
Abstract
Background:
Various exercise interventions are recommended to reduce the risk of anterior cruciate ligament (ACL) reinjury after ACL reconstruction (ACLR). However, the extent to which these training interventions influence lower-limb biomechanics in those who underwent ACLR remains unclear.
Purpose:
To determine whether existing exercise therapies can improve lower-limb biomechanical characteristics after ACLR.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
In accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, we searched PubMed, Embase, Cochrane Library, Web of Science, Scopus, and EBSCO to identify randomized controlled trials investigating the effects of exercise therapy on biomechanical characteristics after ACLR. The control group received conventional rehabilitation training, while the experimental group underwent various types of exercise therapy interventions. Seven kinematic and kinetic parameters were selected as outcome measures, and subgroup analyses were conducted based on testing tasks. The search timeframe spanned from database inception to June 3, 2025. The quality of the included studies was assessed using the Risk of Bias 2.0 tool. A meta-analysis was performed using Review Manager 5.3. Results are presented as standardized mean differences (SMD) with 95% CIs.
Results:
A total of 1512 studies were identified in the initial search. Twelve randomized controlled trials were included. Meta-analysis revealed that exercise therapy significantly increased the peak knee flexion angle (SMD, 0.51 [95% CI, 0.09 to 0.93]; P = .02) and hip extension moment (SMD, 0.39 [95% CI, 0.02 to 0.76]; P = .004) and reduced the peak knee valgus angle (SMD, −2.47 [95% CI, −3.54 to −1.41]; P < .001) compared with the control group. Moreover, the regulatory effect of exercise therapy on vertical ground-reaction force exhibited task dependency but had no significant influence on peak hip flexion angle (SMD, −0.34 [95% CI, −0.36 to 1.04]; P = .34), knee extension moment (SMD, −0.01 [95% CI, −0.33 to 0.35]; P = .95), or knee valgus moment (SMD, −0.32 [95% CI, −0.81 to 0.16]; P = .19).
Conclusion:
Our review demonstrated that exercise therapy can improve lower-limb biomechanical characteristics after ACLR. However, existing exercise therapy cannot fully restore biomechanical deficits in those who underwent ACLR. Further research is required to explore the effectiveness of targeted long-term training interventions.
This study has been registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration No. CRD420251066193).
Anterior cruciate ligament (ACL) rupture represents one of the most common knee joint injuries. 26 As the primary static stabilizer of the knee, the ACL plays a crucial role in maintaining normal movement and stability. 60 ACL rupture can lead to knee instability and functional decline and may progress to degenerative joint diseases due to recurrent instability episodes. 33 Given its severe consequences, most surgeons advocate ACL reconstruction (ACLR) surgery in active patients with knee instability after ACL rupture to improve knee stability and function.4,7 Although ACLR surgery is considered the “gold standard” for restoring preinjury athletic performance levels in athletes with ACL rupture, up to one-quarter of young athletes experience ACL reinjury upon returning to sports. 65 Compared with primary ACLR surgery, ACL revision surgery demonstrates significantly higher failure rates and comparatively poorer postoperative knee joint functional recovery. 66 Therefore, identifying risk factors for ACL reinjury and establishing evidence-based strategies with targeted training interventions to reduce the risk and burden of ACL reinjury is crucial in the field of sports medicine.
The underlying causes of ACL reinjury are multifactorial, extending beyond the muscle strength and/or functional performance deficits traditionally considered in return-to-sport testing, and involve abnormal biomechanical characteristics in patients after ACLR. 37 A prospective study demonstrated that compared with those who underwent ACLR but did not experience reinjury, those who experienced reinjury exhibited reduced hip external rotation moments, increased knee valgus angles, and asymmetrical knee sagittal plane moments during initial contact in bilateral vertical jump tasks. 46 Furthermore, a reduced knee flexion angle diminishes the potential to absorb vertical ground-reaction force (VGRF), subsequently increasing knee joint loading and reinjury risk. 16 Collectively, these studies demonstrate the identification of abnormal loading strategies and may help clinicians develop rehabilitation protocols to lower the risk of reinjury.1,2
Exercise therapy is an indispensable component for improving muscle strength and functional capacity and is recognized as the cornerstone of postoperative rehabilitation after ACLR. 35 Current research has synthesized evidence regarding the effects of exercise therapy after ACLR.3,29 However, most studies have focused solely on knee joint muscle strength and proprioception outcomes but have overlooked the assessment of biomechanical characteristics.3,29 Evaluation of the efficacy of exercise therapy through biomechanical testing can help identify the strengths and limitations of current training interventions and provide guidance for developing future ACLR treatment methods targeting biomechanical deficits. Therefore, this study aimed to comprehensively assess the effectiveness of exercise therapy on biomechanical characteristics after ACLR by synthesizing and analyzing high-quality randomized controlled trials (RCTs), while exploring the influence of various variables (eg, duration, frequency, and total intervention time) on biomechanical outcomes. We hypothesized that exercise therapy would significantly increase the knee extension moment and the peak knee flexion angle and decrease the peak knee valgus angle.
Methods
Protocol and Registration
This review was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 57 The study protocol has been registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration No. CRD420251066193). The PRISMA checklist is listed in Appendix Table S1.
Search Strategy and study selection
A comprehensive search was conducted across PubMed, Embase, Cochrane Library, Web of Science, Scopus, and EBSCO to identify studies evaluating the effects of exercise therapy after ACLR. All relevant articles published globally in any language from database inception to June 3, 2025, were included, without publication date restrictions. The search utilized a combination of Medical Subject Headings (MeSH) terms and keywords. Search terms included “Anterior Cruciate Ligament Reconstruction,” “Anterior Cruciate Ligament,” “ACLR,” “ACL,” “Exercise Therapy,” “Rehabilitation,” “Exercise,” and “Therapeutics.” Detailed search strategies are provided in Appendix Table S2. The search was conducted by 2 independent researchers following the search formula (P.C. and JF.Y.). Discrepancies were resolved through consultation with a third researcher (H.Z.). EndNote X9 software was used to screen and manage the identified reports, removing all duplicate articles. Articles were screened according to the inclusion/exclusion criteria.
A 3-stage process was followed to identify relevant articles. Articles were included in the first stage if they investigated biomechanics related to pre- and post-training interventions associated with ACL reinjury during dynamic tasks. In the second phase, abstracts of each study were screened to exclude those that did not report outcomes after ACLR. The third phase involved reviewing the full texts of all relevant studies that met the eligibility criteria for final inclusion. Both authors independently performed all these tasks. The first and second authors (P.C. and JF.Y.) discussed and resolved potential discrepancies in study inclusion and exclusion criteria, and a third author (HW.Z.) was consulted as needed to reach consensus. Reference lists of included studies were screened by 1 author (L.W.) to identify any additional studies relevant to this review.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) participants: studies involving patients after ACLR with no restrictions on sex, graft type, competition level/experience, or activity level; (2) intervention: implementation of ≥4 weeks of training interventions, such as functional resistance training, neuromuscular training, or core stabilization programs; 50 (3) comparison: control group receiving conventional rehabilitation training; (4) study type: RCTs; and (5) outcomes: reported lower limb kinematics (flexion/extension, adduction/abduction, or internal/external rotation angles) or kinetics (joint moments or VGRF) during dynamic tasks (eg, gait, single-leg landing) pre- and post-intervention, measured using 2-dimensional (2D) or 3D motion capture systems. The exclusion criteria were as follows: (1) studies investigating biomechanical risk factors associated with ACL injury in healthy participants; (2) studies that did not report biomechanical variables during dynamic tasks; (3) case reports or descriptive studies or studies not published as peer-reviewed journal articles, including dissertations, book chapters, and conference abstracts; (4) articles not published in English; (5) studies with duplicate publications, where 2 studies by the same author reported identical data for the same variables and groups across different publications; duplicate data were removed and a single record was used for analysis.
Data Extraction
Data extraction was independently conducted by 2 researchers (JF.Y. and HW.Z.). In cases of disagreement, a third researcher (L.W.) participated in decision-making. The following data were extracted from the included articles: (1) author names and publication year; (2) participants' age and sex; (3) physical activities and levels; (4) testing tasks employed in the studies; (5) data collection methods; and (6) outcome measures. Kinetic measures included knee flexion and valgus moments, hip flexion moment, and VGRF. For kinetic measures, phases of interest included discrete values at peak knee flexion angle/VGRF or peaks during the test task, as these are generally considered the phases when the ACL is most susceptible to injury. 38 Inconsistent sign conventions across included studies were standardized as follows: hip flexion, knee flexion, knee valgus angle, and moment were defined as positive values. Studies reporting moment units as Nm or Nm/kg were included in the meta-analysis. If the included studies lacked essential information, the first or corresponding author was contacted by email to request the missing data. If the authors did not respond to the initial email, then a follow-up email was sent 1 week later. Studies were excluded from the analysis if no response was obtained after 2 attempts or if the authors could not provide the required data. For data reported in graphical format, GetData Graph Digitizer was employed to extract numerical values because this method has been validated as an effective procedure. 14
Quality Assessment
Two independent reviewers (JF.Y. and HW.Z.) evaluated the risk of bias in included studies using the Cochrane Risk of Bias Tool (Version 2; Cochrane). Two researchers summarized the overall quality of evidence using the Summary of Findings table generated through the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework. 57 In cases of disagreement, a third researcher (L.W.) was consulted to assist in adjudication.
Statistical Analysis
Review Manager (RevMan) 5.3 (Cochrane) was used for meta-analysis. Pooled effect estimates were calculated using changes in numerical values from baseline to postintervention, their standard deviations, and the total number of participants. When standard deviations were not provided, they were computed based on standard errors or 95% CIs. 14 A correlation coefficient of 0.5 was assumed when calculating standard deviations for pre- and post-intervention differences. This hypothesis was based on the generally accepted moderate level of measurement reproducibility in the literature. This value was selected to balance potential variability between pre- and post-measurements while ensuring conservative and reliable outcomes. 14 The standardized mean difference (SMD) was adopted as the effect size measure because of differences in measurement methods, and the corresponding 95% CI was calculated. The I 2 statistic was used to examine study heterogeneity. Studies with I 2 values >50% were considered to have high heterogeneity. 28 Sensitivity analysis was performed by excluding studies one at a time to test the robustness of the results. If at least 10 comparisons are included, funnel charts are used to assess publication bias. 40 Univariate meta-regression was performed to explore sources of heterogeneity when >10 comparisons were included. Variables of interest included the type of intervention, the start time of the intervention, the intervention period, the percentage of males, and the mean age. Missing data were imputed using the mean substitution method. 43
Results
Literature Selection and Characteristics
Electronic databases and manual searches yielded 1512 articles, of which 567 were duplicates and 846 were excluded based on title and abstract screening. A total of 100 full-text articles were further screened, of which 12 RCTs8,9,15,19-23,30,31,42,54 fully met the inclusion criteria and were included in qualitative analysis, while 10 studies8,9,15,19,21-23,30,42,54 were included in the meta-analysis (Figure 1).

PRISMA flowchart of the study selection process. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Our review included 372 knees (198 in the experimental group and 174 in the control group). The mean age of participants was 24.5 years. Only 2 studies reported the types of physical activities, such as basketball, volleyball, and handball. Participants' athletic levels ranged from recreational to professional, although 4 studies did not provide this information. Appendix Table S3 presents detailed descriptions of participant characteristics.
The articles included in our review aimed to examine exercise biomechanics after ACLR during pre- and post-training interventions. Six studies15,20,22,23,30,54 required participants to perform single-leg drop/hop landing, 6 studies8,9,19,21,31,42 implemented comfortable-speed gait analysis, while 2 other studies30,42 used lateral cutting and running tests (one study 30 evaluated cutting and single-leg hop landing, and the other 42 evaluated walking and running). The required jump height primarily ranged between 25 and 30.5 cm. Ten studies8,9,15,19,21-23,30,31,42 collected kinematic data using 3D motion capture systems, while 1 study 54 employed 2D cameras. One study 20 did not report any kinematic data. Regarding training interventions, 2 studies21,31 utilized functional resistance training, 2 studies15,22 implemented neuromuscular training, 2 studies8,9 employed secondary prevention exercises plus perturbation training, 2 studies20,54 conducted core stability training, and 1 study 23 used visual motor training and differential learning training, with 3 additional studies19,30,42 respectively applying blood flow restriction training, proprioceptive training, and eccentric training. The duration of training interventions ranged from 5 to 52 weeks, with a frequency of 2 to 7 sessions per week. Appendix Table S4 presents all detailed information regarding the training interventions and outcomes reported in the included studies.
Risk of Bias
Among the 12 included studies, 2 studies15,31 (16.7%) were classified as low risk, 6 studies8,9,20,22,30,42 (50%) as moderate risk, and 4 studies19,21,23,54 (33.3%) as high risk (Appendix Figure S1). Eleven studies8,9,15,19-23,30,31,42 explicitly described their randomization methods, which primarily involved computer-generated random sequences or random number tables. Only 3 studies15,30,31 reported no deviation from intended interventions, indicating a high risk in this aspect. None of the 12 studies reported missing outcome data, reflecting a lower risk in this domain. Twelve studies8,9,15,19-23,30,31,42,54 demonstrated appropriate measurement of outcomes, and 6 studies8,15,20-23 explicitly stated the absence of selective outcome reporting (Appendix Figure S2).
Meta-analysis Findings
Peak Knee Flexion Angle
Figure 2 presents the results of the meta-analysis for peak knee flexion angle. This outcome measure included 13 pairwise comparisons. A random-effect model was employed for the meta-analysis because of the high heterogeneity among studies (I 2 = 75%; P < .001). The meta-analysis results showed that exercise therapy significantly increased the peak knee flexion angle (SMD, 0.51 [95% CI, 0.09 to 0.93]; P = .02) compared with the control group. Subgroup analysis revealed that exercise therapy significantly increased the peak knee flexion angle during landing tasks (SMD, 0.85 [95% CI, 0.22 to 1.48]; P = .008) but showed no significant effect during walking tasks.
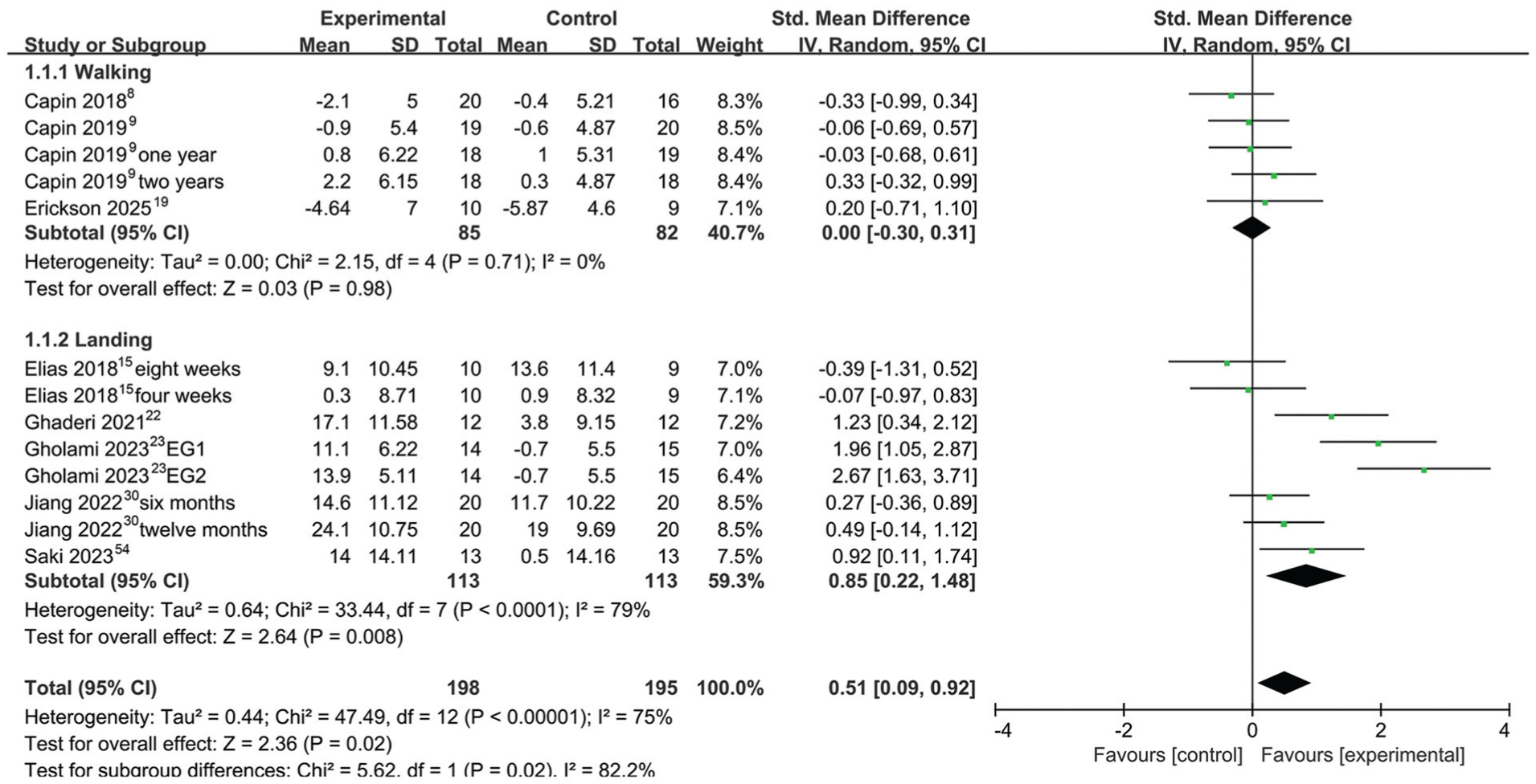
Forest plot of peak knee flexion angle. EG, experimental group; IV, inverse variance; Std, standardized.
Peak Knee Valgus Angle
Five studies reported outcomes on the peak knee valgus angle, with substantial heterogeneity among the literature (I 2 = 84%; P < .001). A random-effects model was employed for analysis. Meta-analysis results showed that exercise therapy significantly reduced the peak knee valgus angle (SMD, −2.47 [95% CI, −3.54 to −1.41]; P < .001) compared with the control group. Subgroup analysis revealed that exercise therapy significantly reduced the peak knee valgus angle during landing (SMD, −3.07 [95% CI, −5.38 to −0.76]; P = .009) and cutting (SMD, −1.82 [95% CI, −2.35 to −1.29]; P < .001) tasks (Figure 3).

Forest plot of peak knee varus angle. EG, experimental group; IV, inverse variance; Std, standardized.
Peak Hip Flexion Angle
Figure 4 illustrates the results of the meta-analysis on the peak hip flexion angle. This outcome measure included 5 pairwise comparisons. Given the substantial heterogeneity among studies (I 2 = 71%; P = .008), a random-effects model was employed for the meta-analysis. The meta-analysis revealed no statistically significant difference between exercise therapy and the control group (SMD, 0.34 [95% CI, −0.36 to 1.04]; P = .345).

Forest plot of peak hip flexion angle. EG, experimental group; IV, inverse variance; Std, standardized.
Knee Extension Moment
Figure 5 presents the meta-analysis results for the knee extension moment. This outcome measure comprised 11 pairwise comparisons. A random-effects model was utilized for the meta-analysis because of moderate heterogeneity among studies (I 2 = 52%; P = .02). Overall, no significant difference was detected between exercise therapy and the control group (SMD, 0.01 [95% CI, −0.33 to 0.35]; P = .95). Subgroup analysis results indicated no significant differences between exercise therapy and the control group in walking, landing, and running tasks.

Forest plot of knee extension moment. IV, inverse variance; Std, standardized.
Knee Valgus Moment
Five studies reported outcomes on knee valgus moment, with low heterogeneity in the literature (I 2 = 0.0%; P = .46). A fixed-effect model was employed for analysis. Overall, no significant difference was found between exercise therapy and the control group (SMD, −0.32 [95% CI, −0.81 to 0.16]; P = .19). Subgroup analysis results showed no significant differences between exercise therapy and the control group in gait, landing, and running tasks (Figure 6).

Forest plot of knee abduction moment. IV, inverse variance; Std, standardized.
Hip Extension Moment
Figure 7 illustrates the results of the meta-analysis on hip extension moment. This outcome measure included 9 pairwise comparisons. Given the low heterogeneity among studies (I 2 = 37%; P = .14), a fixed-effect model was employed for the meta-analysis. Exercise therapy significantly improved hip extension moment (SMD, 0.39 [95% CI, 0.02 to 0.76]; P = .004). Subgroup analysis revealed that exercise therapy significantly improved hip extension moment during walking tasks (SMD, 0.62 [95% CI, 0.27 to 0.97]; P < .001). However, no significant differences were observed between the exercise therapy and control groups in landing or running tasks.
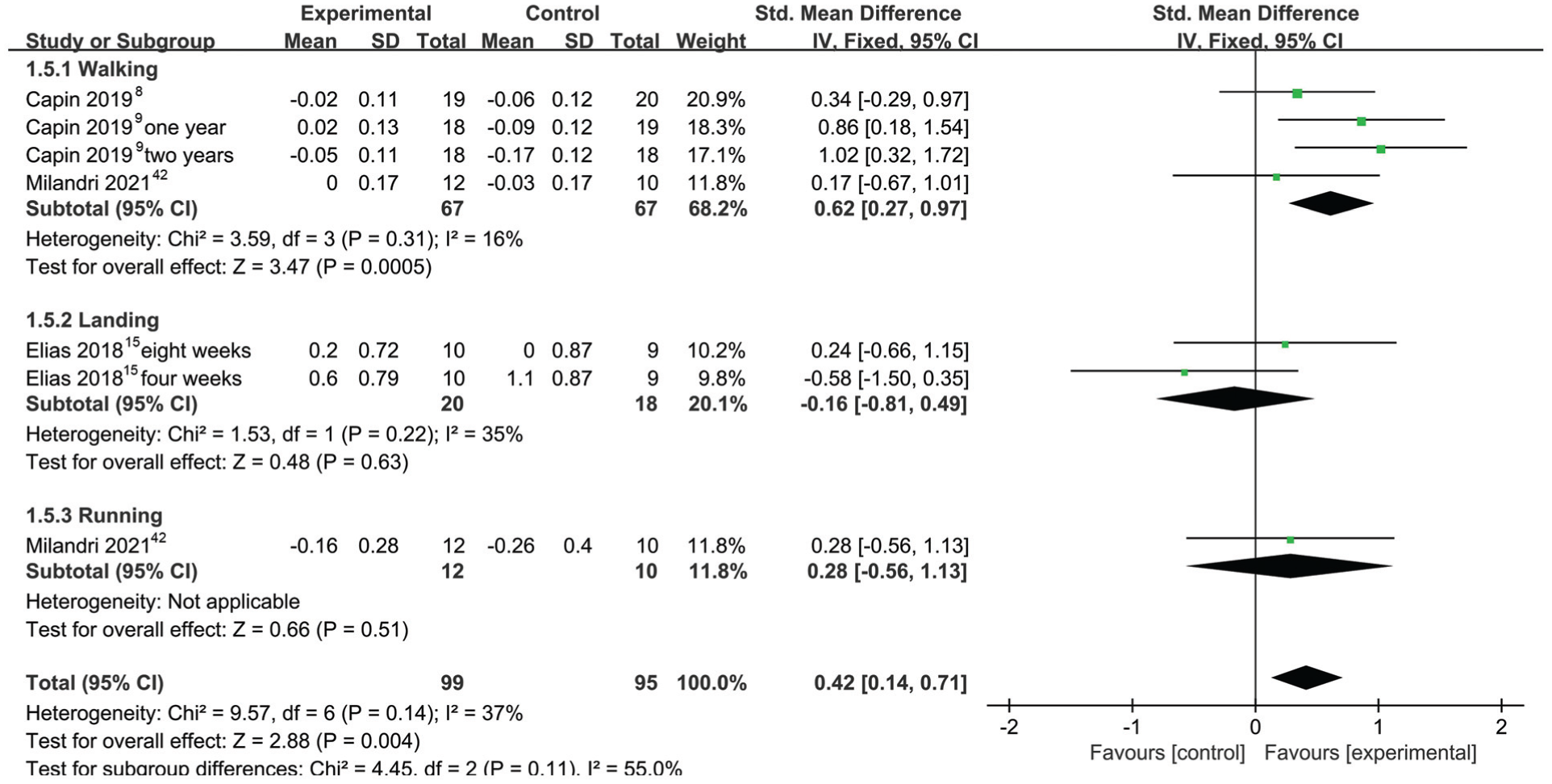
Forest plot of hip extension moment. IV, inverse variance; Std, standardized.
Vertical Ground-Reaction Force
Four studies reported outcomes for VGRF, with substantial heterogeneity among them (I 2 = 83%; P < .001). A random-effects model was employed for analysis. Overall, exercise therapy showed no significant differences compared with the control group (SMD, 0.36 [95% CI, −1.33 to 0.61]; P = .47). Subgroup analysis results revealed that exercise therapy significantly increased VGRF during walking tasks (SMD, 1.15 [95% CI, 0.29 to 2.01]; P = .009) but reduced VGRF during landing tasks (SMD, −0.83 [95% CI, −1.28 to −0.37]; P < .001) (Figure 8).

Forest plot of vertical ground-reaction force. EG, experimental group; IV, inverse variance; Std, standardized.
Sensitivity Analysis and Publication Bias
A sensitivity analysis was conducted across 7 outcome measures, sequentially excluding individual studies to further explore the sources of heterogeneity. Except for the peak flexion angle of the hip joint and the VGRF, the overall effect size remained unchanged, indicating that the meta-analysis results were relatively stable. The funnel plots exhibit a roughly symmetrical distribution (Appendix Figures S3 and S4).
GRADE Assessment
According to the GRADE system, the certainty of evidence ranged from very low to moderate. This was largely due to the high risk of bias in the included studies, inconsistency, and imprecision (Appendix Table S5).
Meta-regression
No significant effect on knee extension moment was found for any covariates. The improvement in peak knee flexion angle was related to the mean age (β = 0.18 [95% CI, 0.07 to 0.29]) but not to other covariates (Appendix Table S6).
Discussion
The major findings of our review demonstrated that exercise therapy significantly increased the peak knee flexion angle and the hip extension moment, while reducing the peak knee valgus angle, compared with the control group. Exercise therapy exhibited task-dependent modulation of VGRF but showed no significant effects on hip flexion angle, knee extension moment, or knee valgus moment.
Our study’s results suggest that exercise therapy significantly increased the peak knee flexion angle after ACLR. Athletes who met return-to-sport criteria after ACLR exhibited smaller peak knee flexion angles during dynamic tasks compared with healthy controls.10,11,34 Small knee flexion angles are associated with great shear forces, valgus moments, internal rotation moments, and VGRF in the knee joint, thereby increasing the risk of ACL reinjury.6,56,68 Alterations in quadriceps femoris activation 36 or a reduction in quadriceps femoris strength62,67 resulted in decreased ability to flex the knee joint during high-demand tasks, such as jumping. Ward et al 63 reported a moderate correlation between quadriceps femoris strength and peak knee flexion angle during landing after ACLR. Exercise therapy can effectively improve quadriceps femoris strength in patients after ACLR compared with non-exercise therapy.24,35 Therefore, we may speculate that improvement in peak knee flexion angle through exercise therapy might be mediated by enhanced quadriceps femoris strength.
The findings of our study indicate that exercise therapy significantly reduces the knee valgus angle. An increased knee valgus angle can generate excessive valgus stress on the knee joint in the coronal plane. 46 When this stress co-occurs with anterior tibial translation in the sagittal plane and axial rotation, it significantly increases ACL tensile load and injury risk. 59 Melick et al 18 reported that compared with healthy individuals, patients who underwent ACLR demonstrated greater knee valgus angles in the surgical limb during the single-leg vertical jump landing phase at 2 to 9 years after surgery, indicating persistent abnormal landing patterns in the long term. Our finding suggests that systematic training can improve movement patterns after ACLR to a certain extent. Our research highlights the positive role of exercise therapy in reducing the risk of ACL reinjury. Furthermore, a reduced knee valgus angle decreases the coronal plane displacement of the center of gravity and maintains the ankle joint in a more “neutral” position rather than inversion, which may help mitigate the risk of ankle sprain.17,69 Unfortunately, few studies have reported on coronal plane biomechanics of the ankle joint, and this inference requires further confirmation in future investigations.
Our meta-analysis showed that exercise therapy can significantly improve hip joint moments after ACLR. After ACLR, athletes often exhibit lower knee joint moments and higher hip joint moments than healthy athletes. 34 As a protective measure to develop secondary injuries, athletes after ACLR attempt to unload the knee and transfer the load to the hip. 34 Paradoxically, this avoidance strategy may inhibit stimulation of normal cartilage and increase the long-term risk of osteoarthritis in the operated knee. 44 Our result potentially suggests that while existing exercise therapy has positive effects on hip joint kinetic characteristics, it may not help patients after ACLR establish ideal loading patterns or sufficiently reduce their fear of reinjury. Therefore, intervention strategies should not only focus on single-joint levels but also integrate the overall motor function of the lower limb musculoskeletal system. Personalized rehabilitation programs should be implemented to facilitate the gradual resumption of physiological loading on the surgical-side knee joint and reduce kinesiophobia after ACLR during high-demand tasks.
Our meta-analysis demonstrated that exercise therapy significantly increased VGRF during walking tasks but decreased VGRF during landing tasks. We propose that differences in testing tasks may sufficiently explain inconsistent outcomes. Increased VGRF during landing tasks has been identified as a risk factor for noncontact ACL injuries.39,51 The VGRF in the surgical limb after ACLR was significantly lower than that in the contralateral limb and the healthy control group.45,55 This finding may be attributed to psychological confidence in the surgical limb after ACLR, leading to unloading of the surgical limb during high-demand dynamic tasks and transferring the load to the contralateral limb.45,55 Existing evidence suggests that knee joint biomechanical abnormalities observed in low-demand activities after ACLR do not necessarily persist during high-demand physical activities.27,32 We posit that exercise therapy may help correct loading patterns after ACLR during low-demand activities (eg, gait) but demonstrates no significant effects on high-demand tasks (eg, landing). Another plausible explanation is that the increased knee flexion angle during landing tasks enhances the potential for VGRF absorption, thereby reducing VGRF.
The results revealed that exercise therapy failed to improve kinetic characteristics in either the sagittal or coronal planes of the knee joint. In healthy populations, exercise therapy is an effective method for improving muscle strength and biomechanical characteristics.12,41,49 Therefore, the pathological characteristics after ACLR may account for the observed discrepancies. Joint moment reflects the muscle strength around the joint, with the knee extension moment primarily associated with quadriceps femoris strength and activation. 58 Quadriceps activation is further modulated by the central nervous system. Emerging evidence indicates that individuals after ACLR exhibit heightened excitability in spinal reflex pathways alongside reduced excitability in corticospinal pathways. These alterations occur concomitantly with diminished quadriceps strength and impaired voluntary activation.52,53 Based on our findings, we postulate that current exercise therapy protocols may fail to induce beneficial neuroplasticity and substantially improve knee joint kinetic characteristics, which may be attributed to their relatively short intervention duration (4-8 weeks) and nonspecific training protocols. Our findings are based solely on phenomena observed in the limited number of clinical trials currently available; thus, these hypotheses still require detailed investigation. Furthermore, we recommend incorporating additional components targeting alterations in neural excitability into existing exercise therapy protocols to restore deficits in knee joint kinetic characteristics after ACLR.
Comparison With Other Studies
To our knowledge, this study is the first systematic review that evaluated the effects of exercise therapy on biomechanical characteristics in patients after ACLR. Previous research primarily focused on investigating the effect of neuromuscular training on ACL injury risk. For healthy populations, training interventions can improve landing biomechanics by altering lower limb flexion, adduction, and rotation angles and moments, as well as landing VGRF, thereby reducing ACL load and injury risk.12,41,49 These multimodal injury-prevention programs can reduce injury risk by 45% to 67% among healthy athletes.13,64 However, no studies have systematically evaluated whether exercise therapy can improve biomechanics and reduce the risk of reinjury after ACLR. Exercise therapy can significantly increase peak knee flexion angle and hip extension moment while reducing peak knee valgus angle. An enhanced understanding of the biomechanical effects of various exercise therapies after ACLR facilitates the refinement and development of effective reinjury intervention measures. This study emphasizes the importance of developing additional intervention strategies targeting biomechanical deficits after ACLR.
Clinical Implications
Our systematic review indicates that exercise therapy demonstrates partial benefits in improving biomechanical characteristics of patients after ACLR, and current exercise therapy protocols fail to fully restore biomechanical deficits. This finding substantiates the perspective that extended recovery periods are required after ACLR1,25 and/or that task-specific training is needed to restore movement symmetry.47,48 Clinical guidelines recommend that knee joint biomechanical deficits should be identified and addressed during rehabilitation to mitigate reinjury risks. 35 Growing evidence suggests that ACLR recovery is no longer considered to require 4 to 6 months, as once thought, but may instead necessitate 1 to 2 years or even longer.1,25 Even when participants meet stringent objective criteria, restoring biomechanical symmetry during gait and landing tasks takes a long time.1,25 Based on the findings of this study, targeted intervention measures may accelerate this process. By synthesizing existing literature on the biomechanical effects of exercise therapy after ACLR, we have taken the first step toward informing the development of new exercise therapy protocols.
This review does not negate the clinical importance of the included exercise components. Muscle strength, reactive capacity, and other deficits may contribute to biomechanical deficits requiring remediation after ACLR. Regardless of modality, structured exercise remains the cornerstone of postoperative rehabilitation, aiming to enhance muscle strength, proprioception, and neuromuscular control to optimize biomechanics and reduce the risk of reinjury. Moreover, the traditional model posits that ACL injury is a musculoskeletal disorder in which adaptive changes occur peripherally rather than at the cerebral level. However, emerging evidence demonstrates that central nervous system alterations persist after ACL injury, and long-term muscle strength deficits and functional impairments after surgery may lead to adaptive changes in the central nervous system.52, 53 Innovative central nervous system stimulation techniques may serve as a potential rehabilitative supplement to restore maladaptive changes.
Strengths and Limitations
First, to our knowledge, no article has systematically and comprehensively investigated the effect of exercise therapy on biomechanical characteristics after ACLR. Therefore, we extensively searched all databases for relevant studies and included all key endpoints in our analysis. Second, to exclude factors potentially influencing outcomes, we performed regression analysis on all results and conducted subgroup analysis based on testing tasks to enhance research precision. However, several limitations should be emphasized. The types of grafts in athletes after ACLR were not standardized, although current evidence indicates no significant differences in biomechanical outcomes between autologous hamstring tendon grafts and bone-patellar tendon-bone grafts.5,61 Variations in training protocols for intervention measures (eg, duration, frequency, training volume, and intensity), along with differences in effect sizes within groups, may contribute to an elevated type 1 error rate. Data collection methods (ie, 2D versus 3D motion capture systems) may have introduced heterogeneity into our findings. Despite these limitations, we observed significant positive effects of exercise therapy on biomechanical characteristics after ACLR.
Conclusion
Our review demonstrated that exercise therapy significantly improved peak knee flexion angle and hip extension moment while effectively reducing peak knee valgus angle compared with the control group. Furthermore, exercise therapy modulated VGRF in a task-dependent manner, whereas its effects on hip flexion angle, knee extension moment, and knee valgus moment remained nonsignificant and had negligible magnitudes. Additional research is warranted to investigate the efficacy of targeted long-term training interventions in comprehensively enhancing multiplanar kinetics and kinematics after ACLR.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251402986 – Supplemental material for Effect of Exercise Therapy on Lower Limb Biomechanical Characteristics in Individuals After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251402986 for Effect of Exercise Therapy on Lower Limb Biomechanical Characteristics in Individuals After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Randomized Controlled Trials by Peng Chen, Junfan Ye, Huiwu Zuo and Ling Wang in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted September 22, 2025; accepted October 19, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.