
Abstract
Background:
Female runners have a higher risk of stress fractures compared with their male counterparts. However, the literature about best practices for preventing stress fractures in female long-distance runners is lacking.
Purpose:
To identify which factors predict the risk of stress fractures within 6 months in highly trained female long-distance runners.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
We measured bone mineral densities (whole body and lumbar spine) and body composition using dual-energy X-ray absorptiometry (DXA) in 21 highly trained female long-distance runners aged 18 to 37 years who belonged to a women's track team. Participants were followed prospectively for 6 months. Stress fractures were confirmed with bone scan, magnetic resonance imaging, and/or computed tomography findings. We employed univariate logistic regression and stepwise multivariate logistic regression, along with receiver operating characteristic curves, to examine the ability of bone mass and body composition parameters, alone or in combination, to predict the occurrence of a stress fracture.
Results:
We performed 118 DXA measurements. Stress fractures (4 sacral, 3 tibial, 3 calcaneal, 2 pubic, 2 femoral neck, 1 rib, 1 cuboid, and 1 metatarsal) occurred in 9 runners within 6 months. Bone mineral densities (% of young adult mean [YAM]; whole body: odds ratio [OR], 0.923; lumbar spine: OR, 0.914), total bone mineral content (BMC) (OR, 0.019), lean body mass (OR, 0.807), and percentage total BMC relative to total body mass (OR, 0.197) were significantly associated with a stress fracture developing. The multivariate analysis showed that bone mineral density of the lumbar spine alone was the strongest predictive factor (OR, 0.914 [95% CI, 0.853-0.963]). A lumbar spine bone mineral density <81.1% of the YAM predicted a stress fracture within 6 months, with 88% sensitivity and 74% specificity (area under the curve, 0.818).
Conclusion:
Our study demonstrated that highly trained female long-distance runners with lumbar spine bone mineral density <81.1% are at increased risk of a stress fracture within 6 months and should reduce their high-impact sports activities to avoid developing a stress fracture. The present study may provide meaningful information, suggesting that DXA measurements could be a useful screening tool in routine medical examinations to predict stress fractures in female long-distance runners, which may assist preventive programs or protocols.
A stress fracture is a sports-related overuse injury common among young competitive athletes, especially women, and can significantly interfere with training and competition.3,17 Patients with high-risk stress fractures take several months to return to full-sport participation, and some experience significant morbidity;11,12 therefore, prevention is preferable to even the most effective treatment. It may be possible to implement measures to prevent stress fractures from developing if risk factors are identified. 7
Low bone density,1,2 soft tissue composition,1,8,21 menstrual disturbances, 21 dietary insufficiency,8,21 biomechanical variants, 1 and excessive training 21 have been proposed as potential risk factors for stress fractures in female athletes. However, a recent review on the epidemiology of stress fractures in athletes suggested that few broad conclusions could be drawn because populations were heterogeneous and data collection methods varied. 19 Because risk factors may not be the same for all athletes, a study can provide useful information for one particular sport. Wright et al 22 systematically reviewed studies on risk factors associated with increased risk of lower extremity stress fractures in runners and concluded that only the factors history of stress fracture and female sex were strongly supported by data.
One prospective study identified risk factors for stress fractures in female long-distance runners, with a mean of 1.85 years after baseline evaluation. 8 However, it is considered impractical to limit the physical activities of long-distance runners for such extended periods, especially at a highly competitive level. Thus, identifying predictive risk factors for stress fractures within a relatively short period in female long-distance runners is useful. However, no studies have focused on identifying predictive risk factors for stress fractures within relatively short periods (eg, ≤6 months). In this study, we aimed to identify predictive risk factors and examine their ability to predict the likelihood of a stress fracture within 6 months in highly trained female long-distance runners. We hypothesized that the bone mineral density (BMD) of the lumbar spine would be a better predictor of stress fracture risk, as the lumbar spine is particularly sensitive to changes in bone health in endurance runners.6,9
Methods
Study Population and Design
We conducted a longitudinal, prospective, case-cohort study with 21 women who belonged to a single corporate women's track team. All women were Asian long-distance runners aged between 18 and 37 years. According to the definition by McKay et al, 13 all participants were classified as highly trained athletes competing at the national level, except for 1 runner who competed at the elite/international level. Between 2015 and 2020, we evaluated BMD and body composition for each individual using dual-energy X-ray absorptiometry (DXA) in May and November of each year, unless the individual had not run ≥300 km during the month before the DXA measurement day. Certain observation periods were excluded due to injuries, including stress fractures. Some runners joined or left the team during the study period. Consequently, the present study included 118 observation periods from 21 runners. The study was approved by the Institutional Review Board of Hokkaido University Hospital (approval number: 011-0178), and informed consent was obtained from all participants.
Bone Density and Body Composition Measurements
Using DXA equipment (Discovery A, Hologic, Inc), we separately measured BMDs of the lumbar spine (L1–4) and the whole body. To ensure measurement reliability, calibration using a phantom was performed at least once a week. We calculated each value as a percentage of the young adult mean (YAM) for the Asian female population. Diagnostic criteria indicate that the BMD of the lumbar spine is normal if the BMD is ≥80% of YAM; osteopenia is diagnosed if osteopenia at 70% to <80% YAM, and osteoporosis at <70% YAM. 20 We used the same equipment to determine body composition measures—total bone mineral content (BMC), body fat, and lean body mass—and also calculated each measure relative to total body mass (% BMC, % body fat, and % lean body mass, respectively). We used the same scanner and software version for all measurements, and at each session we measured body weight and height using an electronic scale (DP-7101PW, Yamato Scale Co) and an electronic stadiometer (SK-200, Shinwa Seiko Co), respectively. Body mass index (BMI) was calculated from these measurements.
Diagnosis of Stress Fractures
A team athletic trainer monitored participants for 6 months after each measurement and reported any possible stress fractures to us immediately. An individual with a possible stress fracture visited our hospital for physical examination by a single team physician (H.T.) and underwent a bone scan, magnetic resonance imaging (MRI), computed tomography, or a combination of these. We defined stress fractures as the presence of bone marrow edema or a fracture line on MRI. Therefore, in this study, cases of stress response with only periosteal reaction, such as shin splints, were excluded from the stress fracture group. All stress fractures were confirmed with radiologists’ reports. A team manager also emailed participants periodically to ask if any suspected stress fractures had occurred. No additional stress fractures were reported.
Statistical Analysis
All statistical analyses were performed using JMP Pro Version 15.2.0 (SAS Institute Inc). Means and standard deviations are presented for continuous variables, and absolute and relative frequencies are presented for categorical variables. We used Student t tests or chi-square tests to compare the characteristics of women who developed stress fractures with those who did not. P < .05 was considered significant.
To identify candidate predictor variables for stress fractures within 6 months, we used univariate logistic regression. To identify predictors of stress fracture development in the 6 months after a DXA measurement, we used stepwise multivariate logistic regression. Variables with P < .1 in the univariate logistic regression analysis were included in the stepwise multivariate regression model. To avoid multicollinearity, we calculated Pearson correlation coefficients for pairs of candidate variables, and if a value was ≥0.90, we excluded the variable with the largest Akaike Information Criterion (AIC) in a separate regression analysis. Predictors for the final regression model were determined by backward stepwise regression based on the minimum AIC. Odds ratios (ORs) and corresponding 95% CIs in all logistic regression analyses are reported. We subsequently performed receiver operating characteristic analysis to calculate the area under the curve (AUC) and to identify a cutoff value based on sensitivity and specificity. The AUC is an effective measure of the inherent validity of diagnostic value. An AUC of <0.5 means the test is noninformative. Values 0.5 to 0.7 are considered poor, 0.7 to 0.79 are considered fair, 0.8 to 0.89 are considered good, and >0.9 are considered excellent. 23
Results
Comparison Between Runners Who Developed and Did Not Develop Stress Fractures Within 6 Months
We included 21 female runners in our analysis. Overall, over the 6 months, we had 118 monitoring episodes and identified 17 new stress fractures in 9 runners, along with 101 episodes without stress fractures. The 17 stress fractures were located as follows: 4 sacral, 3 tibial, 3 calcaneal, 2 pubic, 2 femoral neck, 1 rib, 1 cuboid, and 1 metatarsal. There was no significant difference in age, height, body weight, or BMI between runners who developed stress fractures and those who did not (Table 1). Runners who developed stress fractures had significantly lower whole body and lumbar spine BMDs than those who did not (both, P < .001). Osteopenia was diagnosed significantly more frequently in those who developed stress fractures than in those who did not (P < .001) (Table 2). Body composition, total BMC, lean body mass, and % BMC were significantly lower in runners who developed stress fractures than in those who did not (total BMC, P < .001; lean body mass, P = .010; % BMC, P < .001) (Table 3).
Demographic Characteristics of Patients Who Developed Stress Fractures Within 6 Months Compared With Those Who Did Not a

Data are presented as mean (SD). BMI, body mass index.
Six-month observation periods for 21 runners.
Bone Mineral Density Characteristics of Patients Who Developed Stress Fractures Within 6 Months Compared With Those Who Did Not a

Data are presented as mean (SD). Bold P values indicate statistical significance. BMD, bone mineral density; YAM, young adult mean.
Six-month observation periods for 21 runners.
Body Composition Characteristics of Patients Who Developed Stress Fractures Within 6 Months Compared With Those Who Did Not a

Data are presented as mean (SD). Bold P values indicate statistical significance. BMC, bone mineral content.
Six-month observation periods for 21 runners.
Predictive Risk Factors for Stress Fracture Within 6 Months
We identified single factors, from univariate logistic regression (Table 4), that were significantly associated with stress fracture occurrence within 6 months: BMD of the whole body (P = .020), BMD of the lumbar spine (P = .004), total BMC (P = .002), lean body mass (P = .029), and % BMC P = .021). We failed to detect a significant association between body weight and the development of stress fractures within 6 months (P = .074).
Univariate Logistic Regression Results for Risk Factors Associated With Stress Fractures a

Bold P values indicate statistical significance. AIC, Akaike Information Criterion; BMC, bone mineral content; BMD, bone mineral density; BMI, body mass index; OR, odds ratio; YAM, young adult mean.
Of 6 variables with P < .1 in the univariate regression analysis, body weight and whole-body BMD were excluded from the multivariate analysis to avoid multicollinearity. We found strong correlations (Pearson coefficient ≥0.90) between body weight and lean mass, and between whole-body BMD and total BMC or % BMC (Table 5). Also, the AIC values for body weight and whole-body BMD were large (Table 4). BMD of the lumbar spine, total BMC, lean body mass, and % BMC were included in stepwise multivariate logistic regression, which identified BMD of the lumbar spine (% YAM) alone as the best predictor (OR, 0.914 [95% CI, 0.853, 0.963]). The AUC was good (AUC, 0.818), and the optimal cut-off value for BMD of the lumbar spine was 81.1% YAM, with a sensitivity of 88% and a specificity of 74% for predicting stress fracture occurrence within 6 months (Figure 1).
Pearson Correlation Coefficients for Pairs of Candidate Variables a
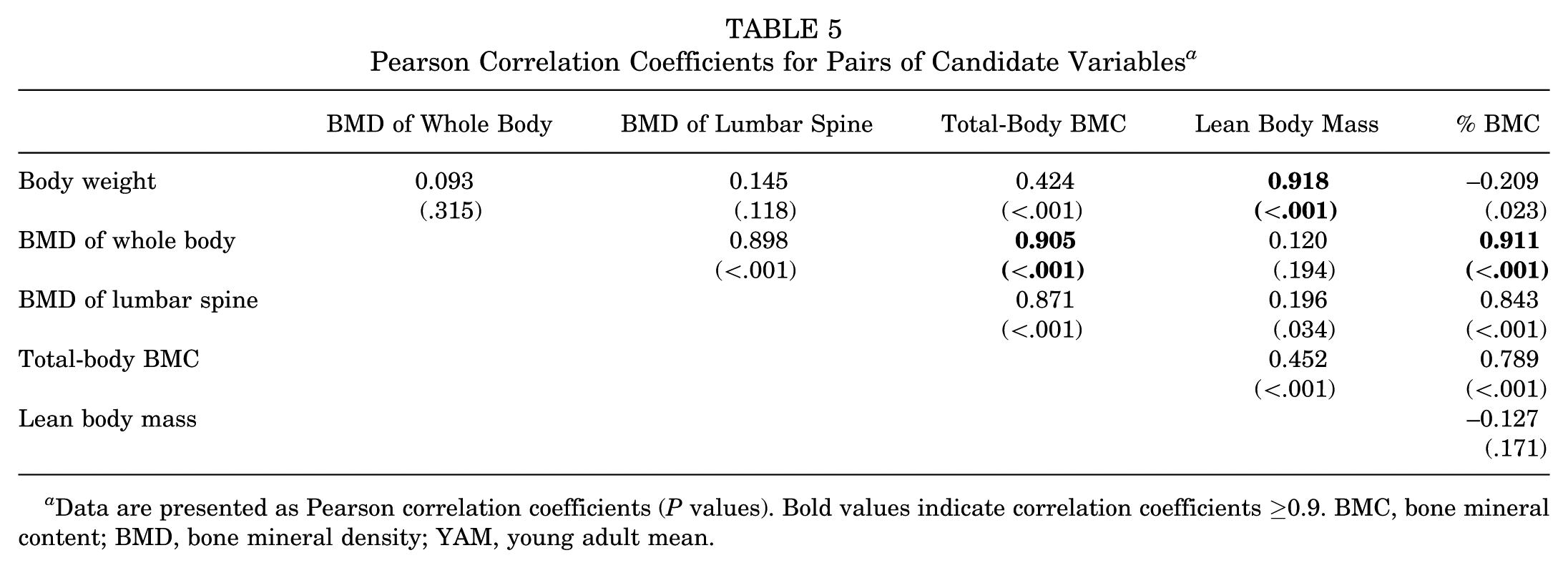
Data are presented as Pearson correlation coefficients (P values). Bold values indicate correlation coefficients ≥0.9. BMC, bone mineral content; BMD, bone mineral density; YAM, young adult mean.

ROCs for the model with lumbar spine bone mineral density (% YAM) as a predictor for the development of a stress fracture within 6 months. The AUC was 0.818 (good). A lumbar spine BMD <81.1% YAM was 88% sensitive and 74% specific (white circle) for predicting a stress fracture within the subsequent 6 months. AUC, area under the curve; BMD, bone mineral density; ROC, receiver operating characteristic; YAM, young adult mean.
Discussion
The major findings of our study demonstrated that low BMD of the lumbar spine alone was the best predictor for a highly trained female long-distance runner developing a stress fracture within 6 months after DXA measurement, and the optimal cutoff value was 81.1% YAM, with a sensitivity of 88% and a specificity of 74%. These results suggest that BMD is meaningful information for preventing stress fractures from developing in female long-distance runners by identifying highly trained female long-distance runners likely to develop stress fractures within 6 months.
Although a paper on a 12-month prospective study of 53 track-and-field athletes previously reported that athletes who sustained stress fractures had significantly lower total BMC and lumbar spine BMD, 1 the relationship between low BMD, as an isolated risk factor, and stress fractures in highly trained long-distance runners remains unclear. Our study included Asian national-class long-distance runners from a single corporate women's track team; therefore, the study population was considered relatively homogeneous—they trained daily at similar intensities over similar distances on the same course, ate the same meals, and lived in the same dormitory. We evaluated BMD and body composition for each runner using the same equipment on the same days in May and November, during the official track event and road race seasons, respectively. In addition, stress fractures were diagnosed by a single team physician (H.T.) at a single institute. Our use of these uniform methods may have reduced the effects of interindividual variance on risk factors and facilitated the identification of predictors.
Kelsey et al 8 identified total BMC as a risk factor for stress fractures among female distance runners aged 18 to 26 years using multivariate analysis, but they did not evaluate lumbar spine BMD or determine the optimal cutoff value of their model. We found that whole-body BMD, total BMC, and % BMC were significantly associated with the development of stress fractures within 6 months among highly trained long-distance runners, although the predictive abilities of these factors for stress fracture development were lower than that of lumbar spine BMD. Whole-body BMD and BMDs of the lower extremities are considered to be highly dependent on the loading characteristics of sports compared with lumbar spine BMD. 5 Lower extremity BMD in endurance runners is higher than that in nonathletes, whereas lumbar spine BMD is comparable with or even lower than that of nonathletes.6,9 We found that the mean whole-body BMD was higher than the YAM value even in those who developed stress fractures. It is possible that the positive effects of mechanical loading on whole-body BMD weaken its predictive ability compared with that of lumbar spine BMD.
Kelsey et al 8 also found that lean mass, but not body weight or BMI, is a risk factor for stress fracture among female distance runners aged 18 to 26 years, which is consistent with our findings. However, Tenforde et al 21 reported that body weight and BMI are risk factors for stress fractures in adolescent runners; the BMI of those who developed stress fractures was significantly lower than that of those who did not (18.7 vs 20 kg/m2). In our study, the BMIs of runners who developed stress fractures and those who did not were 17.6 kg/m2 and 18.2 kg/m2, respectively, with no significant difference between the groups. Therefore, floor effects might diminish the influence of BMI (or body weight) on the risk of developing stress fractures. Moreover, the difference in study population ages might account for this difference in effects.
Our findings indicate that highly trained female long-distance runners with lumbar spine BMD (% YAM) <81.1% are at an increased risk of developing stress fractures within 6 months. A temporary reduction in high-impact training may be a feasible preventive strategy for runners identified as at risk. However, the optimal duration and intensity of such training modifications remain unclear and warrant further investigation to establish evidence-based recommendations. Moreover, BMD is influenced not only by mechanical loading but also by physiological factors such as low energy availability (ie, inappropriate nutritional intake) and hormonal status, including menstrual dysfunction.4,15 Because the lumbar spine is relatively less susceptible to the mechanical loads of running, it may better reflect the effect of these physiological factors on bone health than the lower extremities.6,9 While lumbar spine BMD is useful for predicting stress fracture risk, effective prevention and improvement of bone health require appropriate management of these associated factors.
It is important to acknowledge that BMD values can vary across DXA devices. Such variability may limit the generalizability of absolute threshold values in different settings. In the present study, however, BMD was normalized using YAM values derived from a reference Asian population measured with the same DXA device. The use of population- and device-specific reference standards (such as %YAM) allows for meaningful comparisons and enhances the potential applicability of the findings in other contexts. Therefore, we believe that our results provide useful insights for practitioners using various devices.
Limitations
Our study had some limitations. First, because all participants were Asian, further studies should clarify the optimal cutoff value for lumbar spine BMD for the prediction of stress fractures in other groups. It is well known that BMD varies widely across racial and ethnic groups. Asian women are reported to have lower BMDs than White women, 18 and African-Americans are reported to have higher BMD than White individuals.10,14 Second, we selected national-class long-distance runners who performed daily running training at similar intensities for similar distances on the same courses. A previous study reported that those who run more or are more competitive are at a greater risk of sustaining stress fractures. 21 We should investigate the effects of running distance on the predictive ability of lumbar spine BMD. Third, we did not investigate the menstrual status of female long-distance runners as a risk factor. Nose-Ogura et al 16 reported that secondary amenorrhea increases the risk for stress fractures 12.9-fold in teenage female athletes. There is a high possibility that secondary amenorrhea is a risk factor for predicting the development of stress fractures in female long-distance runners. Despite these limitations, the present study provides meaningful information suggesting a possible useful application of DXA measurements as a screening tool in routine medical examinations to predict stress fractures in female long-distance runners.
Conclusion
The present study indicates that lumbar spine BMD is a predictor of stress fracture development within 6 months, with 88% sensitivity and 74% specificity in highly trained female long-distance runners. Our results suggest that highly trained female long-distance runners with lumbar spine BMD (% YAM) <81.1% are at increased risk of stress fractures within 6 months and should reduce their high-impact sports activities to avoid developing a stress fracture. The present findings suggest that DXA-based BMD measurements may have practical value as a screening tool in routine medical checkups for female long-distance runners, and may support the development of effective preventive strategies.
Footnotes
Acknowledgements
The authors thank Makoto Oda, BS, from the Division of Medical Imaging and Technology, Hokkaido University Hospital, for his assistance with DXA measurements. Additionally, the authors would like to thank Saori Iwata, MS, from the Graduate School of Health Sciences, Hokkaido University, for her assistance with data acquisition.
Final revision submitted September 15, 2025; accepted October 8, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hokkaido University Hospital (approval number: 011-0178).