
Abstract
Background:
Anterior cruciate ligament (ACL) injuries are prevalent among elite athletes, particularly in high-impact sports. While ACL reconstruction (ACLR) is the gold-standard treatment, graft failure rates can exceed 30% in high-risk populations. Moreover, associated meniscal injuries often necessitate secondary surgical interventions. Implementing a systematic surgical approach, including advanced meniscal repair techniques and lateral extra-articular procedures, may enhance outcomes and reduce reoperation rates.
Purpose/Hypothesis:
This study aimed to assess the effect of a systematic approach to ACLR on secondary surgery rates and ACL graft survival among professional athletes. It was hypothesized that this approach would significantly reduce secondary surgeries and ACL graft failures.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective analysis of data from the SANTI database, focusing on professional athletes who underwent primary ACLR performed by a single senior surgeon between 2003 and 2020, was performed. Patients were categorized into 2 groups: those before October 2012 and those treated after the introduction of a systematic surgical approach. Primary outcomes included ACL graft rupture rates and secondary surgery rates (meniscectomy and revision ACLR). Cox proportional hazards models were used to evaluate risk factors.
Results:
The final cohort comprised 342 patients, with 130 treated before October 2012 and 212 after the introduction of a systematic protocol. Athletes treated after October 2012 exhibited a significantly lower rate of secondary surgery (30.0% before vs 16.5% after, P = .0174) and reduced ACL graft rupture rates (13.1% before vs 6.6% after, P = .0039). The 7-year graft survival rate improved from 86.9% before October 2012 to 93.3% after that month. Notably, younger athletes (<21 years) had an elevated risk of reoperation (hazard ratio, 2.090) and graft failure (hazard ratio, 2.224). The systematic approach also led to a significant reduction in the rate of secondary medial meniscectomy (10.8% vs 3.3%, P = .0052).
Conclusion:
A systematic approach to ACLR significantly reduced secondary surgeries and graft failure rates in elite athletes. These findings support the routine use of advanced meniscal repair techniques and lateral extra-articular procedures to enhance long-term outcomes.
Keywords
Anterior cruciate ligament (ACL) injuries are among the most common and debilitating knee injuries in elite sports, particularly in high-risk sports characterized by frequent pivoting, sudden cutting, and jumping.8,10,16 Given the significant physical demands placed on the knee joint, ACL injuries have a significant effect on an athlete's career. ACL reconstruction (ACLR) is the gold standard surgical procedure for restoring knee stability and facilitating return to play.3,27 However, despite surgical advances, graft failure remains a persistent problem, reported in over 30% of cases in high-risk populations.6,13,14
Graft failure is a career-threatening event, contributing to the inability of up to 20% of elite athletes to return to preinjury performance levels. 17 Several factors contribute to ACL graft failure, with technical errors and untreated secondary knee pathologies being the most common. 1 Among these secondary pathologies, meniscal lesions are of particular importance as they are the most common indication for secondary surgery after ACLR.19,24 Certain meniscal lesion patterns, such as longitudinal tears in the posterior horn of the medial meniscus or meniscocapsular injuries of the posterior horn, commonly referred to as ramp lesions, can often go undetected during standard anterior knee arthroscopy and preoperative imaging.15,32 Failure to address these lesions can result in increased rotational laxity, excessive anterior translation, and ultimately ACL graft failure.9,21 Therefore, a careful, systematic arthroscopic evaluation, including a trans-notch view to explore the posteromedial knee compartment, is essential to optimize diagnostic accuracy. 32
In addition to meniscal pathology, residual anterolateral instability after ACLR remains a significant factor in graft failure. 11 Biomechanical studies suggest that isolated ACLR fails to restore normal knee kinematics. Lateral extra-articular procedures (LEAPs), including lateral extra-articular tenodesis (LET) and anterolateral ligament reconstruction (ALLR), have gained interest as adjuncts to ACLR to address this issue. Recent studies suggest that combining ACLR with LEAPs restores native knee kinematics and significantly reduces graft failure rates, particularly in high-risk patients. In a cohort of professional athletes, the addition of a LET reduced the revision rate by nearly 3 times (9.5% vs 3.4%) compared with isolated ACLR. 2 Similar results have been reported in elite alpine skiers, where ACLR combined with a LEAP reduced graft rupture rates from 34.0% to 6.5%. 14
Given the high performance demands and financial implications associated with ACL injuries in professional sports, any ACLR strategy should aim to minimize the number of surgical procedures required and reduce time away from competition. The aim of this study was to evaluate the effect of systematic arthroscopic evaluation, enhanced meniscal repair techniques, and the addition of LEAPs on the rates of secondary surgery in professional athletes undergoing ACLR. The hypothesis was that this comprehensive surgical approach would reduce the incidence of secondary surgery and improve ACL graft survival in elite athletes.
Methods
Study Design, Participants, and Exclusions
Institutional review board approval (IRB No. COS-RGDS-2022-02-004-SONNERY COTTET-B) was granted for this retrospective cohort study. A retrospective analysis was conducted using prospectively collected data from the SANTI database. The study included professional athletes who underwent primary ACLR using autograft performed by the senior author (B.S.-C.) between January 2003 and January 2020. The diagnosis of an ACL graft rupture was based on clinical examination and magnetic resonance imaging. Indications for a particular type of ACLR (isolated or combined with a LEAP) were based on patient factors, patient choice, and the evolving indications for concomitant LEAPs noted by the senior surgeon during the study period. A systematic surgical approach that included a standardized arthroscopic assessment, advanced meniscal repair techniques, and LEAPs was implemented after October 2012. To assess the effect of this approach, athletes were categorized according to the date of surgery: before October 2012 and after October 2012. Athletes were included if they had a minimum follow-up of 2 years after ACLR. Patients who underwent multiligament reconstruction or osteotomy were excluded. Only those with complete follow-up data were analyzed.
Surgical Technique
All surgical procedures were performed by the senior author (B.S.-C.) in accordance with previously published descriptions, as summarized below.22,25,31,33
All patients were placed in a supine position with the knee flexed to 90°. A lateral support, foot roll, and tourniquet were utilized. Arthroscopic inspection of the knee and meniscal surgery were performed before the ACLR.
ACLR With a Bone–Patellar Tendon–Bone Graft
A 10-mm bone–patellar tendon–bone (BPTB) graft was harvested with a 9 × 15–mm patellar bone plug and an 11 × 20–mm tibial bone plug. The femoral tunnel was drilled in an outside-in fashion. The graft was passed through the femoral tunnel in an antegrade fashion. The graft was fixed in the femoral tunnel using a press-fit technique and then fixed in the tibial tunnel with the knee flexed at 30° using an interference screw (Bio-Interference Screw; Arthrex). 22
ACLR With a Quadriceps Tendon Graft
A 10-mm quadriceps tendon graft was harvested with a 10 × 25–mm patellar bone plug. The femoral tunnel was drilled in an outside-in fashion. The graft was passed through the femoral tunnel in an antegrade fashion, ensuring the bone plug remained within the tibial tunnel. The graft was then fixed on both sides with bioabsorbable screws (Bio-Interference Screw; Arthrex). The graft was tensioned and fixed on the femoral side with the knee flexed at 30°. 25
ACLR With a Hamstring Tendon Graft
The semitendinosus and gracilis tendons were harvested using an open-ended tendon stripper. The tibial insertion was preserved to improve fixation and vascularity. 36 The femoral tunnel was drilled in an outside-in fashion. Tendons were quadrupled and then fixed on both sides with bioabsorbable screws (Bio-Interference Screw; Arthrex). The graft was tensioned and fixed on the femoral side with the knee flexed at 30°. 33
Combined ACLR and ALLR
The hamstring tendons (HTs) were harvested as described above. A combined 4-strand ACL graft and single-strand anterolateral ligament (ALL) graft was prepared using a tripled semitendinosus with an additional length of gracilis sutured to it. A single femoral tunnel was drilled in an outside-in fashion. Intra-articularly, this was placed in a mid-anteromedial bundle position, and laterally, it was positioned at the femoral origin of the ALL (proximal and posterior to the lateral epicondyle). The ACL portion of the graft (3-part semitendinosus/1-part gracilis) was fixed on both sides using bioabsorbable screws (Bio-Interference Screw; Arthrex) with the knee flexed to 30°. The additional length of gracilis that emerged from the femoral tunnel at the lateral cortex formed the ALL portion of the graft. This was passed under the iliotibial band using a suture grasper through a tunnel in the proximal tibia and then back to the ALL origin, where it was tensioned and fixed with the knee in extension, forming an anatomic ALL reconstruction. 31
Modified Lemaire
A 9 × 1–cm strip of iliotibial band was harvested and remained attached to Gerdy's tubercle. The strip was passed under the lateral collateral ligament and then fixed at an isometric point (Krakow’s point) proximal and posterior to the lateral epicondyle using a bioabsorbable screw (Bio-Interference Screw; Arthrex). 20 The graft was fixed close to extension to avoid fixing the tibia in external rotation.
Systematic Surgical Approach
After October 2012, a standardized arthroscopic protocol was introduced, which included the following:
- Posterior visualization and posteromedial probing of the posterior horn of the medial meniscus, which helps discover a higher rate of lesions that could be easily missed through a standard anterior exploration. In numerous cases, these lesions can be “hidden” under a membrane-like tissue and discovered after minimal debridement through a posteromedial portal. 32
- Meniscal repair of ramp lesions through a posteromedial portal using a suture hook, which provides a high rate of meniscal healing 35
- The use of LEAPs, including ALLR and LET
Postoperative Rehabilitation Protocol
All patients participated in the same protocol, regardless of the surgical technique. This consisted of brace-free, immediate full weightbearing and progressive range of motion exercises, with restriction of range of motion to 0° to 90° for 6 weeks for patients who underwent meniscal repair. Early rehabilitation focused on maintaining full extension and quadriceps activation exercises. Return to sports was allowed at 4 months for nonpivoting sports, 6 months for pivoting noncontact sports, and 8 to 9 months for pivoting contact sports.
Follow-up and Data Collection
All patients were reviewed by the surgical team or a sports medicine physician at 3 and 6 weeks and 3, 6, 12, and 24 months. Physical examination and side-to-side measurements of anterior translation with a Rolimeter (Aircast Europa) were performed to assess the stability of the operated knee.
The study endpoint was determined to be December 31, 2021. Final follow-up for each patient was defined by the last patient follow-up recorded in prospectively collected data from the SANTI database. Patient notes were reviewed by an investigator, independent of the primary surgeons, to determine if the patient had sustained a further ipsilateral knee injury or undergone any reoperations or complications after the index procedure.
Statistical Analysis
Descriptive data analysis was conducted depending on the nature of the considered criteria. For qualitative data, this included the number of filled and missing data, as well as the frequency and percentage (referring to filled data) for each modality. Proportions were estimated, along with their exact 95% confidence intervals, when appropriate. Comparisons of data were made using the chi-square or Fisher exact test, according to the expected values under the assumption of independence. For quantitative data, this included the number of filled and missing data, the arithmetic mean, the standard deviation, the median, the first and third quartiles, and the minimum and maximum. Comparisons of data were made using a Student test or Mann-Whitney-Wilcoxon test, depending on the distribution of the variable of interest. The risk of graft failure occurrence was described in terms of the probability of occurrence and confidence interval using the Kaplan-Meier method. The different groups were compared using the log-rank test. For the analysis of graft failure occurrence, survival analysis was performed using a Cox proportional hazards model considering different adjustment factors. The Breslow method was used to account for tied times. The Cox model, which expresses the instantaneous risk of an event as a function of time and covariates, considers the follow-up period for each patient in addition to the occurrence of the event; therefore, the risk of event estimation is unbiased. Statistical significance was set at P < .05. All analyses were performed with SAS for Windows (v 9.4; SAS Institute).
Results
Patient Demographics and Baseline Characteristics
Of the 420 professional athletes who met the inclusion criteria, 342 had at least 2 years of follow-up and were included in the final analysis. In total, 130 athletes underwent surgery before October 2012 and 212 athletes after October 2012 (Figure 1).

Study flowchart. ACLR, anterior cruciate ligament reconstruction.
Patients treated before and after October 2012 were predominantly young male athletes participating in pivoting and contact sports, such as football and rugby (Table 1).
Characteristics of the Study Population a

Bold values indicate statistically significant differences between groups.
Surgical Technique Trends
The implementation of a systematic surgical protocol after October 2012 led to notable shifts in ACLR techniques. The use of combined procedures (ACLR + LEAP) increased from 39.2% to 85.4%, and the use of BPTB autografts decreased from 59.2% to 15.1%. Additionally, meniscal lesions were identified more frequently and therefore treated after October 2012 (Table 2).
Intraoperative Characteristics a

ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone; HT, hamstring tendon; LEAP, lateral extra-articular procedure; LM, lateral meniscus; MM, medial meniscus; QT, quadriceps tendon. Bold values indicate statistically significant differences between groups.
Overall Secondary Surgery Rates
Overall, 74 athletes (21.6%) underwent secondary surgery for graft rupture, secondary meniscectomy, or debridement of a cyclops lesion. Of these, 39 athletes (30.0%, including 13.1% for graft rupture) had a secondary procedure before October 2012, and 35 athletes (16.5%, including 6.6% for graft rupture) had a secondary procedure after October 2012 (P = .0174). The probability of avoiding secondary surgery at 7 years was 71.5% (95% CI, 62.9%-78.5%) before 2012 versus 82.4% (95% CI, 75.7%-87.4%) after 2012 (Figure 2).

Kaplan-Meier plot demonstrating the difference in the rates of secondary surgery before and after the introduction of systematic anterior cruciate ligament reconstruction. A significant difference in survivorship was found (P = .0256).
When the Cox model for subsequent surgery was adjusted for the date of surgery and the athlete's age at the time of the index procedure, those who underwent surgery before October 2012 had a 2.125 times higher risk (95% CI, 1.202-3.758) of requiring a secondary surgery compared with those treated after October 2012 (P = .0095).
A significant proportion of reinterventions were secondary medial meniscectomies: among athletes treated before October 2012, 14 of 130 (10.8%) underwent a secondary medial meniscectomy, compared with 7 of 212 (3.3%) of those operated on after October 2012 (P = .0052). The 7-year survival rate of avoiding secondary medial meniscectomy was 90.0% (95% CI, 83.4%-94.1%) before 2012 and 95.6% (95% CI, 90.4%-98.0%) after 2012.
A significant difference was demonstrated (P = .04260) for the difference in time (months) to secondary medial meniscectomy, between athletes operated before October 2012 and after October 2012 (Figure 3).

Kaplan-Meier plot demonstrating the difference in time to secondary medial meniscectomy surgery between athletes operated on before and after the introduction of systematic anterior cruciate ligament reconstruction. A significant difference is demonstrated (P = .0426).
There was no significant difference in the rate of secondary lateral meniscectomies, with 3 cases (2.3%) before October 2012 and 4 cases (1.9%) after October 2012 (P = .99), or for cyclops lesion debridement (P = .3832) or arthrolysis (P = .7475).
Graft Rupture
In athletes who underwent surgery before October 2012, 17 of 130 (13.1%) experienced graft rupture, while in those who underwent surgery after October 2012, 14 of 212 (6.6%) experienced graft rupture (P = .0039).
At 7 years, graft survival was 86.9% (95% CI, 79.8%-91.7%) before 2012 and 93.3% (95% CI, 89.0%-96.0%) after 2012. The adjusted Cox proportional hazards model on all risk factors showed that the risk of graft rupture was significantly associated with age (hazard ratio, 2.224; 95% CI, 1.070-4.620) and isolated ACLR (hazard ratio, 3.013; 95% CI, 1.100-8.251) (Table 3).
Adjusted Cox Model for Graft Rupture on All Risk Factors: Athletes With a 2-Year Follow-up (n = 342) a
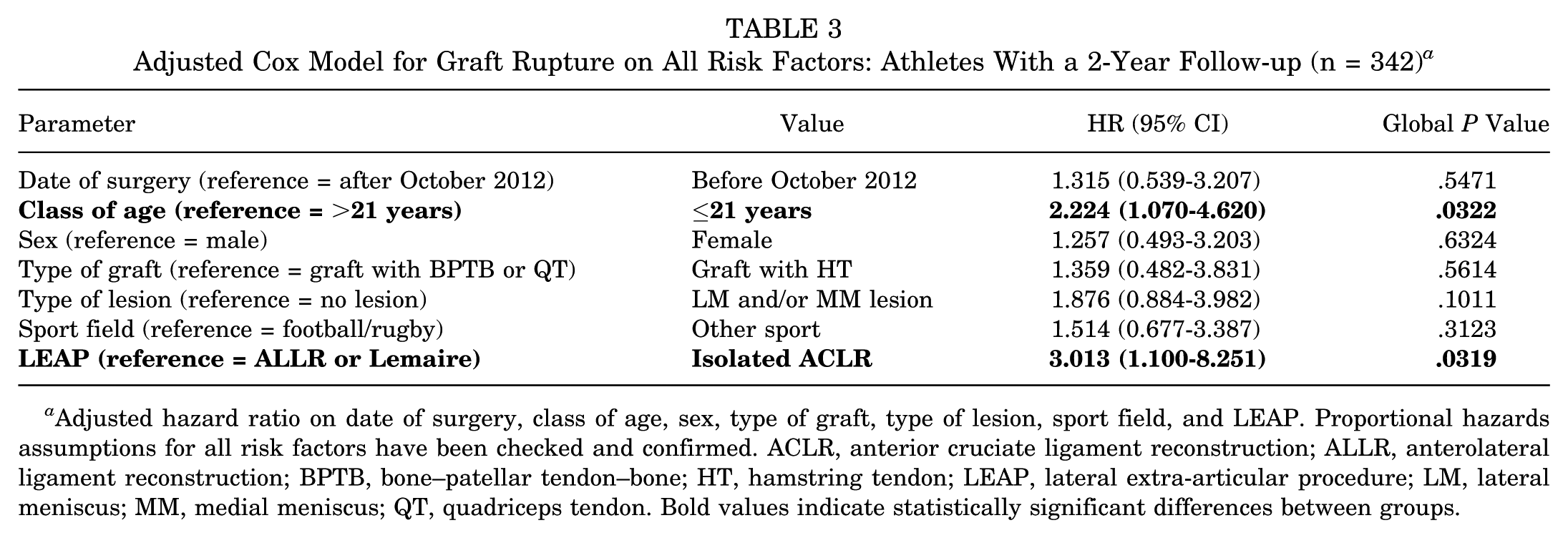
Adjusted hazard ratio on date of surgery, class of age, sex, type of graft, type of lesion, sport field, and LEAP. Proportional hazards assumptions for all risk factors have been checked and confirmed. ACLR, anterior cruciate ligament reconstruction; ALLR, anterolateral ligament reconstruction; BPTB, bone–patellar tendon–bone; HT, hamstring tendon; LEAP, lateral extra-articular procedure; LM, lateral meniscus; MM, medial meniscus; QT, quadriceps tendon. Bold values indicate statistically significant differences between groups.
Kaplan-Meier analysis (Figure 4) showed no significant difference in time to graft failure between the 2 groups (P = .1022).

Kaplan-Meier plot demonstrating the difference in time to anterior cruciate ligament reconstruction (ACLR) graft failure, before and after the introduction of systematic ACLR. No significant difference is demonstrated (P = .1022).
Discussion
The main finding of this study was that the implementation of a systematic ACLR approach after October 2012, including standardized meniscal assessment, advanced meniscal repair techniques, and the increased use of LEAPs, was associated with a significant reduction in the rates of secondary surgeries. The Cox proportional hazards model showed that athletes who underwent surgery before October 2012 had a 2.125-fold increased risk of secondary surgery compared with those treated after this period.
Younger athletes had a higher risk of revision surgery. Specifically, those younger than 21 years had a 2.090-fold increased risk of requiring secondary surgery compared with older athletes. This finding is consistent with the existing literature, which shows that younger patients require more ACLR revisions and have significantly higher rates of graft rupture.30,38 The higher revision rates in younger athletes may reflect their increased exposure to high-risk pivoting sports and potential biological factors influencing graft integration.4,28,37
The addition of LEAPs to ACLR in young, high-risk individuals has been shown to significantly reduce graft rupture and persistent rotational laxity while maintaining long-term functional outcomes.5,7,18,23 The STABILITY Group conducted a randomized controlled trial to assess whether the addition of LET to single-bundle hamstring autograft ACLR reduces the risk of clinical failure in young, active patients. 11 At 2 years postoperatively, the ACLR + LET group demonstrated a significantly lower clinical failure rate (25% vs 40%, P < .0001) and a 67% reduction in graft rupture (4% vs 11%, P < .001).
In addition, several reports showed that combining ACLR with LEAPs has a protective effect on meniscal repairs performed during ACLR, resulting in lower rates of secondary meniscectomy compared with isolated ACLR.26,34
In the current series, a significant shift in surgical strategy was observed regarding LEAPs. Before October 2012, 39.2% of athletes underwent a combined procedure, but after October 2012, 87.8% underwent a combined procedure of ACLR with ALLR or LEAP. A change in graft preference was also noted, with a significant increase in the use of HT grafts (from 29.2% to 84.0%) and a decrease in the use of BPTB grafts (from 59.2% to 15.1%) after October 2012. This trend is in line with wider ACLR practice, where HT has become the preferred graft choice due to its potential for lower donor site morbidity compared with BPTB. 29 In addition, the increased use of the gracilis tendon for ALLR has contributed to the greater acceptance of HT grafts as the primary choice for ACLR in this series.
The introduction of routine and systematic arthroscopic meniscal evaluation, including posterior visualization, probing via a trans-notch approach, and exploration of the posteromedial knee, resulted in a higher detection rate of meniscal injuries: 41.5% versus 55.6% of patients had a meniscal injury. Longitudinal lesions of the posterior horn of the medial meniscus were identified more frequently after October 2012, with 21 of 130 patients (16.2%) diagnosed before this period compared with 50 of 212 patients (23.6%) after. These findings suggest that many meniscal injuries may have gone undetected before the introduction of this systematic evaluation.
The overall rate of secondary surgery decreased significantly after the introduction of systematic ACLR (30.0% before October 2012 vs 16.5% after October 2012, P = .0174).
A significant proportion of reinterventions were secondary medial meniscectomies, with a notable decrease observed after October 2012 (10.8% vs 3.3%). This reduction may be due to more thorough exploration of the posteromedial region, combined with the adoption of improved meniscal repair techniques using a suture hook, which was introduced in October 2012. These findings are consistent with previous studies suggesting that suture-hook repair through a posteromedial portal is associated with a significantly lower rate of secondary meniscectomy compared with all-inside meniscal repair for longitudinal tears of the posterior horn of the medial meniscus performed at the time of ACLR combined with a LEAP. 12 Also, a significant difference is demonstrated for the difference in time (in months) to secondary medial meniscectomy between athletes operated before and after October 2012, highlighting the effect of meniscal preservation strategies introduced after 2012.
Limitations
This study has several limitations. First is its retrospective design, although data were collected prospectively. Second, all ACLRs were performed by a single senior surgeon, which, although ensuring surgical consistency, may limit the generalizability of the findings to other settings and surgeons using different techniques. Similarly, return to sport was allowed at 4 months for nonpivoting sports, 6 months for pivoting noncontact sports, and 8 to 9 months for pivoting contact sports, which may differ from current protocols in many countries. Finally, the changes in surgical approach after October 2012 were multifactorial, including systematic meniscal assessment, improved meniscal repair techniques, and increased use of LEAPs, making it difficult to isolate the contribution of each factor to the observed improvements in outcomes.
Conclusion
The introduction of a systematic approach to ACLR, including improved meniscal assessment, advanced meniscal repair techniques, and the widespread use of LEAPs, was associated with a significant reduction in the rates of secondary surgery and graft rerupture in professional athletes undergoing ACLR. These findings suggest that a comprehensive surgical strategy that emphasizes thorough meniscal evaluation and preservation, along with the routine use of LEAPs, enhances outcomes, particularly in high-risk populations such as elite athletes.
Importantly, young age (<21 years) remained an important risk factor for both graft rupture and secondary surgery.
Footnotes
Acknowledgements
The authors thank Horiana Health Data Consulting for their invaluable assistance with the statistical analyses and Ramsay Recherche et Enseignement for their support of the research conducted at Centre Orthopédique Santy.
Final revision submitted July 7, 2025; accepted September 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.S.-C. has received consulting fees and royalties from Arthrex. A.C. has received a grant from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Scientific Committee of the GCS Ramsay Santé for Education and Research (IRB No. COS-RGDS-2022-02-004-SONNERY COTTET-B).