
Abstract
Background:
Acetabular labral tears are frequently treated with arthroscopic repair using suture anchors. Iatrogenic chondral injury may occur during predrilling for suture anchors owing to factors such as portal location and drill guide type.
Purpose/Hypothesis:
The purpose of this study was to evaluate the effect of portal location and use of straight versus curved drill guides on drill perforation rates of the acetabular subchondral bone and outer cortex. It was hypothesized that curved guides and distal portals would minimize these perforation rates.
Study Design:
Controlled laboratory study.
Methods:
Nine cadaveric acetabula were marked at specific clockface positions (3:00 to 11:00) and drilled through anterior, anterolateral, and distal anterolateral accessory (DALA) portals using straight and curved guides. Ninety drill holes were analyzed for subchondral and cortical perforations. Statistical analysis included Fisher exact test and regression modeling.
Results:
A total of 90 acetabular suture anchor drill holes were created using each combination of portal (anterior, anterolateral, DALA), drill guide (curved, straight), and clockface position on the acetabulum. Among 90 drillings, 7 (7.8%) perforated the subchondral bone, and 10 (11.1%) perforated the outer cortex. Out of 45 drillings performed with a straight drill guide, 6 (13.3%) perforated the subchondral surface, as opposed to 1 (2.2%) with a curved drill guide. Of 30 drillings conducted via the anterolateral portal, 5 (16.7%) perforated the subchondral surface, as compared with 1 (3.3%) drilled from the DALA or anterior portal. Multiple linear regression based on portal, drill guide, and clockface position did not predict subchondral perforation (R2 = 0.08; P = .35) or outer cortical perforation (R2 = 0.04; P = .35).
Conclusion:
The use of anterior and DALA portals minimized subchondral perforation rates but was not statistically significant. Curved guides showed a trend toward reduced perforations when compared with straight guides. Articular surface penetration was most common at the 3:00 and 11:00 positions.
Clinical Relevance:
This study supports the use of curved guides and distal portals to enhance safety during arthroscopic acetabular labral repair, providing actionable insights for optimizing surgical techniques.
Keywords
Acetabular labral tears are frequently treated with arthroscopic repair using suture anchors. Short- and midterm outcomes of arthroscopic labral repair have demonstrated positive results.1,4,5,9,10,18 The procedure remains technically challenging and has a steep learning curve.2,17,23 Labral repair techniques have evolved over the past 2 decades. Suture anchor placement should be close to the acetabular rim to avoid eversion of the labral tissue and loss of the labral seal after repair.3,19,22 Proper anchor placement also avoids iatrogenic injury to the subchondral bone or intrapelvic structures. Several studies have helped identify optimal suture anchor position.8,11,15,20
Iatrogenic chondral injury is a commonly cited complication of labral repair during hip arthroscopy. Given the concave nature of the acetabulum, a potential complication of predrilling at the acetabular rim for suture anchor placement is iatrogenic penetration of the adjacent subchondral bone and overlying articular cartilage. Several factors play a role in drilling and placing suture anchors at the optimal position, including the need for acetabuloplasty (rim trimming), portal placement, drill angle, and the use of straight versus curved insertion guides.13,16,20 Acetabuloplasty has been shown to increase the rim angle (the angle between the subchondral margin and the outer cortex of the acetabulum), which makes placement of anchors safer. 15 Portal placement, specifically the use of distal-based portals, has been suggested to allow for safer anchor placement.8,11,16 A drill angle of 10° from a line perpendicular to the acetabular face was proposed as the proper angle for anchor drilling. 13 The use of a curved guide has been shown to increase the distance from the anchor to the acetabular surface, thus reducing the risk of chondral penetration. 20
In addition to the risk of damaging the articular cartilage, damage to intrapelvic structures with acetabular drilling can occur. One study attempted to evaluate the risk and found that the use of drills with a set stop point decreased the risk of intrapelvic penetration. 12
The purpose of this study was to evaluate the effect of the arthroscopic portal and type of drill guide (straight vs curved) on the frequency of articular subchondral bone and far cortical bone penetration during drilling for acetabular suture anchor placement on a cadaveric model. The use of cadaveric models more closely reflects true surgical conditions than manufactured models and allows for variances in acetabular morphology. Our hypothesis was that distal portals and curved drill guides would decrease the frequency of drill penetration of the subchondral and outer cortices.
Methods
This study was exempt from review from our institutional review board as it did not involve live human or animal subjects. This biomechanical study was performed with 3 separate acetabula from pelvic cadavers: 1 full hemipelvis specimen with an intact soft tissue envelope and 2 isolated bony acetabula. The single soft tissue specimen was used to reproduce soft tissue restraints and portal angles for all drilling on the other specimens. A full hemipelvis and 2 isolated acetabula with soft tissue envelope added to them were mounted in a neutral position, with the femoral head distracted 1 cm from the acetabulum to simulate arthroscopic hip anatomy (Figure 1). Portals were first created with the overlying soft tissues to simulate a realistic arthroscopic approach. After portal placement, the hip was disarticulated and the capsule removed to visualize and access precise clockface positions. The anterolateral (AL) poral was created at the intersection of the anterior and superior borders of the greater trochanter. The anterior portal was created at the intersection of a transverse line from the superior aspect of the trochanter and a longitudinal line from the anterior superior iliac spine. The distal AL accessory (DALA) portal was created 4 cm distal to and in line with the AL portal. The use of the AL portal for the 3-o’clock position reflects common surgical access trajectories in hip arthroscopy. Although the anterior portal is not typically used for the 11-o’clock position in clinical practice, we included this configuration to systematically evaluate penetration risks across various access points.

A full hemipelvis was mounted in a neutral position, with the femoral head distracted 1 cm from the acetabulum to simulate arthroscopic hip anatomy. Portals were initially created with the soft tissues to replicate arthroscopic conditions. The capsule was later removed to allow direct visualization for accurate drilling trajectory. The anterolateral portal was created at the intersection of the anterior and superior borders of the greater trochanter. The anterior portal was created at the intersection of a transverse line from the superior aspect of the trochanter and a longitudinal line from the anterior superior iliac spine. The distal anterolateral accessory portal was created 4 cm distal to and in line with the anterolateral portal.
The acetabulum of each pelvic specimen was marked at the acetabular rim at the 3:00, 2:00, 1:00, 12:00, 11:00, 10:00, and 9:00 positions (Figure 2).
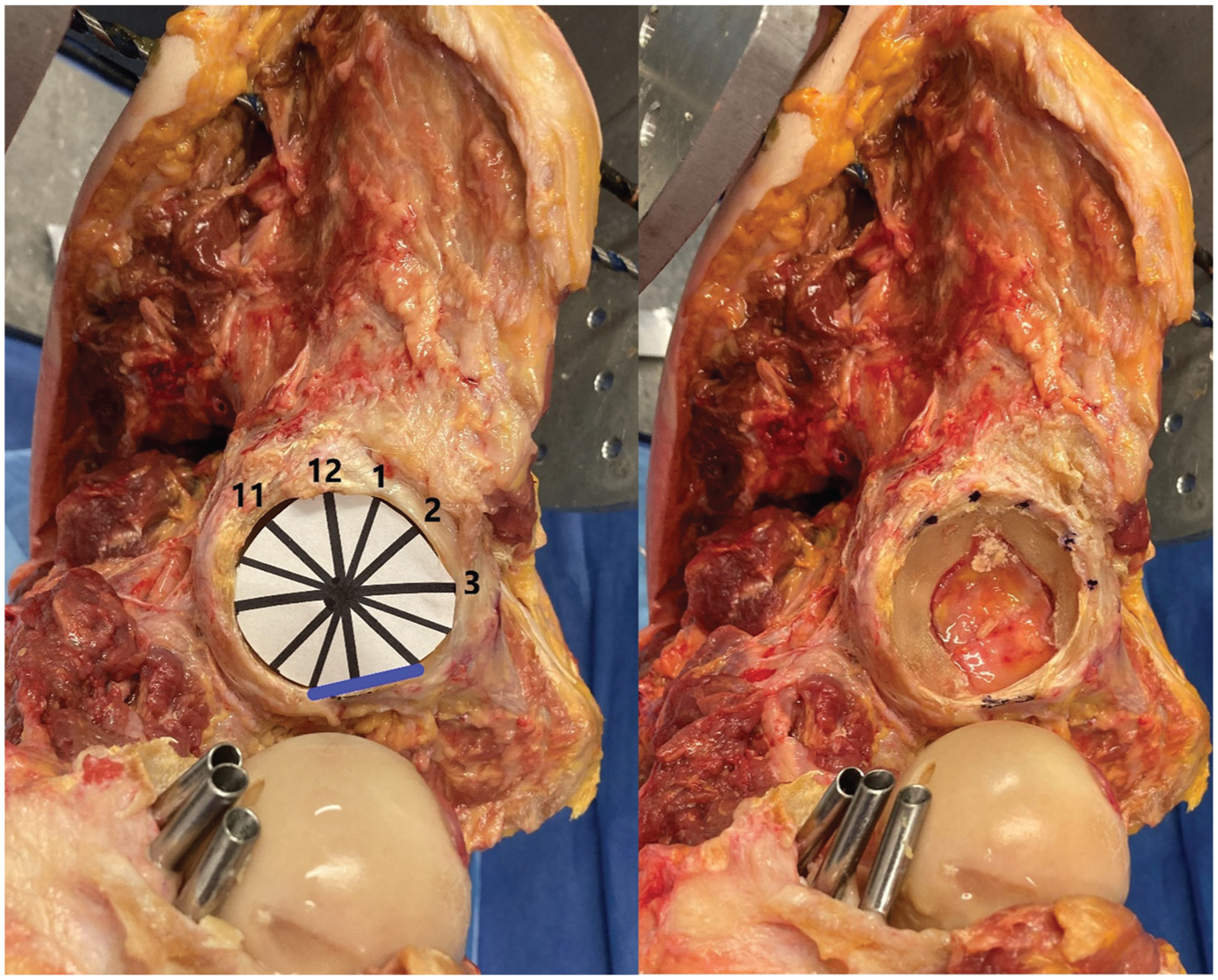
The acetabulum of each pelvic specimen was marked at the acetabular rim at the 3:00, 2:00, 1:00, 12:00, 11:00, 10:00, and 9:00 positions.
The acetabular clockface was marked per the conventional practice of the 6:00 position being the midpoint of the transverse acetabular ligament inferiorly and the psoas fossa being at the 3:00 position anteriorly. 21 Twelve groups of acetabula were created so that each combination of portal, drill guide, and start point was repeated 5 times. We utilized the Smith & Nephew Q-Fix 1.8-mm suture anchor drill guide. For the straight drill guide, the standard rigid drill bit was used and for the curved drill guide, the flexible drill bit. The specimens were each systematically drilled at the 11:00, 12:00, 1:00, 2:00, and 3:00 positions (Figure 3). The drill was inserted completely until a hard stop on the drill guide was reached. For each drilling trial, the presence or absence of penetration of the drill bit through the acetabular articular surface or far cortex was recorded.

The specimens were each systematically drilled at the 11:00, 12:00, 1:00, 2:00, and 3:00 positions. The drill was inserted completely until a hard stop on the drill guide was reached. For each drilling trial, the presence or absence of penetration of the drill bit through the acetabular articular surface or far cortex was recorded.
Statistical Analysis
Comparison of categorical variables was performed by the Fisher exact test (2 categorical variables) and the Pearson chi-square test (>2 categorical variables). Multiple linear regression models were created to identify factors that were associated with subchondral perforation or far cortical perforation. Statistical analysis was conducted in SPSS Statistics (Version 24; IBM SPSS). All reported P values are 2-tailed with an alpha level of .05 indicating statistical significance. 14 A post hoc power analysis assessed the adequacy of the sample size based on the observed perforation rates. The effect size was 1.95, representing a very large difference between the curved and straight drill guide groups. 6 With 20 specimens and α = .05, the post hoc power exceeded 99.99%, indicating that the study was sufficiently powered to detect clinically meaningful differences between groups.
Results
A total of 90 acetabular suture anchor drill holes were created by using each combination of portal (anterior, AL, DALA), drill guide type (curved, straight), and clockface position on the acetabulum. Out of 90 drillings, 7 (7.8%) perforated the subchondral bone, and 10 (11.1%) perforated the far cortex. Among 45 drillings performed with a straight drill guide, 6 (13.3%) perforated the subchondral surface, as opposed to 1 (2.2%) with a curved drill guide. Of 30 drillings conducted via the AL portal, 5 (16.7%) perforated the subchondral surface, as compared with 1 (3.3%) when drilled from either the DALA or anterior portal. Multiple linear regression based on portal, drill guide type, and clockface position did not predict subchondral perforation (R2 = 0.08; P = .35) or far cortical perforation (R2 = 0.04; P = .35). Frequency of articular subchondral penetration and far cortical penetration using each combination of variables is presented in Table 1.
Frequency of Acetabular Subchondral and Outer Cortical Perforation at Each Clockface Position by Grouping of Variables a
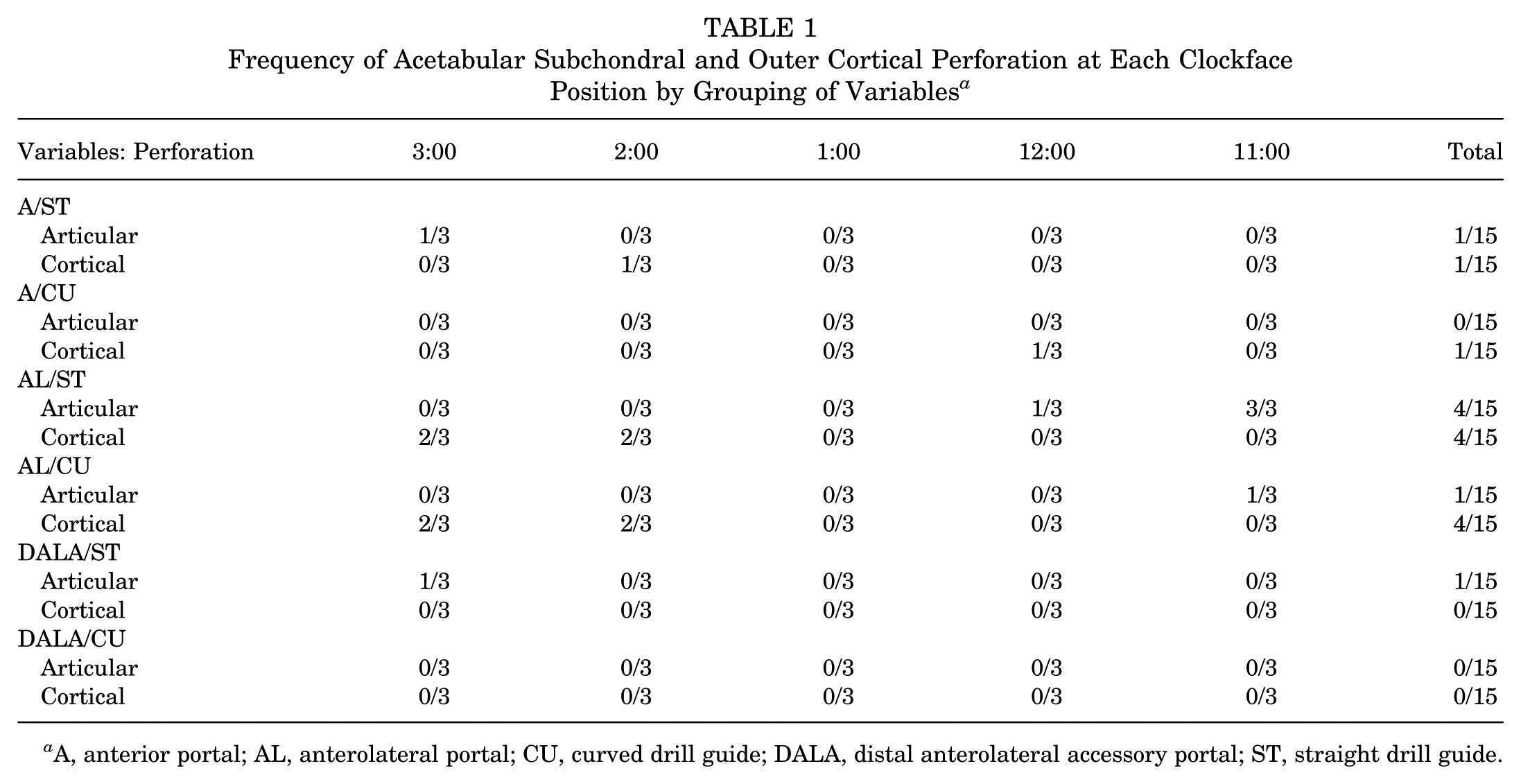
A, anterior portal; AL, anterolateral portal; CU, curved drill guide; DALA, distal anterolateral accessory portal; ST, straight drill guide.
Drilling from the anterior, AL, and DALA portals breached the articular subchondral bone on 1 (3%), 5 (17%), and 1 (3%) of 30 attempts, respectively. The use of the anterior and DALA portals resulted in the fewest articular subchondral penetrations. Drilling from the anterior, AL, and DALA portals breached the far acetabular cortex on 2 (7%), 8 (27%), and 0 (0%) of 30 attempts. Drilling from the DALA portal resulted in the fewest far cortical perforations.
Drilling with a straight guide breached the articular subchondral bone on 6 (16%) of 45 attempts, as opposed to 1 (2%) attempt with a curved drill guide (P = .059). Drillings with a straight guide breached the subchondral bone on 5 (11%) attempts. Drilling with a curved drill guide breached the far cortex on 5 (11%) attempts (P = .318).
Articular surface penetrations were most frequent at the 11:00 and 3:00 positions. Far cortical perforations were most common at the 2:00 and 3:00 positions. Table 2 details articular subchondral and far cortical perforations at each clockface position.
Acetabular Subchondral and Cortical Perforations at Each Position on the Clockface a

36 drillings were performed at each position.
Discussion
Our study provides a multifactorial analysis of factors affecting the risk of articular subchondral or far cortical bone penetration during drilling for arthroscopic acetabular labral repair. Our results demonstrate that an anterior portal or DALA portal, a distal-based portal, decreased the frequency of articular subchondral penetration as compared with the AL portal, although this was not statistically significant. Moreover, there were fewer articular subchondral penetrations when using a curved drill guide and flexible drill bit as compared with a straight drill guide and rigid drill bit, although this did not reach statistical significance. Unique to this study was the risk to the psoas tunnel, specifically when placing anchors from the AL portal. These findings were consistent with our previous study. 11
With regard to acetabular far cortical penetration, although not statistically significant, our results show that drilling from the AL portal increased the risk of penetration specifically at the anterior acetabulum (2:00 and 3:00). This result was a novel finding with this study.
Various studies have evaluated elements involved in optimal placement of suture anchors for acetabular labral repair. These factors include guide placement on the acetabular rim, the need for and effect of acetabuloplasty, portal placement, drill length, drill angle, and straight versus curved drill guides. Matsuda et al 16 reported on a small series of patients treated for anchor-induced chondral damage and suggested preventative measures such as using distal-based portals, smaller-diameter and shorter-length suture anchors, all-suture suture anchors, and curved anchor insertion instrumentation. Lertwanich et al 15 proposed the concept of the acetabular rim angle measurement. The acetabulum rim angle quantifies the angle between the subchondral margin and the outer cortex of the acetabulum. A higher angle indicates a broader safety zone for anchor insertion. The acetabular rim angle is dependent on the position on the acetabular clockface. The angle was largest (safest) at the 2-o’clock position and smallest (least safe) at the 3-o’clock position or psoas tunnel. Acetabuloplasty increased the acetabular rim angle, thus rendering suture anchor predrilling and insertion safer. Our study did not assess the effect of acetabuloplasty.
Hernandez and McGrath 13 recommended a safe angle of 10° from a line perpendicular to the acetabular face. In the study, the authors also utilized a start point slightly off the acetabular rim at the labral insertion (approximately 2 mm). A previous study evaluated the on-rim and off-rim drilling sites through a Sawbones model. 11 For this study, however, we utilized only the on-rim drill site, as the off-rim site can lead to eversion of the labrum and loss of the suction seal.19,22
Degen et al 8 performed a cadaveric study examining the safety of inserting suture anchors using a straight drill guide from the midanterior portal and the DALA portal. Their data revealed that overall 4.48% of anchors perforated the joint (4% from the midanterior portal and 4.95% from the DALA portal). They did not identify a difference at each position on the clockface. They also found no difference in the rate of psoas tunnel perforation when using the midanterior or DALA portal. They did not assess drilling from the AL portal, which demonstrated the highest rate of psoas tunnel perforation in our results. Both portals in the study by Dengen et al were distal based, which may explain why both had similar rates of articular subchondral or psoas tunnel penetration. Our study differs from their study in that we compared the DALA portal against standard AL and anterior portals, and we also utilized a curved guide.
Degen et al 7 evaluated perforation of the psoas tunnel at the anterior position on the acetabulum. Our results, although not significant, were consistent with far cortical perforation at the 2- and 3-o’clock positions. Anchor perforation and irritation of the psoas muscle have been postulated to be a continued source of pain after arthroscopic acetabular labral repair. 7 As our results differed from the initial Sawbones model, we postulate that it underrepresents the psoas tunnel.
Curved suture anchor guides with flexible drill bits have demonstrated increased angles of diversion away from the acetabular chondral surface. Nho et al 20 evaluated the use of curved (25°) and straight (0°) guides for suture anchor placement in 7 matched pairs of cadaveric specimens. The use of a curved guide significantly increased the insertion angle (divergence from the acetabular articular surface) at the 1:00, 2:00, and 3:00 positions and increased the distance from the tip of the suture anchor to the articular cartilage at the 1-o’clock position. While there were fewer articular perforations our study, we found no statistically significant advantage to using a curved drill guide. Conceptually, we expected to see decreased articular subchondral penetration using a curved drill guide. Nho et al utilized a 25° curved guide, in contrast to a 13° curved guide in our study. It is possible that using a guide with a more substantial curve would have further decreased the rate of articular subchondral penetration. Although guides with a more substantial curve could offer increased protection against articular subchondral penetration, their curve may make passage through standard arthroscopic cannulas difficult or impossible. This may be relevant for some surgeons depending on the surgical technique.
Damage to intrapelvic structures with acetabular drilling has been proposed. Gereli et al 12 investigated the risk of injury to neurovascular structures with increased drill length. Through-and-through penetration of the inner pelvis was noted to occur more commonly when drilling was performed at an angle with greater divergence from the acetabulum, but the use of a drill sleeve manufactured with a hard stop substantially reduced the risk of penetration to the inner pelvis regardless of drilling angle. Their study did not find any subchondral penetrations over a total of 60 drillings. Their study tested drilling with the guide at 10° or 20° from the coronal plane. The specific portal location simulated was not specified for this study, although this insertion angle is consistent with a distal-based portal.
There are limitations to this study. First, it was underpowered to show statistical significance. This was due to the availability of cadavers and the high cost of cadaveric work. The use of a soft tissue cadaveric model provides a realistic approach for portal placement, but owing to the variability of acetabular sizes, the model did not match each acetabulum precisely. We acknowledge that the small differences in drill trajectories (1-2 mm or 1°-2°) and the pressure from surrounding soft tissues cannot be fully reproduced in a cadaveric model. Furthermore, patient-specific anatomic differences, such as version and inclination, add complexity to anchor placement in live cases. Although our study confirms the trend of curved drill guides being safer in avoiding subchondral penetration, this does not consider the higher cost and increased breakage risk of curved drill guides, which must be balanced in clinical practice. Drill guides were positioned by direct visualization of the acetabular rim as opposed to arthroscopic visualization, which is most commonly used for suture anchor placement. Because we utilized a single cadaveric soft tissue model, we did not address the variations in hip soft tissue envelope that are typically encountered and can render portal placement suture anchor insertion more challenging. Last, the modified midanterior portal (MMAP) has become more common in recent years. Our study did not include MMAP trajectories, owing to its focus on standard portals in use at the time of study design and to the lack of widespread MMAP adoption at our institution during the study period.
Conclusion
The use of the anterior and DALA portals was associated with the lowest rate of acetabular subchondral perforation but was not statistically significant. While a trend toward reduced subchondral and cortical penetration was observed with the use of curved drill guides and specific portals, these findings did not reach statistical significance and should be interpreted with caution. Further studies with larger sample sizes are needed to validate these observations.
Footnotes
Final revision submitted August 11, 2025; accepted September 18, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.