
Abstract
Background:
Medial meniscal ramp lesions (MMRLs) can occur in up to 28% of pediatric patients at the time of anterior cruciate ligament (ACL) reconstruction (ACLR). However, limited studies have examined the outcomes after combined MMRL repair and ACLR in this at-risk patient population.
Purpose:
To evaluate the mid-term clinical outcomes after MMRL repair and ACLR in pediatric and adolescent patients and investigate possible risk factors for a secondary medial meniscal surgery.
Study Design:
Case series, Level of evidence, 4.
Methods:
Patients <18 years old who underwent MMRL repair during primary ACLR between 2015 and 2022 at 5 institutions with a minimum of 2-year follow-up were included. MMRLs were defined as an arthroscopically diagnosed partial or complete peripheral vertical/longitudinal tear of the posterior horn of the medial meniscus at/or within 3 mm of the meniscocapsular junction that underwent repair at the time of ACLR. Postoperative outcome measures included subjective International Knee Documentation Committee (IKDC) scores, return to sport (RTS), patient satisfaction, complications, rate of secondary medial meniscal surgery, and other reoperations. Descriptive statistics were used to report the demographic characteristics, operative findings, and postoperative outcomes for the cohort. Risk factors were assessed for a secondary medial meniscal surgery.
Results:
A total of 54 patients who underwent MMRL repair during primary ACLR at a mean age of 16.1 years (range, 12.4-17.9 years) were included in this study. Most patients reported a sports-related injury (82%), with 52% occuring during American football or basketball participation. At the time of surgery, 50% of patients demonstrated a high-grade pivot-shift (grade 2 or 3) examination under anesthesia, and 59% were arthroscopically diagnosed with a concomitant lateral meniscal tear. A total of 48 MMRL repairs (89%) were performed using all-inside techniques, while 5 (11%) were performed using inside-out techniques, and only 3 (6%) patients underwent a concomitant lateral extra-articular procedure. The mean follow-up was 60 months (range, 24-118 months). Postoperatively, 11 (20%) patients underwent a secondary medial meniscal surgery at a mean of 14 months (range, 6-28 months) after the index procedure. All 11 patients were initially treated with all-inside MMRL repairs, and were arthroscopically diagnosed with a tear involving or extending into the initial repair site at the time of revision surgery. The majority of retears were complex morphologies that occurred in the setting of an intact ACL graft and were the result of acute trauma within the first 2 postoperative years. Six (55%) were treated with a medial partial meniscectomy, while 5 (45%) underwent revision repair. No significant risk factors were associated with the presence of a secondary medial meniscal surgery. Overall, the cohort demonstrated a mean IKDC score of 88 ± 12 (range, 41-100), and for those who wished to RTS, an RTS rate of 76%.
Conclusion:
In this multicenter cohort of pediatric and adolescent patients who underwent MMRL repair during primary ACLR, with a mean follow-up of 5 years, the rate of secondary medial meniscal surgery was 20%. Overall, while the subjective patient-reported outcome measures were cautiously reassuring, larger studies are needed to better understand the modifiable risk factors for MMRL repair failure after ACLR in pediatric patients.
Keywords
Medial meniscal ramp lesions (MMRLs) of the posterior horn of the medial meniscus are peripheral longitudinal/vertical tears at or within 3 mm of the meniscocapsular junction.8,10,22,41 The biomechanical function of these meniscocapsular attachments is to prevent anterior tibial translation, making the ramp area predisposed to tear concomitantly in anterior cruciate ligament (ACL) tears.8,11,12,41 As such, MMRLs have been reported to occur concomitantly in 9% to 42% of adults undergoing an ACL reconstruction (ACLR).20,38,39 These meniscal tears have a predilection to be missed due to challenges with diagnosis on physical examination, magnetic resonance imaging (MRI), and standard anterior arthroscopic probing at the time of ACLR.2,17
In the setting of adult ACLR (age >18 years), the clinical evidence in favor of repairing MMRLs continues to evolve.9,14,31,38,42 Biomechanically, unrepaired MMRLs (in the setting of a reconstructed ACL) have been shown to increase residual anterior tibial translation, which is eliminated with MMRL repair. While long-term clinical data are still lacking, Tuphé et al reported that 21% of unrepaired stable MMRLs during ACLR progressed to medial meniscal bucket-handle tears at long-term follow-up. 42 Despite the potential risk of residual instability and long-term complications, the existing clinical outcomes on MMRL repair and ACLR are limited and primarily confined to adult patient populations.
Pediatric patients, commonly defined as those ≤18 years old, are considered to be the highest risk patient population for sustaining ACL tears, meniscal tears, and graft rupture after ACLR.4,5 While most of the current literature on MMRL repair and ACLR is derived from adults, a few observational studies have reported the presence of MMRLs in 13.2% to 28% of pediatric patients undergoing ACLR.2,17,28 However, relatively little is known about the clinical outcomes after MMRL repair and ACLR in these young patients who are at a higher risk for failure. Pediatric patients are clinically distinct from adults due to their increased ligament laxity, higher rates of participation in organized sports, unique challenges with rehabilitation, and an increased risk of reinjuries and revision surgeries.4,5 As such, this multicenter study aimed to evaluate the mid-term clinical outcomes after MMRL repair and ACLR in pediatric and adolescent patients and investigate possible risk factors for a secondary medial meniscal surgery.
Methods
Patient Selection and Identification
Institutional review board approvals and multicenter data sharing agreements were accepted and granted at the 5 study institutions (Yale School of Medicine, Hospital for Special Surgery, Texas Children's Hospital, Rush University Medical Center, and Twin Cities Orthopedics). Surgical records were queried using Current Procedural Terminology (CPT) codes for ACLR (29888) with meniscal repair (CPT 29882 and 29883) to identify all patients aged <18 years at the time of surgery who underwent concomitant MMRL repair during ACLR at 1 of the 5 study institutions between January 2015 and December 2022. Patient data were queried across 5 orthopaedic surgeons (1 board-certified pediatric and sports medicine fellowship–trained surgeon (P.D.F.); 1 board-certified pediatric fellowship–trained surgeon (S.D.M.), and 3 board-certified sports medicine fellowship–trained surgeons (M.J.M., J.C., R.F.L.)), each from the 5 separate institutions.
All surgeons reported routinely performing a modified Gillquist maneuver and/or an accessory posteromedial portal during the study period to arthroscopically assess for the presence of MMRLs at the time of ACLR.1,13 Each operative note was independently reviewed by 2 reviewers (J.M. and J.Z.A.) to confirm sufficient documentation for meeting the definition for the presence of a MMRL. Based on an established arthroscopic definition in the literature, MMRLs were defined as arthroscopically diagnosed partial or complete peripheral vertical/longitudinal tears of the posterior horn of the medial meniscus at/or within 3 mm of the meniscocapsular junction at the time of ACLR.2,3 In cases of disagreement between reviewers on the definition of an MMRL, the senior author (R.F.L.) made the final decision to include or exclude the patient of interest. Arthroscopic images and further subclassification of the MMRLs were not assessed.
After identifying the initial cohort who underwent MMRL repair during ACLR, patients were excluded if they met any of the following criteria at the time of initial surgery: (1) concomitant periarticular fractures, not including bone bruises or subchondral insufficiency fractures; (2) complex medial meniscal tears or those extending into the meniscal body, anterior horn, or roots; (3) revision ACLR, as opposed to primary ACLR; (4) incomplete or ambiguous surgical documentation precluding confirmation of an MMRL; (5) congenital lower extremity abnormalities; (6) diagnosis of an ipsilateral discoid meniscus; (7) previous ipsilateral knee surgery or injury; (7) concomitant medial patellofemoral reconstruction, multiligament reconstruction or repair (medial collateral ligament, posterior cruciate ligament, and fibular [lateral], collateral ligament reconstruction, or complete posterolateral corner injury); (8) osteotomy; or (9) tibial eminence avulsion fracture.
For patients who satisfied the inclusion and exclusion criteria, the following variables were collected from reviewing the medical charts: (1) age at the time of surgery; (2) sex; (3) time from injury to ACLR/MMRL repair (categorized as acute <6 weeks, subacute ≥6 weeks to <12 weeks, and chronic ≥ 12 weeks);1,26 (4) body mass index (BMI); (5) BMI percentile according to sex and age; (6) obesity status (defined as ≥95th percentile for BMI for age and sex) 7 ; and (7) mechanism of injury (categorized as contact or noncontact).25,29 Skeletal maturity was classified as mature (closed physes) or immature (open physes) based on MRI. Physes were considered to be open if there was a band of high signal intensity on T2-weighted images in the expected location of the distal femoral physeal plate. 24 Lachman (grades 1-3) and pivot-shift grading (grades 1-3) were performed under anesthesia and recorded at the time of the index surgery. A high-grade pivot-shift was defined as patients who displayed a grade of ≥2.
Additional surgical findings at the time of MMRL repair and ACLR that were collected included the presence and surgical treatment of concomitant lateral meniscal tears, the type of ACLR graft, the MMRL repair technique, the number of sutures used for MMRL repair, and the presence of a concomitant lateral extra-articular procedure (LEAP).
Secondary Surgeries, Complications, and Patient-Reported Outcome Measures
All patients had a minimum of 2-year clinical follow-up. Final follow-up for each eligible patient was defined by the date (with a study end date of December 2024). Telephone interviews and electronic questionnaires were administered to obtain subjective postoperative International Knee Documentation Committee (IKDC) scores; return to sport (RTS), defined by returning to the same or higher level of sport after surgery; visual analog score for patient satisfaction (0 = worst, 10 = best); and information regarding any complications, reinjuries, or reoperations. Patients who were unable to be contacted to complete telephone interviews and electronic questionnaires, or who refused to participate, were considered lost to follow-up. The patient-acceptable symptom state for isolated ACLR in adolescent patients has been reported 23 to be an IKDC score of ≥80.5. While the present study presents a different injury pattern than those that undergo an isolated ACLR, the number of patients achieving this IKDC score threshold was reported for improved interpretation of the IKDC data. For the RTS calculation, patients who reported not participating in sports after surgery for reasons unrelated to their knee injury were excluded. 18 Patients who underwent ipsilateral secondary surgery during the study period were excluded from the subjective postoperative patient-reported outcome measure (PROM) analysis for the cohort.
The presence of any secondary surgeries during the postoperative period was assessed. In addition to reviewing the medical charts, patient interviews inquired about potential complications or additional revision surgeries that may have been performed at an outside institution or concomitantly with a secondary medial meniscal surgery. For patients who underwent a secondary medial meniscal surgery after the index procedure, the following variables were collected: time to secondary medial meniscal surgery (defined as the time between the index MMRL repair and ACLR and secondary medial meniscal surgery); arthroscopic description of the medial meniscal retear pattern; mechanism of reinjury; additional arthroscopic operative findings, including medial meniscal retear treatment (repair and/or partial medial meniscectomy); and additional concomitant procedures at the time of revision surgery. PROMs were reported only for patients who did not undergo a secondary surgery.9,38
Surgical Technique for Medial Meniscal Ramp Lesion Repair During Primary ACLR
For all 5 surgeons, the indication for performing an ACLR at the time of surgery included a complete ACL tear confirmed with increased laxity on physical examination, MRI, and diagnostic arthroscopy. ACLRs were performed with a mix of autograft techniques, including bone-patellar tendon-bone, quadriceps tendon, or semitendinosus/gracilis grafts, with or without physeal-sparing reconstruction techniques, based on skeletal maturity. The indications for performing a concomitant LEAP were not standardized and varied among the surgeons.
The indications for an MMRL repair during ACLR were not standardized among surgeons, but were commonly performed in the setting of a partial or complete MMRL deemed unstable with arthroscopic probing.2,3 Patients underwent all-inside or inside-out MMRL repairs performed according to previously described and biomechanically validated techniques in the literature and sugeon specific preference.9,15 All-inside repairs were most commonly performed through standard anterior arthroscopic portals using capsular-based, self-tensioning devices (Figure 1). 15

Arthroscopic images of a 13-year-old adolescent female's knee at the time of primary ACLR with (A) a concomitant MMRL showing the meniscocapsular separation diagnosed on arthroscopy using a modified Gillquist maneuver and (B) a subsequent mattress repair of the medial meniscal ramp lesion with an all-inside, capsular-based, self-tensioning device. ACLR, anterior cruciate ligament reconstruction; MFC, medial femoral condyle; MMRL, medial meniscal ramp lesion; PMC, posteromedial capsule.
For inside-out MMRL repairs, suture needles were passed in a vertical-mattress fashion, retrieved through an open posteromedial incision, and subsequently tied over the posteromedial capsule under direct arthroscopic visualization anteriorly (Figure 2).9,27

Arthroscopic images of an example of an inside-out MMRL repair technique. (A) Anterior view of an MMRL that was deemed unstable with arthroscopic probing. (B) MMRL in the posteromedial compartment from a modified Gilliquist or trans-notch view. (C) Reapproximation of the meniscocapsular attachment during suture placement through the posterior horn and posteromedial capsule. (D) Complete inside-out MMRL repair with double-row vertical mattress sutures. Image originally published in DePhillipo NN, Dornan GJ, Dekker TJ, Aman ZS, Engebretsen L, LaPrade RF. Clinical Characteristics and Outcomes After Primary ACL Reconstruction and Meniscus Ramp Repair. Orthop J Sports Med. 2020;8(4):2325967120912427. MMRL, medial meniscal ramp lesion
Postoperative Rehabilitation Protocol
Postoperative rehabilitation protocols varied across centers and allowed either partial or full weightbearing as tolerated, with a brace locked in extension and crutches recommended until a nonantalgic gait was achieved or for up to 6 weeks postoperatively. From weeks 2 to 6, most protocols permitted 0° to 90° of knee motion. By 6 weeks, all patients were allowed full weightbearing and unrestricted range of motion, without engaging in impact activities. At 12 weeks, the majority began straight-line running, with continued restrictions on pivoting and cutting. Sport-specific progression was initiated after successful completion of a functional assessment. RTS was typically permitted around 9 months after injury, once patients demonstrated symmetric strength, stability, and range of motion compared with the contralateral limb. In some cases, clearance for cutting and pivoting sports was delayed until approximately 12 months postoperatively.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics, surgical details, and clinical outcomes. Continuous variables are reported as means and standard deviations. Categorical variables are presented as counts and percentages. Because of the small sample size and low event frequency, formal hypothesis testing was limited. Exploratory bivariate analyses were performed using t tests or nonparametric equivalents for continuous variables, and the chi-square test or the Fisher exact test for categorical variables. Statistical significance was set as P≤ .05. Analyses were performed using Microsoft Excel with Real Statistics add-in (Microsoft Corp).
Results
Cohort Selection and Patient Eligibility
Overall, 72 patients <18 years who underwent concomitant MMRL repair and primary ACLR between 2015 and 2022 were identified. Of these 72 patients, 54 (75%) were included in the final analysis and cohort (Figure 3).
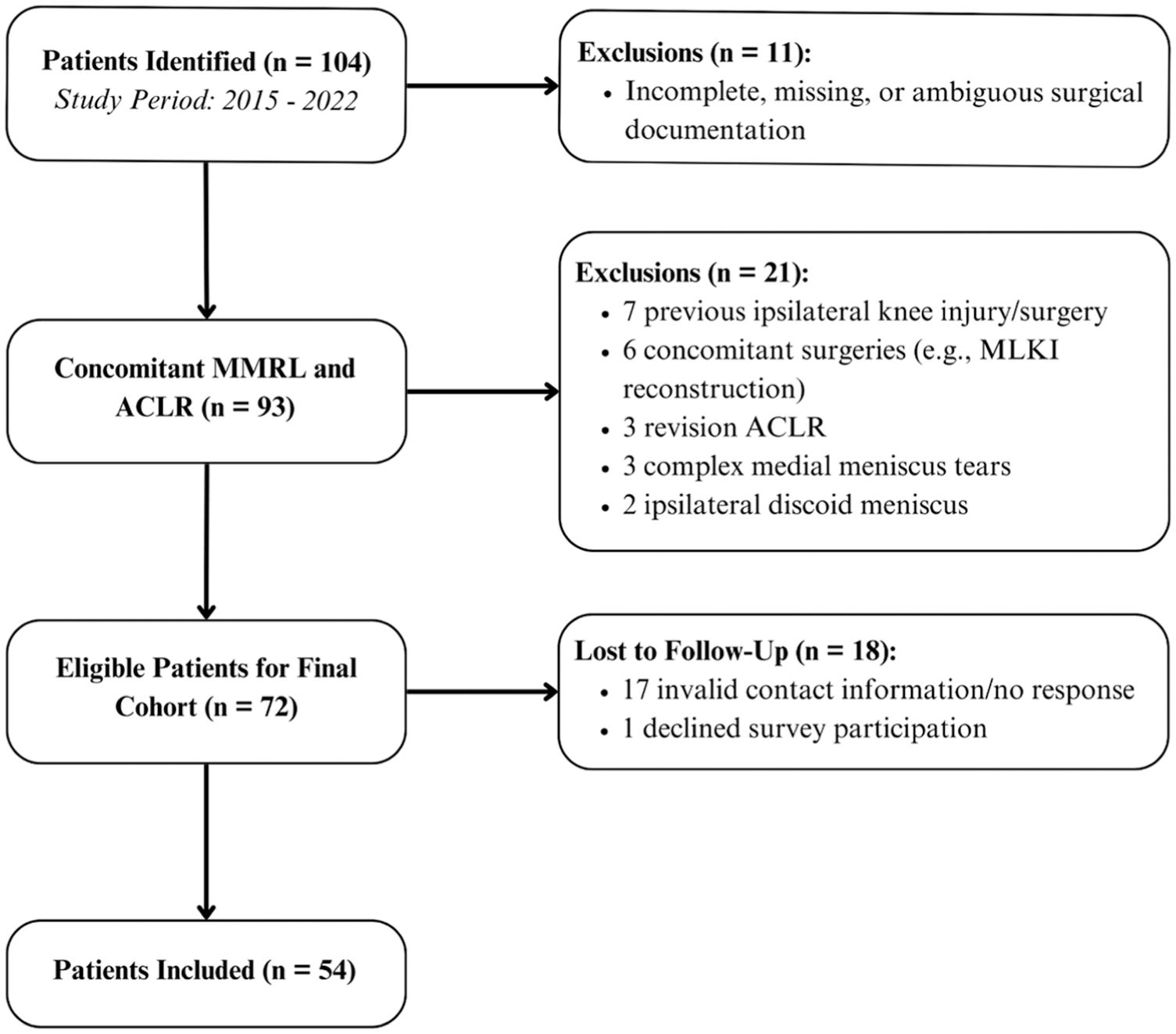
Study flow chart for the final cohort selection. ACLR, anterior cruciate ligament reconstruction; MLKI, multiligament knee reconstruction; MMRL, medial meniscal ramp lesion.
Patient characteristics for the cohort are summarized in Table 1.
Patient and Cohort Characteristics at the Time of MMRL Repair During Primary ACLR a (n = 54)

Data are presented as mean ± SD (range) or n (%). ACLR, anterior cruciate ligament reconstruction; BMI; body mass index; MMRL, medial meniscal ramp lesion.
During the index procedure, 27 (50%) demonstrated a high-grade pivot-shift examination under anesthesia (defined by grade ≥2), and 32 (59%) had a concomitant lateral meniscal tear diagnosed arthroscopically. A total of 48 MMRL repairs (89%) were performed using all-inside techniques, while 6 (11%) were inside-out. Overall, only 3 (6%) patients underwent a concomitant LEAP. Lastly, inside-out MMRL repairs used significantly more sutures, on average, than all-inside MMRL repairs (5 sutures per repair vs 3 sutures per repair; P < .001). Physical examination findings under anesthesia and operative details from the index surgery are summarized in Table 2.
Physical Examination Findings Under Anesthesia and Operative Findings at the Time of MMRL Repair During Primary ACLR a (n = 54)
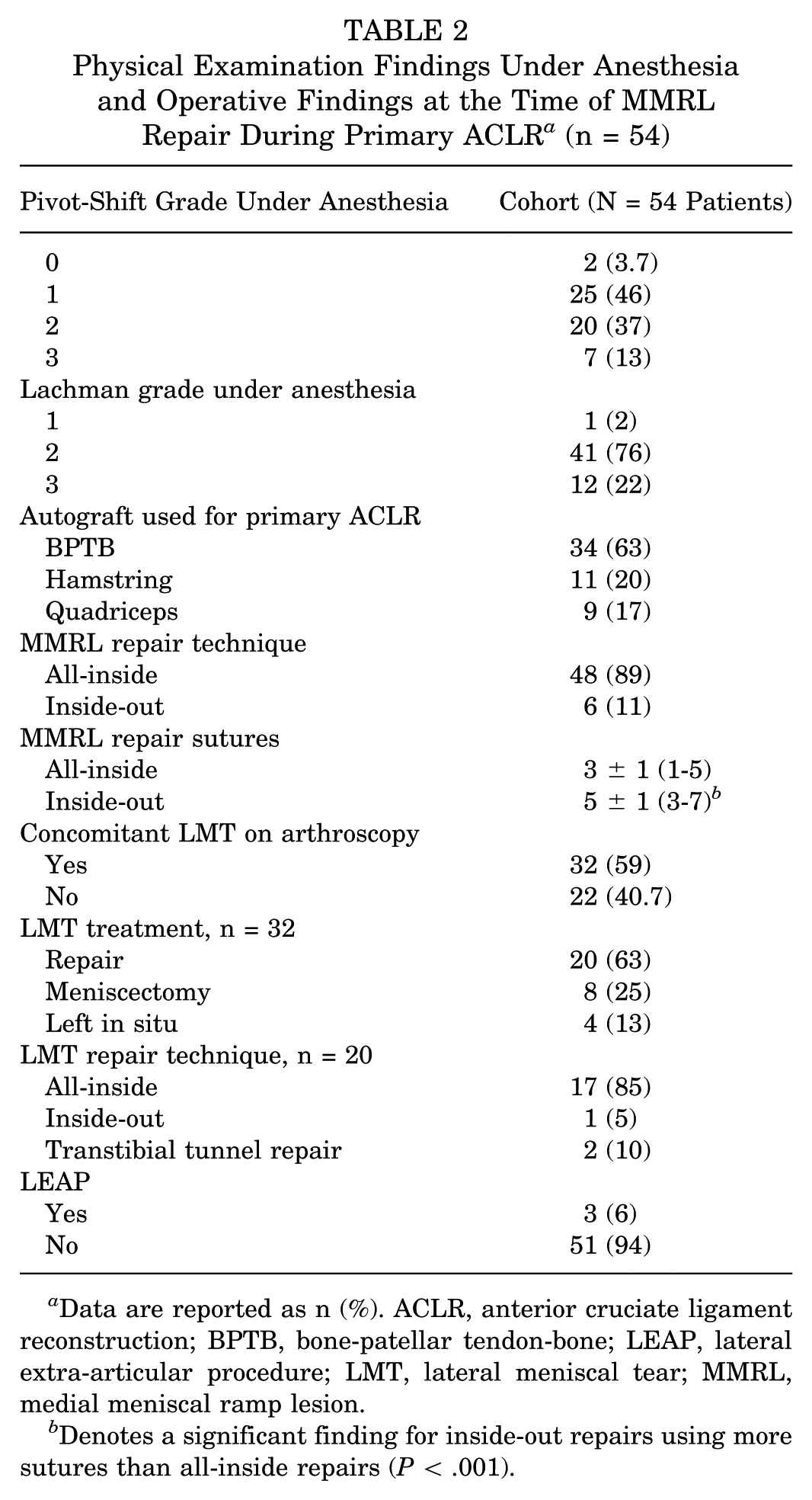
Data are reported as n (%). ACLR, anterior cruciate ligament reconstruction; BPTB, bone-patellar tendon-bone; LEAP, lateral extra-articular procedure; LMT, lateral meniscal tear; MMRL, medial meniscal ramp lesion.
Denotes a significant finding for inside-out repairs using more sutures than all-inside repairs (P < .001).
PROMs, Complications, and Revision Surgery
The mean follow-up of the cohort was 60 months (range, 24-118 months) after primary ACLR and MMRL repair. Overall, 11 (20%) patients underwent a secondary medial meniscal surgery during the follow-up period. Of the 43 patients who did not undergo secondary medial meniscal surgery, the mean subjective IKDC was 88 ± 12 (range, 41-100), with 35 of 43 patients (81%) achieving a score of ≥80.5. The median patient satisfaction score was 9 (interquartile range, 8-10). Of the 37 eligible patients for RTS analysis, 28 (76%) reported RTS at the same or higher level postoperatively. Overall, 4 patients experienced a contralateral ACL tear during the follow-up period.
Eleven patients (20%) underwent a secondary surgery for a medial meniscal retear at a mean of 14 months (range, 6-28 months) after the index procedure. Of these 11 patients, 7 (64%) underwent an isolated secondary medial meniscal surgery while 4 (36%) had an additional same-day concomitant revision procedure (2 patients underwent revision ACLR, 1 patient underwent lysis of adhesions for arthrofibrosis with a cyclops lesion, and 1 patient underwent revision lateral meniscal repair). Nine patients (82%) had an intact ACL graft on arthroscopic evaluation.
All of the medial meniscal retear patterns diagnosed arthroscopically at the time of revision surgery involved or extended into the initial MMRL repair site and included 6 complex radial oblique/flap tears at the body/posterior horn with extension into the previous repair site, 3 vertical/longitudinal tears (recurrent MMRLs) at the index repair site, and 2 complete medial meniscal bucket-handle tears. Overall, 6 (55%) retears (3 complex, 2 bucket-handle, and 1 vertical/longitudinal) were treated with a medial partial meniscectomy, while 5 (46%) (3 complex and 2 vertical/longitudinal retears) underwent revision medial meniscal repair.
All 11 patients with a MMRL repair failure were initially treated with all-inside MMRL repairs at the time of the index procedure; however, there was no significant difference when comparing the failure rates of all-inside versus inside-out MMRL repairs. The reported mechanisms of reinjury were as follows: acute trauma during physical activity or high school sports (n = 10; 91%) and persistent knee instability with no inciting event (n = 1; 9%). The bivariate analysis demonstrated no significant differences between patients who did and did not undergo a secondary medial meniscal surgery; therefore, a multivariable logistical regression was not performed (AppendixTables A1 and A2).
Discussion
In this multicenter cohort of pediatric and adolescent patients who underwent MMRL repair and primary ACLR, with a mean follow-up of 5 years, 20% underwent a secondary medial meniscal surgery for a retear that involved or extended into the initial MMRL repair site. Interestingly, these retears were predominately complex morphologies, most commonly occurred in the setting of an intact ACL graft, and were the result of acute traumatic reinjuries within the first 2 postoperative years. More than half of these young patients underwent a medial partial meniscectomy as opposed to revision repair. Additionally, the present study found no significant risk factors associated with the presence of a secondary medial meniscal surgery. Overall, while the subjective PROMs were cautiously reassuring, larger studies are needed to better understand the modifiable risk factors for MMRL repair failure after ACLR in pediatric patients.
A few studies in the adult literature have reported on the outcomes after MMRL repair and ACLR, with mean cohort ages ranging from 26 to 29 years at the time of surgery.9,14,31,38,42 Sonnery-Cottet et al 37 reported a 10.8% secondary medial meniscectomy rate in adults (defined as MMRL repair failure) at a mean follow-up of 46 months for all-inside posteromedial suture hook MMRL repairs, while Gousopoulos et al 16 reported a 15.6% failure rate at a mean follow-up of 8 years. Similarly, Tanel et al 38 reported a 21.9% secondary meniscectomy rate at 10-year follow-up in adults undergoing ACLR and all-inside MMRL repairs. 38 Compared with adult patients, meniscal repairs have been associated with a significantly higher failure rate in the pediatric and adolescent patient population.21,34 Shieh et al 34 studied revision meniscal surgery in children and adolescents and found that 18% of primary isolated meniscal repairs (excluding MMRLs) required revision surgery at a 40-month follow-up. Nearly all their failures were attributed to acute reinjury during physical activity within the first postoperative year. 34 Similarly, in our cohort of pediatric and adolescent patients treated with MMRL repair and ACLR, with a mean follow-up of 60 months, 20% underwent a secondary medial meniscal surgery for a reinjury that occurred from acute traumatic mechanisms during high school sports or physical activity within the first 2 postoperative years. However, the present cohort's MMRL repair failure rate appears to be on the higher end of the spectrum compared with those reported for adults, although further studies that directly compare the 2 populations are needed to confirm this.
In multiple adult studies throughout the literature, the presence of a secondary or revision medial meniscal surgery is a commonly used metric to define MMRL repair failure after ACLR.9,14,31,38,42 However, this definition may underestimate the true number of repair failures, as clinical symptoms and/or postoperative MRIs were not analyzed, and second-look arthroscopy was not performed on every patient to assess the healing status of the MMRL repair, particularly in asymptomatic patients. It is also unknown whether the repair failures in the present study were the result of an unrelated new tear that extended into the initial repair site or a failure of the actual MMRL repair that could have predisposed the patient to retearing their meniscus. As such, the term retear and the resultant rate of secondary medial meniscal surgery should be interpreted within the context of these study parameters. Also, pediatric patients with both MRI-proven retears and clinical symptoms who do not undergo revision surgery should be accounted for in future studies.
The treatment of medial meniscal reinjuries after MMRL repair and ACLR remains poorly understood, especially in pediatric and adolescent patients. The present study found that most of these patients had complex retears in the setting of an intact ACL graft. While speculative in nature, the possibility exists that trauma from the initial repair using all-inside devices that penetrate the meniscus could have predisposed a patient to retear in a complex manner. More than half underwent a partial medial meniscectomy rather than revision repair, primarily due to avascularity and poor tissue quality of the retear and remaining medial meniscus. In the setting of a failed MMRL repair, partial meniscectomy of the retear may significantly increase the risk of posttraumatic osteoarthritis, especially in younger patients.33,43 Alternatively, 45% were treated with a revision medial meniscal repair. If the tissue quality and retear pattern appear amenable, a revision repair may offer a better long-term prognosis than a partial meniscectomy. 6 However, larger and long-term clinical studies are necessary to confirm these findings, as the present study is limited to a small cohort with mid-term outcomes, where these potential consequences may not be evident.
The management of MMRLs remains elusive, especially in the pediatric population. Standardized systematic arthroscopic techniques, such as a modified Gillquist maneuver or posteromedial accessory portal, should be employed in every pediatric patient undergoing ACLR. 36 All surgeons were routinely performing a modified Gilliquist maneuver and/or accessory posteromedial portal on every patient undergoing ACLR during the entirety of the study period. 13 Furthermore, it is strongly recommended that unstable MMRLs be repaired during ACLR, which was the primary indication for repair in the present study.9,11,27,35 The present study did not include patients with MMRLs who were left untreated and deemed stable at the time of ACLR. In addition, MMRLs were not categorized into different subtypes, and the use of an existing classification system may help identify which subtypes carry a higher risk of failure in pediatric and adolescent patients. 40 Overall, the present study found that the mean IKDC score was 88, with 35 patients (81%) achieving a score of ≥80.5 and 28 (76%) returning to sport at the same or higher level postoperatively. These PROM scores closely align with those reported in the literature for isolated ACLR in pediatric and adolescent patients.19,30
Of the MMRL repairs performed in the present study, 89% were all-inside, while 11% were inside-out. Inside-out MMRL repair techniques, on average, used significantly more sutures per repair compared with all-inside techniques (5 vs 3 per repair; P < .001). However, no significant difference was found in failure rates when comparing the 2 repair techniques. Inside-out MMRL repair may offer flexibility with the placement and number of sutures, thereby creating a stronger repair. However, this technique requires an open posteromedial incision and is more technically challenging compared with all-inside techniques.9,27 Although not assessed in the present study, all-inside MMRL repairs may inadequately address the meniscotibial attachment that could contribute to repair failure.16,32 The vast majority of all-inside MMRL repairs in the present study were performed using anterior arthroscopic portals only. Similarly, large sample sizes are warranted to compare the clinical efficacy of different and modern-day MMRL repair techniques—including those through a posteromedial portal—as there is still no consensus on the optimal repair technique in high-risk pediatric patients.
The protective role of a LEAP in high-risk adolescents undergoing ACLR has gained much attention recently. 44 In the present study, only a small percentage (6%) underwent a concomitant LEAP at the time of MMRL repair and ACLR, likely due to the inclusion of a large number of patients treated before 2020. It is important to highlight that 50% of our cohort demonstrated a high-grade pivot shift examination at the time of the index procedure. However, the widespread adoption of LEAPs and present-day indications, such as a high-grade pivot-shift in an adolescent athlete, most likely differed from those during our study period. 3 Nevertheless, the added rotational stability afforded by an LEAP has been reported to be protective of MMRL repair failure in adults undergoing ACLR. 34 This is an important consideration for pediatric and adolescent patients with ACL tears and MMRLs, given that the majority of patients who underwent a secondary medial meniscal surgery in the present study had isolated and complex retears in the setting of an intact ACL graft. As such, the addition of a concomitant LEAP may have the potential to decrease the risk of MMRL repair failure in pediatric patients, and its protective role in this specific at-risk patient population still needs to be elucidated.
This multicenter study has several limitations that have not been mentioned—including its retrospective design and the lack of a control group for comparison. Eighteen patients (25%) were considered lost to follow-up and were unable to be contacted for telephone interviews and electronic questionnaires, which may have influenced both the reported failure and success rates. While assessing arthroscopic images could have enhanced the classification of MMRLs, digital storage of intraoperative images in the medical charts was not routinely practiced at every institution during our study period. Given the small number of patients who underwent a secondary medial meniscal surgery, our sample size was likely underpowered to detect any differences or risk factors between the 2 groups. Patients were treated by 1 of 5 sports medicine surgeons, each employing their preferred repair techniques, implants, and postoperative rehabilitation protocols that were not standardized across centers, potentially introducing selection bias. Only two of the surgeons were dedicated pediatric sports medicine surgeons, whose practices primarily consisted of this patient population, while the other 3 surgeons primarily treated adult patients. As such, the number of pediatric and adolescent patients contributed by each surgeon and institution varied greatly due to these inherent practice differences. However, this heterogeneity may increase the generalizability of our results. The study start period was chosen because patient contact information was routinely stored in the electronic medical charts beginning in 2015 at the majority of these institutions, which limited our ability to explore the longer-term outcomes associated with MMRL repairs in this population. Lastly, while the type of sport and participation may influence the survivorship of MMRL repairs after ACLR, the diversity of sports represented in this cohort limited our ability to conduct meaningful subgroup analysis.
Conclusion
In this multicenter cohort of pediatric and adolescent patients who underwent MMRL repair during primary ACLR, with a mean follow-up of 5 years, the rate of secondary medial meniscal surgery was 20%. Overall, while the subjective PROMs were cautiously reassuring, larger studies are needed to better understand the modifiable risk factors for MMRL repair failure after ACLR in pediatric patients.
Footnotes
Appendix
Comparison of the Index Operative Data of Patients Who Did and Did Not Undergo a Secondary Medial Meniscal Surgery After MMRL Repair and ACLR a

| No Secondary Medial Meniscal Surgery, n = 43 | Secondary Medial Meniscal surgery, n = 11 | P | |
|---|---|---|---|
| Pivot-shift grade | .169 | ||
| 0 | 1 (2.3) | 1 (9.1) | |
| 1 | 21 (48.8) | 4 (36.4) | |
| 2 | 14 (32.6) | 6 (54.5) | |
| 3 | 7 (16.3) | 0 (0) | |
| Lachman grade | |||
| 1 | 1 (2.3) | 0 (0) | |
| 2 | 32 (74.4) | 9 (81.8) | |
| 3 | 10 (23.3) | 2 (18.2) | |
| MMRL repair technique | .327 | ||
| All-inside | 37 (86) | 11 (100) | |
| Inside-out | 6 (14) | 0 (0) | |
| MMRL repair sutures | 3 ± 1.4 (1-7) | 2.6 ± 0.9 (1-4) | .687 |
| Concomitant LMT | .167 | ||
| Yes | 23 (53.5) | 9 (81.8) | |
| No | 20 (46.5) | 2 (21.2) | |
| LMT treatment, n = 32 | ≥.999 | ||
| Repair | 14 (60.9) | 6 (66.7) | |
| Meniscectomy | 6 (26.1) | 2 (22.2) | |
| Observation | 3 (13) | 1 (11.1) | |
| LMT repair technique, n = 20 | ≥.999 | ||
| All-inside | 11 (78.6) | 6 (100) | |
| Inside-out | 1 (7.1) | 0 (0) | |
| Transtibial root | 2 (14.3) | 0 (0) | |
Data reported as n (%). ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; LMT, lateral meniscal tear; MMRL, medial meniscal ramp lesion.
Final revision submitted October 10, 2025; accepted October 15, 2025.
Authors
Jay Moran, MD (Department of Rehabilitation and Orthopedics, Yale School of Medicine, New Haven, Connecticut, USA); Jason Z. Amaral, BS (Texas Children's Hospital, Houston, Texas, USA); Ruth H. Jones, BS (Department of Pediatric Orthopedic Surgery, Hospital for Special Surgery, New York, USA); Udit Dave, BS (Department of Sports Medicine Surgery, Rush University, Chicago, Illinois, USA); Michael S. Lee, BA (Department of Rehabilitation and Orthopedics, Yale School of Medicine, New Haven, Connecticut, USA); Stuart D. Ferrell Jr, MBS (Texas Children's Hospital, Houston, Texas, USA); Luke V. Tollefson, BS (Twin Cities Orthopedics, Edina, Minnesota, USA); Christopher M. LaPrade, MD (Twin Cities Orthopedics, Edina, Minnesota, USA); Lee D. Katz, MD (Department of Radiology, New Haven, Yale School of Medicine, Connecticut, USA); Jack Porrino, MD (Department of Radiology, New Haven, Yale School of Medicine, Connecticut, USA); Elizabeth Gardner,† MD (Department of Rehabilitation and Orthopedics, Yale School of Medicine, New Haven, Connecticut, USA); Christina R. Allen,† MD (Department of Rehabilitation and Orthopedics, Yale School of Medicine, New Haven, Connecticut, USA); Andrew E. Jimenez, MD (Department of Rehabilitation and Orthopedics, Yale School of Medicine, New Haven, Connecticut, USA); John P. Fulkerson, MD (Department of Rehabilitation and Orthopedics, Yale School of Medicine, New Haven, Connecticut, USA); Timothy E. Hewett, PhD (Department of Orthopedic Surgery, Marshall University, Huntington, West Virginia, USA); Nikhil N. Verma, MD (Department of Sports Medicine Surgery, Rush University, Chicago, Illinois, USA); Jorge Chahla, MD, PhD (Department of Sports Medicine Surgery, Rush University, Chicago, Illinois, USA); Michael J. Medvecky, MD (Department of Rehabilitation and Orthopedics, Yale School of Medicine, New Haven, Connecticut, USA); Peter D. Fabricant, MD, MPH (Department of Pediatric Orthopedic Surgery, Hospital for Special Surgery, New York, USA); Scott D. McKay, MD, MPH (Texas Children's Hospital, Houston, Texas, USA); and Robert F. LaPrade, MD, PhD (Twin Cities Orthopedics, Edina, Minnesota, USA).
One or more of the authors has declared the following potential conflict of interest or source of funding: A.E.J. has received hospitality payments from Abbott Laboratories; and support for education from Polaris Technology Solutions, Gotham Surgical Solutions & Devices, and Medwest Associates. R.F.L. has received royalties from Arthrex and Smith & Nephew. P.D.F. has received consulting fees from WishBone Medical. J.C. has received consulting fees from Smith & Nephew and DePuy Synthes; and support for education from Midwest Associates. N.N.V. has received research support from Breg and Ossur; consulting fees from Arthrex and Stryker; royalties from Graymont Professional Products and Smith & Nephew; and hospitality payments from Spinal Simplicity. M.J.M. has received both consulting and nonconsulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.