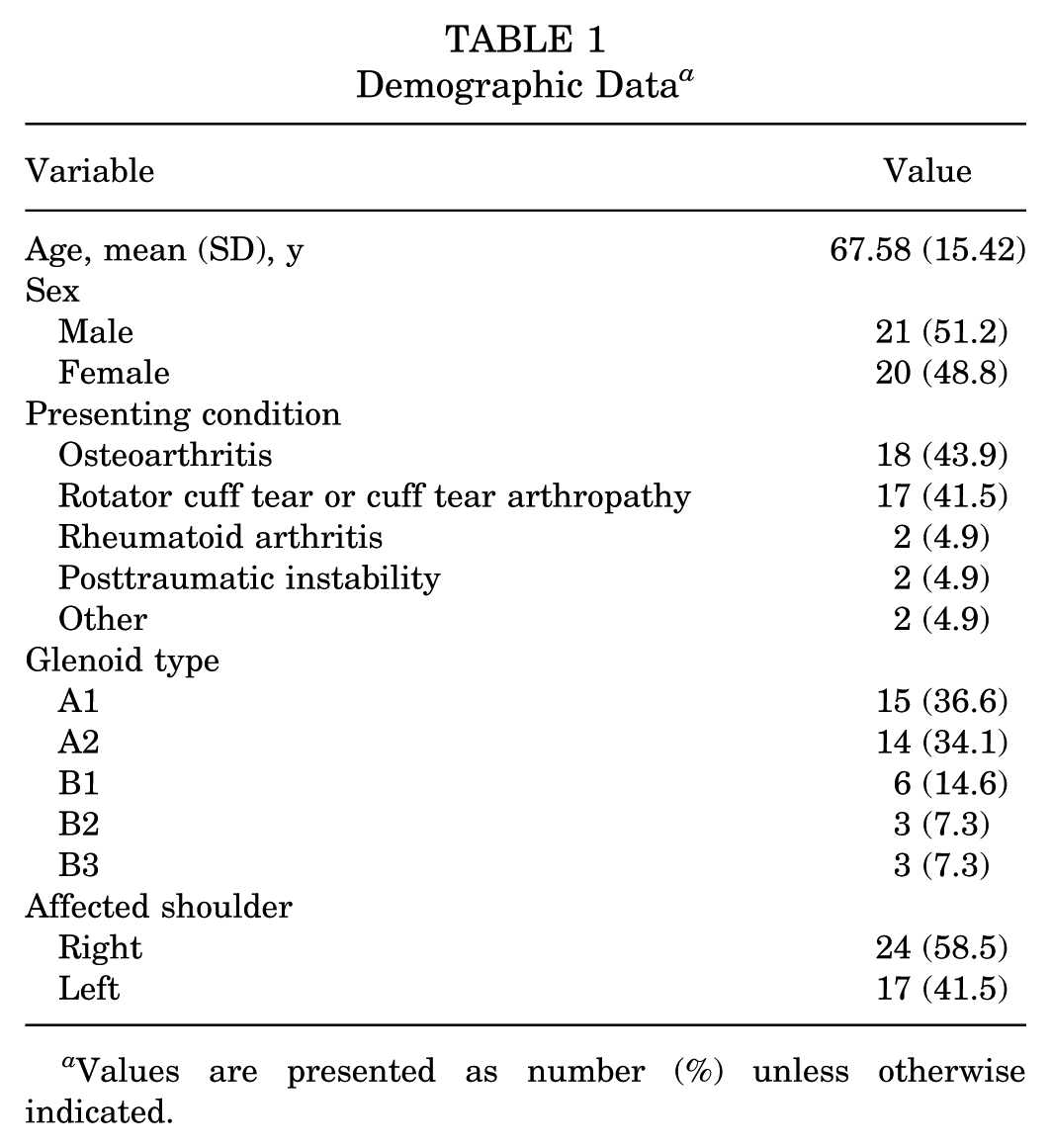
In total, 41 patients (20 women [48.8%], 21 men [51.2%]) were included in our final analysis. The mean (SD) patient age was 67.6 (15.4) years. The most common referring diagnoses were primary osteoarthritis (18 patients, 43.9%) and rotator cuff tear arthropathy (17 patients, 41.5%) (see Table 1). The mean β angle measured on radiographs was 78.8° versus 76.9° on CT scan (P = .02). The average RSA angle on radiographs was 20.7° compared with an average of 21.7° on CT scan (P = .34). The average BRD on radiographs was 7.32 mm as compared with 5.86 mm on CT scan (P < .001). This equates to a 19.9% difference in resection measurement between the 2 imaging modalities. Three patients (7.3%) had a β angle that differed by >10° on radiographs versus CT scan measurements. Nine patients (22.0%) had RSA angles that differed by >10°. In 14 patients (34.1%), the BRD differed by >2 mm for the 2 imaging modalities (Table 2).
Demographic Data a

Values are presented as number (%) unless otherwise indicated.
Radiograph Versus CT Scan Measurements of β Angle, RSA Angle, and Resection Depth a
BRD, bony resection depth; CT, computed tomography; RSA, reverse shoulder arthroplasty.
ICCs were calculated to determine interobserver reliability. Radiograph β angle had the highest ICC value at 0.956. Three measurements had ICCs >0.9 (radiograph β angle, CT β angle, and CT RSA angle), corresponding to excellent interobserver reliability. All interobserver ICC analyses produced values >0.75, corresponding to good interobserver reliability (Table 3). Intraobserver reliability ICCs showed high levels of consistency of measurements. Both reviewers had intraobserver ICC scores >0.7, with most scores >0.9 (Table 4).
ICC Measurements of Interrater Reliability a
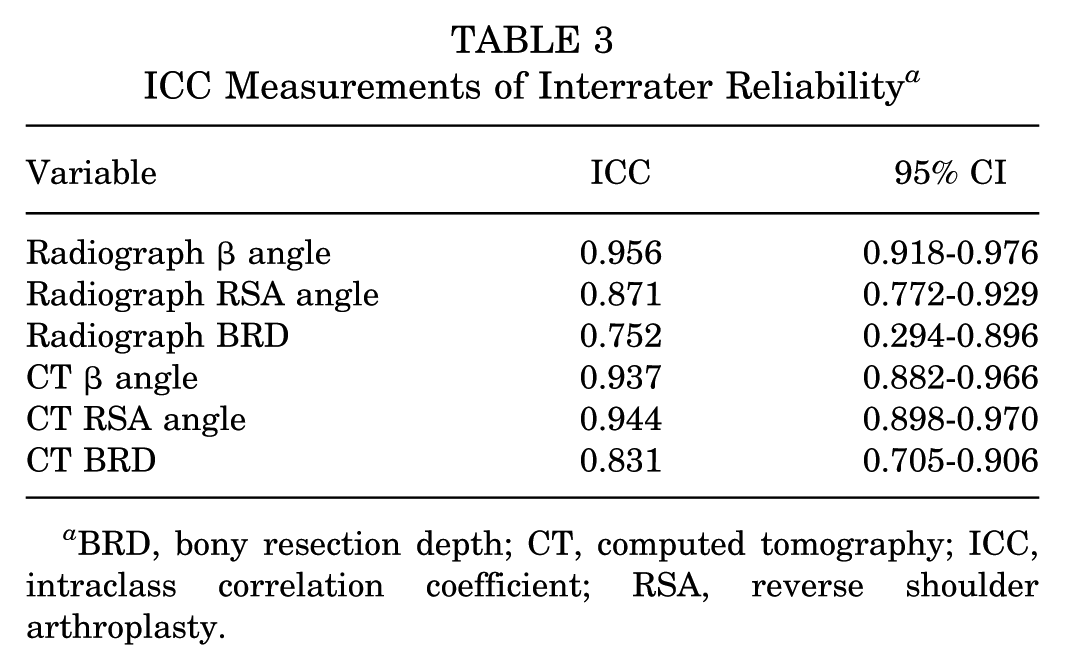
BRD, bony resection depth; CT, computed tomography; ICC, intraclass correlation coefficient; RSA, reverse shoulder arthroplasty.
ICC Measurements of Intrarater Reliability a

BRD, bony resection depth; CT, computed tomography; ICC, intraclass correlation coefficient; RSA, reverse shoulder arthroplasty.
Subgroup analyses were further performed. Among male patients, a statistically significant difference was found between radiograph and CT scan measurements for β angle (81.6° on radiograph vs 78.4° on CT scan, P = .01) and BRD (7.08 mm on radiograph vs 9.96 mm on CT scan, P = .002). There was no significant difference in RSA angle noted between male patients’ radiograph and CT scan measurements (P = .26). Among female patients, only the difference in resection depth was statistically significant (7.57 mm vs 5.76 mm, P < .001). Differences in β angle and RSA angle were not significant (P = .62 and P≥ .999, respectively). Finally, we performed a between-group analysis for the male and female patients in our cohort. We found a statistically significant difference in radiograph β angles, with men having a higher average measurement (81.6° vs 75.8°, P = .001). There were no significant differences observed with respect to radiograph RSA angle, resection depth, or any of the CT scan measurements. Tables 5 and 6 summarize these results.
Comparison of Radiograph and CT Scan Measurements of β Angle, RSA Angle, and Resection Depth Among Men and Among Women a

BRD, bony resection depth; CT, computed tomography; RSA, reverse shoulder arthroplasty.
Comparison of Radiograph and CT Scan Measurements of β Angle, RSA Angle, and Resection Depth Between Men and Women a
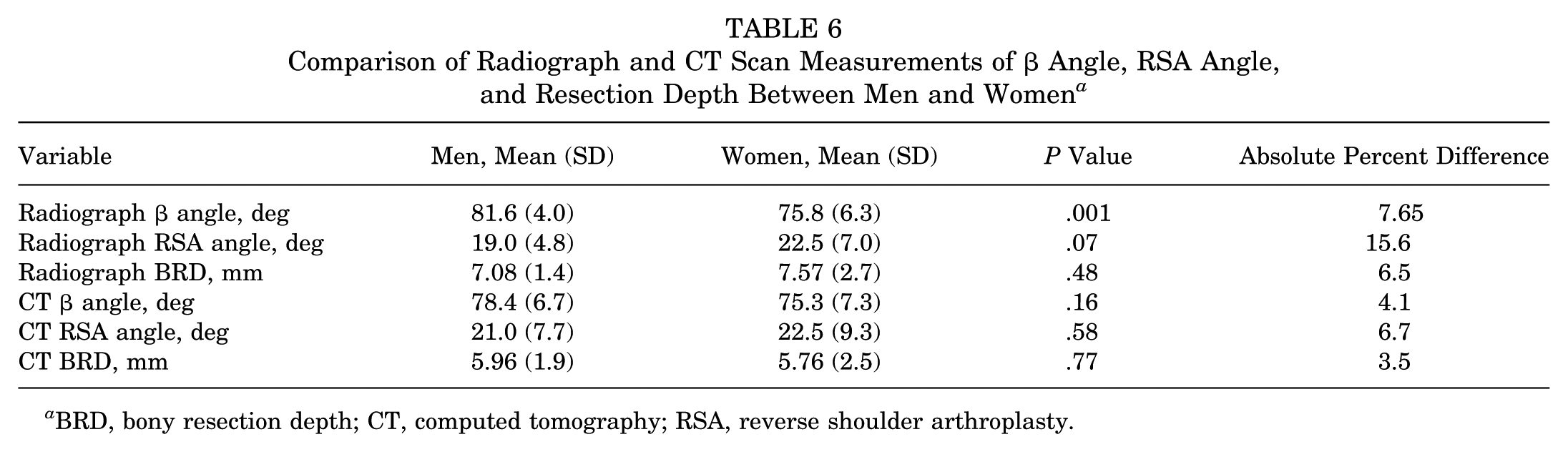
BRD, bony resection depth; CT, computed tomography; RSA, reverse shoulder arthroplasty.
Discussion
In this study, we compared radiographs and 2D CT scans for the measurement of shoulder β angle, RSA angle, and inferior glenoid BRD. All measurements had high interobserver and intraobserver reliability, including BRD, for which reliability of measurement had not been previously described. We found that a mean (SD) inferior glenoid BRD of 7.32 (2.1) mm on radiograph and 5.86 (2.2) mm (P < .0001) on CT scan would be required when planning a baseplate in 0° of superior inclination. This amount of inferior bony resection may lead to loss of the supportive subchondral bone and increase the risk for implant loosening. 15 This study highlights that regardless of imaging modality used, many patients may benefit from surgical techniques or augmented implants that preserve bone while still allowing surgeons to achieve a neutral or inferiorly inclined baseplate.
We additionally found that the mean β angle was 2° greater on plain radiographs as compared with CT scan, with excellent interobserver ICCs for both imaging modalities (radiograph β angle of 0.96 and CT β angle of 0.94). These data conflict with the findings of Boileau et al, 1 who found that plain radiographs underestimated the β angle as compared with CT scans. This may be due to systematic differences in how the radiographs were acquired or how the measurements were obtained. A previous study conducted by Daggett et al 4 compared β angle measurements on plain radiographs and 2D CT scans with a gold-standard 3-dimensional (3D) CT scan measurement. The authors found that 2D CT scans were more accurate than plain radiographs in determining accurate β angles. In addition, the authors found that 2D CT scans that were not formatted in the appropriate plane were highly unreliable for determining β angles. As such, in our present study, we opted to exclude any patients from final analysis if their CT scans were not properly formatted in the scapular plane. Of note, the present study focuses on optimal placement of the glenoid baseplate in RSA and how to use preoperative imaging modalities to achieve success. The RSA angle and BRD are most relevant for preoperative planning for this procedure, while the β angle is most important to consider before anatomic TSA. As such, differences in β angle measurements between radiographs and CT scans should be interpreted in this context and used selectively when preparing for anatomic TSA.
There was no significant difference between radiographic and CT measurements of the RSA angle (P = .33) in our study. However, in 22.0% of patients, the RSA angles differed by >10° when measured on radiographs versus CT scans. This may be due to differences in patient positioning, quality of the plain radiographs, or equipment used. There may also be errors in observer measurement; however, given that there was no difference in mean RSA angle between the 2 imaging modalities and the higher inter- and intraobserver reliability, the authors do not believe there is a consistent systematic difference in RSA angle between radiograph and CT imaging. Interobserver ICC values for RSA angle were 0.871 and 0.944 for radiographs and CT scans, corresponding to good and excellent agreement in measurement, respectively. In the original study by Boileau et al 1 on the RSA angle, the authors found mean RSA angles of 25° on radiographs and 20° on 2D CT scans, which is similar to the mean values obtained in the present study. While we did not find overall differences in RSA angle between the 2 imaging modalities, surgeons should be aware that in nearly one-fourth of cases, the RSA angles differed by at least 10° between plain radiographs and CT scans. This is particularly relevant for both preoperative planning and intraoperative execution, especially if intraoperative fluoroscopy is used for baseplate placement.
We found that the mean inferior glenoid BRD was 1.46 mm greater on plain radiographs compared with CT scans (P < .0001). Because the BRD and RSA angles use the same measurement of the supraspinatus fossa and anatomic point on the inferior glenoid, and given that there was no significant difference in RSA angle between radiographs and CT scans, we believe that the difference in BRD mainly arises from magnification on plain radiographs. Specifically, BRD is a linear measurement based on the RSA angle. It is important to note, however, that in over one-third of patients, the difference in resection depth differed by at least 2 mm, which is a significant amount of bony resection if performed intraoperatively. Regardless of the imaging modality used, this study indicates that correcting the RSA angle and placing a baseplate in 0° superior inclination with complete backside coverage would lead to overresection of the inferior glenoid in many patients. This could lead to loss of the supportive subchondral bone and increase the risk of implant loosening and subsidence. Further research is necessary to better elucidate this relationship and define how much bony resection of the glenoid is acceptable and what amount of native glenoid superior inclination requires adjunctive techniques such as augmented or inferiorly inclined baseplates, bone grafting, or planned incomplete backside coverage. Based on the findings in the present study, a large proportion of patients may benefit from implants or techniques that allow surgeons to both optimize baseplate fixation and biomechanics while limiting the risks of overresection of native bone stock.
Finally, we sought to investigate whether there were differences in native glenoid morphology based on sex. We found similar differences in resection depth among both male and female patients, with radiographs estimating a greater degree of resection (P = .002 for men, P < .0001 for women). Notably, when comparing male and female patients, we did not find significant differences in RSA angle or resection depth for either radiographs or CT scans. We did, however, find significant differences in β angles between the 2 sexes when measured using radiographs (P = .001). Male patients also had greater β angle measurements than their female counterparts when measured using CT scans, but these results were not statistically significant (P = .16). Piponov et al 14 reviewed 108 shoulder CT scans and found that male patients had larger and more retroverted glenoids. Merrill et al 12 further found differences in glenoid morphology based on sex, including a more ovoid glenoid shape for female patients compared with a rounder male glenoid on average. Tackett and Ablove, 16 however, did not find significant differences between the sexes with respect to glenohumeral relationships or glenoid version. The present study indicates that there may be an association between the inclination of the glenoid and sex. One previous anatomic study by Churchill et al 3 evaluated 172 cadaveric scapula samples of individuals aged 20 to 30 years at the time of death. The authors did not find a significant difference in glenoid inclination based on sex. Given the overall paucity of data regarding sex and glenoid inclination, further research is warranted to better understand this relationship and assist surgeons with preoperative planning for shoulder arthroplasty, as well as possible differences in future implant design parameters.
Limitations
There are limitations inherent to the present study design. First, there is the possibility of random or systematic measurement error. We sought to minimize this by standardizing measurement techniques and having reviewers perform measurements together on sample radiographs before initiating the study. The interobserver ICC values demonstrated good to excellent interobserver agreement overall, suggesting that all measurements, including the BRD, were reproducible in our study. Second, using a single number for BRD oversimplifies the 3D removal of bone during glenoid reaming. While alternate imaging modalities, including 3D CT scans, allow for a volumetric assessment of planned resection, these studies are rarely available intraoperatively or postoperatively; therefore, plain radiographs and 2D CT remain clinically relevant tools in planning and evaluating reverse shoulder arthroplasty. In addition, this study cannot definitively comment on what the gold standard is or should be for glenoid morphology measurements. Rather, the authors believe that surgeons should use the various imaging modalities described in this study, as well as 3D CT scans when available, to better understand a given patient's anatomy. Using this collection of data will allow surgeons to make maximally informed decisions both pre- and intraoperatively regarding glenoid baseplate positioning and bony resection. Furthermore, the use of appropriately formatted CT scans and radiographs is essential to increase the reliability of these measurements. Lastly, while our sample size is consistent with similar studies in the literature, 1 our sample size may be too small to detect differences in glenoid morphology. In particular, our study cohort was likely underpowered to detect differences in glenoid morphology based on sex. Further research with a larger cohort of patients is warranted to better understand these differences and the implications of sex-based morphologic variation for preoperative planning.
Conclusion
In this study, we demonstrated that both radiographs and 2D CT scans have good to excellent intraobserver and interobserver reliability for the measurement of shoulder β angle, RSA angle, and inferior glenoid BRD. There was no difference in mean RSA angle based on imaging modality, whereas the mean β angle was greater on plain radiographs. Due to the significant mean superior inclination of the inferior glenoid, we found that the inferior glenoid resection required to achieve a neutral baseplate may frequently lead to overresection of the glenoid, putting patients at risk for baseplate loosening and subsidence. Further research is needed to define how much resection of the inferior glenoid is acceptable and what amount of native glenoid superior inclination requires adjunctive surgical techniques or implants to optimize baseplate orientation while preserving supportive glenoid bone.
Footnotes
Final revision submitted September 14, 2025; accepted November 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.O. receives payments from Newclip and Smith & Nephew, is a paid consultant for Medacta, and receives financial/material support from SLACK Incorporated. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Southern California (#HS-22-00553).