
Abstract
Background:
Scope-assisted lower trapezius tendon transfer (SALTT) has emerged as a viable treatment option for posterosuperior irreparable rotator cuff tears (PSIRCTs) due to its biomechanical advantages and favorable clinical outcomes. However, there is limited research on deltoid muscle volume (DMV) and muscle strength recovery after SALTT.
Purpose:
To evaluate the changes in DMV and its effect on clinical outcomes—including muscle strength after SALTT.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This retrospective study analyzed 54 patients with PSIRCT who underwent SALTT from January 2021 to January 2022, with a minimum follow-up of 2 years. The deltoid muscle area of each 2-dimensional axial magnetic resonance image was identified and segmented using ITK-SNAP automatic segmentation software. The 3-dimensional (3D) deltoid muscle model was generated by combining each segmented 2D axial image, and the volume was automatically calculated. The clinical assessment included shoulder pain, patient-reported outcome measures (PROMs), active range of motion (aROM), and muscle strength of aROM.
Results:
The postoperative clinical outcomes were significantly improved after SALTT. The postoperative body mass index-adjusted DMV (aDMV) showed a statistically significant increase compared with the preoperative aDMV. Based on the mean postoperative Constant score, 32 patients had scores above the mean (optimal function group), while 22 patients had scores below the mean (suboptimal function group). The pre-aDMV and post-aDMV in the optimal function group were significantly larger than those in the suboptimal function group. However, there was no significant difference in ΔaDMV (the difference between pre-aDMV and post-aDMV) between the 2 groups. A graft rupture occurred in 6 patients. The graft-intact group showed statistically significantly better outcomes than the graft-rupture group. Although there was no difference in pre-aDMV between the 2 groups, post-aDMV and ΔaDMV were significantly larger in the graft intact group. The ΔaDMV is significantly correlated with postoperative PROMs, aROM, and muscle strength.
Conclusion:
This study confirmed that the postoperative aDMV was significantly increased after SALTT, and the increase of aDMV was significantly associated with good clinical outcomes—including PROMs, aROM, and aROM strength. These findings contribute to understanding the mechanism of aROM strength recovery by demonstrating an increase in DMV after SALTT.
Keywords
Recently, scope-assisted lower trapezius tendon transfer
The deltoid muscle plays a crucial role in shoulder function, significantly contributing to motion, stability, and strength of the shoulder joint.9,16 The deltoid muscle serves as the primary mover for shoulder forward elevation and abduction and works in coordination with the rotator cuff muscles to stabilize the humeral head in the glenoid cavity during shoulder motions.10,21 Moreover, the deltoid muscle generates significant force for lifting, pushing, and pulling activities, making it essential for daily activities.5,10 Previous studies have demonstrated that the deltoid muscle volume (DMV) was associated with clinical outcomes after reverse shoulder arthroplasty (RSA) or rotator cuff repair. 21 While the measurement of DMV is crucial for evaluating the shoulder function and clinical outcome, the methods for measuring the DMV are not standardized. 11 This lack of standardization leads to variability in results, making it difficult to compare findings across different studies or clinical assessments. 6 Moreover, there was no study evaluating the DMV after SALTT.
This study aimed to evaluate the changes in DMV after SALTT and their effect on clinical outcomes. For this, the DMV was measured using the magnetic resonance image (MRI)-based 3-dimensional (3D) reconstruction system. We hypothesized that DMV would increase after SALTT and that this increase is associated with improved postoperative clinical outcomes—including strength recovery. Therefore, a detailed study of muscle volume changes is a critical step in understanding the mechanisms of strength recovery and enhancing the clinical outcomes of SALTT.
Methods
This study was approved by the Ministry of Health and Welfare Institution Review Board (IRB no. 2023-0470-001), and informed consent was waived by the IRB.
Patients
This retrospective study analyzed patients with PSIRCTs who underwent SALTT from January 2021 to January 2022 and had a follow-up of at least 2 years.
PSIRCTs were defined as cases involving irreparable supraspinatus and infraspinatus based on preoperative MRI and intraoperative arthroscopic findings, while the subscapularis was either intact or repairable. SALTT was indicated in patients with PSIRCT who experienced persistent pain and dysfunction interfering with daily life despite >6 months of nonoperative treatment. Moreover, SALTT was indicated for patients without arthritic progression (Hamada classification 1 or 2) and without any infectious or neurological complications.
The inclusion criteria were patients who underwent SALTT for symptomatic PSIRCTs and were followed up for >2 years postoperatively. Among them, 5 patients who were not followed up before 2 years postoperatively and 6 patients with incomplete clinical or radiological evaluations were excluded. Finally, 54 patients were included.
Descriptive data and factors influencing outcomes are as follows: age, sex, body mass index (BMI), side of involvement, medical comorbidities, smoking status, preoperative Goutallier fatty infiltration grade of rotator cuff, Hamada grade, management for subscapularis and long head of biceps tendon (LHBT), and interpositional graft type.
Surgical Technique
All surgical procedures were performed by a single experienced orthopaedic surgeon (C.H.B.). The patients were prepared under general anesthesia in the lateral decubitus position. After diagnostic examination, if necessary, subscapularis repair was performed, and the LHBT was addressed with tenotomy or tenodesis. For harvesting the lower trapezius tendon, a horizontal skin incision approximately 5 cm in length is made at the midpoint of the scapular spine. The LT tendon was gently separated and freed from the infraspinatus fascia and middle trapezius tendon. An incision of the infraspinatus fascia and the space between the remnant posterior cuff and the deltoid muscle was developed for transferring the LT tendon. Then, the interpositional graft was prepared using either an Achilles tendon allograft (ATA) or a fascia lata autograft (FLA). The FLA was obtained from the ipsilateral lateral side of the thigh. The ATA and FLA were folded 2 to 3 times to achieve the desired graft size.
After preparing the interpositional graft, 2 medial-row anchors were secured in the anterior and posterior regions of the humeral head footprint. Three suture threads from the posterior anchors were passed through the posterior remnant cuff to create a side-to-side suture. The interpositional graft was introduced from the infraspinatus fascia incision to the subacromial space. The graft was then secured using a double-row suture bridge technique with the previously placed anterior medial-row anchors. The side-to-side sutures between the interpositional graft and the posterior remnant rotator cuff were completed. Subsequently, the interpositional graft was firmly fixed to these lateral-row anchors. After that, an unprepared portion of the graft was anastomosed to the inferior border of the LT tendon with the Krakow technique with maximal external rotation (ER) and 60° of abduction to ensure optimal physiological tension (Figure 1).

Arthroscopy-assisted lower trapezius tendon transfer. (A) Arthroscopic image of posterosuperior irreparable rotator cuff tears of the right shoulder. (B) Preparation of the lower trapezius tendon. (C) The Achilles tendon allograft is attached to the supraspinatus footprint. (D) The Achilles tendon allograft is attached to the inferior margin of the prepared lower trapezius.
Postoperatively, patients wore a shoulder brace maintaining the shoulder at 0° of external rotation for 6 weeks. After this period, they began a passive range of motion (ROM) exercise, which continued for 4 weeks. Subsequently, patients transitioned to active ROM (aROM) exercises and started gentle strengthening exercises.
DMV Measurement
MRI scans for DMV measurement were obtained using a 1.5-T Magnetom Amira (Siemens Healthineers). The patients were prepared in a supine position with the humerus in a neutral alignment and the palm oriented upward. MR images were scanned from the supraclavicular area to the mid portion of the deltoid, with an approximate length of 8 cm, using axial T1-weighted sequences (section thickness, 3 mm; field of view, 20.0 cm). All MR images were acquired digitally in the Digital Imaging and Communications in Medicine format using a picture archiving and communication system. ITK-SNAP automatic segmentation software (Version 4.2.2; University of Pennsylvania) was used to measure the DMV. The deltoid muscle area of each 2-dimensional (2D) axial MR image was identified and segmented using ITK-SNAP software. After that, the 3D deltoid muscle model was generated by combining each segmented 2D axial image. To ensure a consistent length of the 3D-reconstructed deltoid muscle for each patient, 25 2D axial images (25 × 3 mm = 7.5 cm) from the supraclavicular origin area were included. After creating the 3D deltoid muscle model, its volume was automatically calculated (Figure 2). The final DMV was then adjusted according to the patient's BMI (DMV/BMI ratio). Preoperative DMV and postoperative DMV (2 years after the operation) were measured and compared.

Deltoid muscle volume measurement. (A) Axial T1-weighted image of the right shoulder. (B) Demarcation of the deltoid muscle. (C and D) Creation of 3-dimensional deltoid muscle volume.
Outcome Measurement
The clinical assessment included shoulder pain, patient-reported outcome measures (PROMs), aROM, and muscle strength of aROM. Shoulder pain was evaluated using the visual analog scale (VAS) score. PROMs to evaluate shoulder function status included the Constant-Murley score and the American Shoulder and Elbow Surgeons (ASES) score. The minimal clinically important difference (MCID) of the Constant and ASES scores was calculated as one-half of the standard deviation of the delta between the preoperative score and the postoperative score. The MCIDs of the Constant and ASES scores were 7.5 and 8.5, respectively. The significant clinical benefit (SCB) of the Constant and ASES scores was 19.9 and 26, respectively.13,15 Also, aROM was measured for shoulder forward elevation, abduction, internal rotation, and external rotation using a standard goniometer. Shoulder forward elevation was measured by having the patient lift their arm in the sagittal plane with the elbow extended. Shoulder abduction is measured by having the patient raise their arm in the coronal plane with the elbow extended. Shoulder external rotation is measured by having the patient rotate their arm outward with the elbow flexed at 90°. Shoulder internal rotation was assessed by determining the highest spinal level the patient could reach behind their back with the tip of the thumb. Shoulder aROM strength is measured using a standard barometer by applying resistance to the movement and recording the force exerted at a specific joint angle (90° forward elevation, 90° abduction, neutral internal rotation, and neutral external rotation). Clinical assessments were conducted preoperatively and at 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. The preoperative clinical status was compared with the clinical outcomes at 2 years postoperatively. All clinical outcomes were objectively assessed by a research coordinator (S.J.K.) who blinded the patient's information and the details of this study.
The radiologic assessment included shoulder joint arthritis and graft integrity. Shoulder joint arthritis was assessed using the acromiohumeral distance (AHD), Hamada grade, and the progression of osteoarthritis (OA). AHD and Hamada grades were evaluated on true anteroposterior radiographs. The progression of shoulder joint OA was defined as a postoperative Hamada grade advancing to 3 or 4. Shoulder joint arthritis was assessed preoperatively and at 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. The preoperative radiologic status was compared with the radiologic outcome at 2 years after surgery.
Graft integrity was assessed using the Sugaya 20 Classification on postoperative MRI. A graft was considered a rupture if there was any discontinuity corresponding to Sugaya Classification 4 or 5 at the humeral attachment or mid-substance of the graft. The MRIs were obtained preoperatively, as well as at 1 month, 6 months, and 1 year postoperatively, and then conducted annually thereafter. Graft integrity was evaluated using MRI 2 years after surgery (Figure 3). All radiologic outcomes were objectively assessed by an experienced musculoskeletal radiologist who was blinded to the patient's information and the details of this study.

Postoperative magnetic resonance image of arthroscopy-assisted lower trapezius tendon transfer. (A) Axial T1-weighted and (B) Coronal T1-weighted images show the transferred lower trapezius tendon and Achilles allograft (arrow) of the right shoulder.
Statistics
Pre- and postoperative continuous variables were compared using the Wilcoxon signed-rank test, a nonparametric method, while categorical variables were evaluated using the McNemar test. Comparisons between the 2 groups were performed using the Mann-Whitney U test for continuous variables and the Fisher exact test for categorical variables. Bivariate correlation analysis was used to evaluate the relationship between DMV, demographic variables, and clinical outcomes. Statistical analyses were performed using the Statistical Package for the Social Sciences (IBM), with significance set at 95%.
To assess interobserver reliability for the DMV, the intraclass correlation coefficient (ICC) 14 was employed. An experienced orthopaedic surgeon (J.G.K.) and an evaluator (B.T.K.) independently and randomly assessed the DMV, with each evaluator blinded to the other's measurements. To determine intraobserver reliability, B.T.K. conducted a second evaluation using the same images 3 weeks after the initial measurement, without access to the previous ratings for any patient.
Results
The total of 54 patients had a mean age of 60.9 ± 7.5 years, and 20 patients were women (37%). The demographic and clinical characteristics of the patients are summarized in Table 1. The 2-year postoperative MRIs were obtained at a mean of 23.4 ± 1.4 months after surgery.
Demographic and Clinical Characteristics of Patients a

Data are presented as mean ± SD or n (%). ATA, Achilles tendon allograft; BMI, body mass index; FLA, fascia lata autograft; ISP, infraspinatus; SSC, subscapularis; SSP, supraspinatus; Tm, teres minor.
The postoperative clinical outcomes—including VAS score, PROMs (Constant-Murley score and ASES score), aROM (FE, ABD, ER at side), and muscle strength of aROM (FE, ABD, ER at the side)—showed a statistically significant improvement compared with the preoperative clinical assessment. Radiologically, there were no changes in the AHD and the Hamada grade before and after the operation. However, the postoperative adjusted DMV with BMI (aDMV) showed a statistically significant increase compared with the preoperative aDMV (7857.5 ± 2479.4 mm3 to 9177.9 ± 2791.4 mm3/kg/m2; 16.8%; P < .001) (Table 2 and Figure 4).
Preoperative Assessment and Postoperative Outcomes a
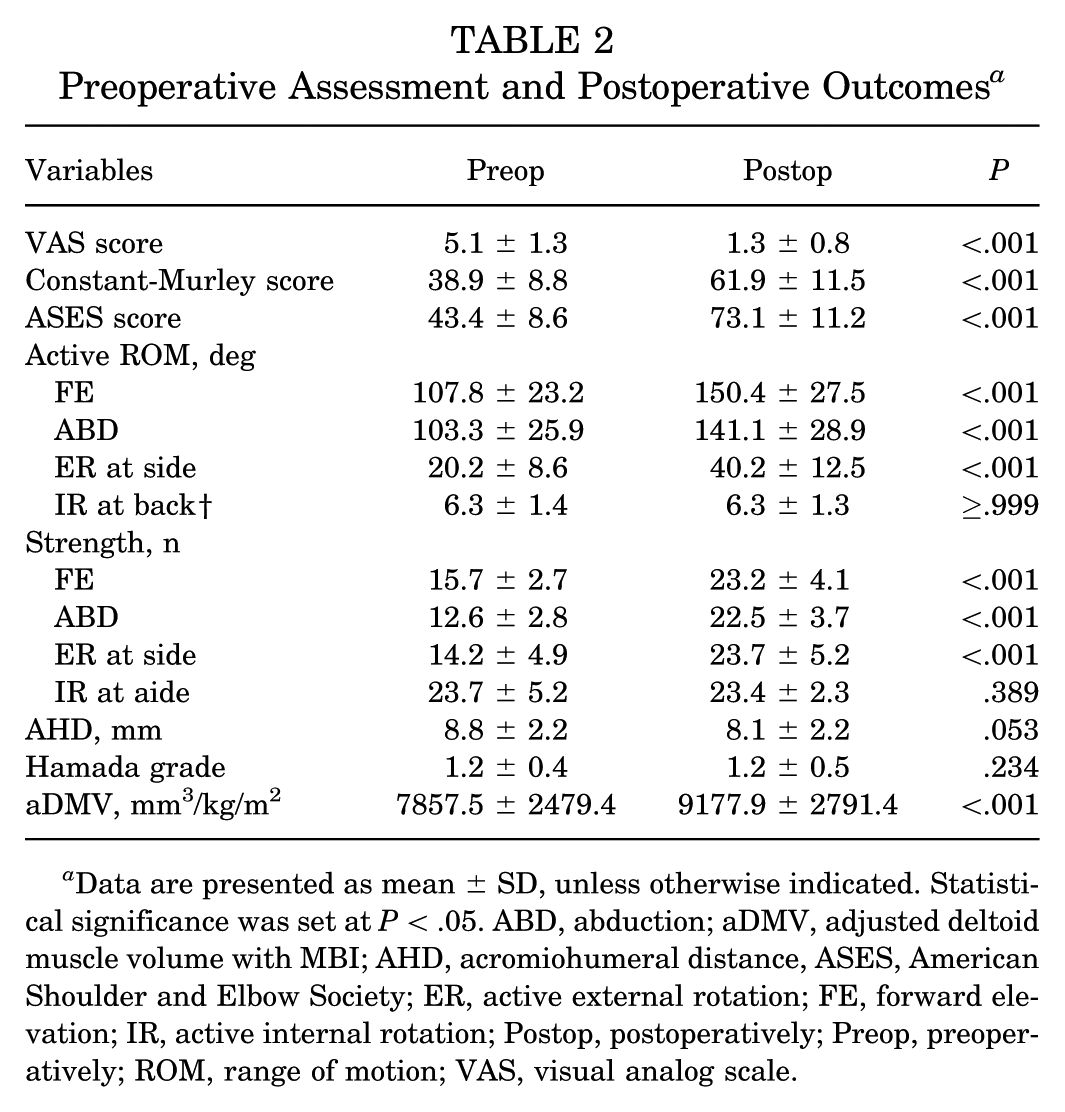
Data are presented as mean ± SD, unless otherwise indicated. Statistical significance was set at P < .05. ABD, abduction; aDMV, adjusted deltoid muscle volume with MBI; AHD, acromiohumeral distance, ASES, American Shoulder and Elbow Society; ER, active external rotation; FE, forward elevation; IR, active internal rotation; Postop, postoperatively; Preop, preoperatively; ROM, range of motion; VAS, visual analog scale.

The volume change of the DMV after arthroscopy-assisted lower trapezius tendon transfer. (A) The preoperative Axial T1-weighted image of the right shoulder. (B) The postoperative Axial T1-weighted image showed an increase in the DMV compared with the preoperative image. (C) Preoperative 3D DMV. (D) The postoperative 3D DMV showed a significant increase compared with the preoperative image. DMV, deltoid muscle volume; 3D, 3-dimensional.
For exploratory purposes, patients were grouped based on the mean postoperative Constant-Murley score, with 32 patients above the mean categorized as the optimal function group and 22 patients below the mean categorized as the suboptimal function group. This subgrouping was performed to compare trends in clinical outcomes and DMV descriptively. The optimal function group showed statistically significantly better outcomes than the suboptimal function group in Constant-Murley score, ASES score, ER aROM, and muscle strength (FE, ABD, and ER at side). The achievement of MCID for Constant (93.8% vs 40.9%; P < .001) and ASES (93.8% vs 63.6%; P = 0.001) scores was significantly better in the optimal function group. The achievement of SCB for Constant (93.8% vs 31.8%; P < .001) and ASES (87.5% vs 40.9%; P < .001) scores was significantly better in the optimal function group. Additionally, the pre-aDMV and post-aDMV in the optimal function group were considerably larger than those in the suboptimal function group. However, there was no difference in the difference between pre-aDMV and post-aDMV (ΔaDMV) between the 2 groups (Table 3).
Comparison of Postoperative Outcomes Between the Good Function and Poor Function Groups a

Data are presented as mean ± SD or n (%). Statistical significance was set at P < .05. ABD, abduction; AHD, acromiohumeral distance; ASES, American Shoulder and Elbow Society; ΔaDMV, difference between pre-aDMV and post-aDMV; ER, active external rotation; FE, forward elevation; IR, active internal rotation; ISP, infraspinatus; Post-aDMV, postoperative adjusted deltoid muscle volume with BMI; Pre-aDMV, preoperative adjusted deltoid muscle volume with BMI; ROM, range of motion; SSC, subscapularis; SSP, supraspinatus; Tm, teres minor; VAS, visual analog scale.
Among the total 54 patients, graft rupture occurred in 6 patients. The clinical outcomes and DMV were compared between the graft-intact group and the graft-rupture group. The graft intact group showed statistically significantly better outcomes than the graft retear group in PROMs (Constant-Murley score and ASES score), aROM (FE, ABD, and ER at the side), and muscle strength (FE, ABD, and ER at the side). Although there was no difference in pre-aDMV between the 2 groups, post-aDMV and ΔaDMV were significantly larger in the graft-intact group (Table 4). A post hoc power analysis based on the observed difference in Constant scores between the graft intact group (63.3 ± 11.1) and the graft rupture group (50.3 ± 6.9) yielded a Cohen's d of 1.40 and a statistical power of 84% (α = .05, 2-tailed). These results indicate that the study was adequately powered to detect meaningful differences in functional outcomes between the 2 groups.
Comparison of Postoperative Outcomes Between Graft Intact and Graft Rupture Groups a

Data are presented as n (%) or mean ± SD, unless otherwise specified. Statistical significance was set at P < .05. ABD, abduction; AHD, acromiohumeral distance; ASES, American Shoulder and Elbow Society; ΔaDMV, difference between pre-aDMV and post-aDMV; ER, active external rotation; FE, forward elevation; IR, active internal rotation; ISP, infraspinatus; Post-aDMV, postoperative adjusted deltoid muscle volume with BMI; Pre-aDMV, preoperative adjusted deltoid muscle volume with BMI; ROM, range of motion; SSC, subscapularis; SSP, supraspinatus; Tm, teres minor; VAS, visual analog scale.
In correlation analyses, the pre-aDMV was significantly correlated with sex, PROMs (Constant-Murley score and ASES score), and muscle strength (forward elevation [FE], abduction [ABD], and external rotation [ER] at the side). The post-aDMV was significantly correlated with sex, PROMs (Constant-Murley score and ASES score), aROM (ER at the side), and muscle strength (FE, ABD, and ER at the side). The ΔaDMV was significantly correlated with sex, PROMs (Constant-Murley score and ASES score), aROM (FE and ABD), and muscle strength (FE, ABD, and ER at side) (Table 5).
Correlation Analyses Between DMV and Clinical Outcomes a

Statistical significance was set at P < .05. ABD, abduction; aROM, active range of motion; ASES, American Shoulder and Elbow Society; DMV, deltoid muscle volume; ER, active external rotation; FE, forward elevation; ISP, infraspinatus; Post-aDMV, postoperative adjusted deltoid muscle volume with BMI; SSC, subscapularis; SSP, supraspinatus; Tm, teres minor.
This study demonstrated a high degree of interobserver reliability for DMV (ICC preoperative DMV = 0.993; P < .001; ICC postoperative DMV = 0.996; P < .001) and intraobserver reliability for DMV (ICC preoperative DMV = 0.997; P < .001; ICC postoperative DMV = 0.994; P < .001).
Discussion
This study evaluated the changes in DMV after SALTT and their effect on clinical outcomes. The main finding of this study is that the patients with PSIRCTs who underwent SALTT had significantly higher postoperative aDMV than preoperative aDMV, and the increase in aDMV was significantly associated with better clinical outcomes. Moreover, both preoperative and postoperative aDMV were significantly associated with postoperative clinical outcomes—including PROMs, aROM, and aROM strength. This study is significant as the first clinical investigation to identify the increase in DMV and its association with clinical outcomes after SALTT. Furthermore, this study contributes to understanding the mechanism of aROM strength recovery by demonstrating an increase in DMV after SALTT. These findings provide valuable insights into the mechanism of SALTT and offer shoulder surgeons useful information.
SALTT has become a joint-preserving treatment option for patients with PSIRCTs, owing to its biomechanical advantages and favorable clinical outcomes.1,7 Initially, SALTT was performed to restore external rotation in PSIRCTs by attaching the interpositional graft to the infraspinatus footprint on the greater tuberosity. 8 Biomechanically, SALTT attached to the infraspinatus footprint can reestablish the transverse plane force couple by substituting for the infraspinatus, as it closely mimics the natural line of pull of this muscle. 18 Recently, by attaching the interpositional graft to the supraspinatus footprint, SALTT has been able to ensure that the deltoid functions well by replicating the function of the supraspinatus across the full range of shoulder motion. 4 Moreover, under the subacromial space, an interpositional graft attached to the supraspinatus footprint could act as a static spacer. 2 Ultimately, SALTT provides dynamic stability by restoring force coupling of the glenohumeral joint and static stability under the subacromial space.2,4 With these biomechanical advantages, SALTT has demonstrated good clinical outcomes—including pain relief, improved PROMs, restored pseudoparalysis, and recovery of aROM strength in short-term and mid-term clinical studies.1,7 However, there is limited research on strength recovery and its mechanisms after SALTT. Therefore, studying the changes in DMV after SALTT is essential to understanding the mechanisms of aROM strength recovery.
The association between DMV and clinical outcomes after shoulder surgery is well established. 21 In RSA, the preoperative 2D cross-sectional area of the deltoid on MRI has been shown to correlate with PROMs and abduction strength. 6 A study using a 3D deltoid muscle model demonstrated that the preoperative DMV significantly affected the clinical outcome and served as an independent prognostic factor for good clinical outcomes after RSA. 21 Moreover, a study on DMV using ultrasound found that postoperative DMV was correlated with clinical outcome and abduction strength after RSA. 6 Similarly, higher preoperative DMV has been linked to improved functional outcomes after arthroscopic rotator cuff repair. 19 However, these studies primarily estimated DMV using a single image from 2D MRI or ultrasound images, limiting the accuracy of DMV measurement. Even in studies using a 3D deltoid muscle model, only the association between preoperative DMV and clinical outcomes was evaluated, while postoperative DMV remained unexamined.11,21 Therefore, this study is significant in that it evaluated preoperative and postoperative DMV using MRI-based 3D reconstruction software after SALTT and assessed its association with clinical outcomes.
This study confirmed that patients with PSIRCTs who underwent SALTT had significantly higher post-aDMV scores than pre-aDMV scores, and the increase in aDMV was significantly associated with optimal clinical outcomes. Additionally, the graft rupture group showed suboptimal clinical outcomes compared with the graft intact group and did not exhibit an increase in aDMV. These results are thought to be attributed to the restoration of shoulder joint stability through the restoring force coupling of the glenohumeral joint. 17 The deltoid muscle plays a crucial role in shoulder movement and stability. 16 However, its effectiveness is improved with the integrity of the rotator cuff and overall shoulder stability. In case of massive rotator cuff tears, the superior translation force of the deltoid cannot be adequately counterbalanced, leading to loss of aROM and the progression of arthritic changes. 10 Therefore, by improving shoulder stability, SALTT may enable the deltoid muscle to function more effectively, thereby enhancing clinical outcomes in PSIRCTs. Furthermore, biomechanical studies have shown that SALTT itself contributes to increased deltoid force and function in a cadaveric model of massive rotator cuff tears. 17 According to the tendon transfer principle, the transfer itself leads to loss of transferred muscle power, and therefore, it cannot increase muscle power. 12 As a result, it can be thought that SALTT increases deltoid function by improving shoulder stability. The normalization of deltoid muscle function leads to an increase in DMV, which may be associated with improved muscle strength after SALTT. However, various factors may influence muscle strength, and the increase in DMV may be one of these factors. Therefore, future studies, such as prospective cohort studies or mediation analyses that control for other variables affecting muscle strength recovery, will be necessary to confirm the direct relationship between the increase in DMV and muscle strength recovery.
Although this study is meaningful as the first clinical study to identify the increase in DMV and its association with clinical outcomes after SALTT, it had several limitations. First, the small number of patients without a comparator, such as an alternative tendon transfer or surgical technique, in this study may be a limitation, potentially leading to a lack of statistical significance in the study results. Future comparative studies with a larger number of patients will be necessary to reduce the possibility of a type 2 error. Second, the short follow-up period in this study may be a limitation in assessing the long-term effects on DMV change. Third, the method used to evaluate DMV is an approximation because the entire deltoid muscle was not captured in the MRI scan. While previous studies using a 3D deltoid muscle model have calculated total DMV based on MRI-derived measurements, they did not directly measure the entire DMV in practice. However, the present study is meaningful because DMV changes were evaluated by measuring preoperative DMV and postoperative DMV over the same range in all patients. Fourth, this study only assessed ipsilateral DMV, without comparing it with other shoulder muscles or with the deltoid muscle of the contralateral shoulder. Fifth, pre- and postoperative MRI scans may show different axial planes, which can potentially affect the consistency of DMV measurements. Nonetheless, the same MRI device was used in all patients with an arm-positioning fixture applied during the scan. Sixth, there may be potential measurement errors in assessing DMV. However, because the intra- and interobserver reliability of DMV measurement is excellent, the likelihood of measurement errors is expected to be minimal. Additionally, a limitation of this study is that the quality of the deltoid muscle and fatty degeneration could not be evaluated. Finally, several other factors, such as sex and rehabilitation compliance, that may affect PROMs and/or aDMV were not assessed, and the sample size was insufficient to perform multivariate analysis. Nevertheless, it is important to emphasize that this study represents the first attempt to investigate DMV changes after SALTT in patients with PSIRCTs.
Conclusion
This study confirmed that the postoperative aDMV was significantly increased after SALTT, and the increase in aDMV was significantly associated with good clinical outcomes—including PROMs, aROM, and aROM strength. This study contributes to understanding the mechanism of aROM strength recovery by demonstrating an increase in DMV after SALTT.
Footnotes
Final revision submitted July 31, 2025; accepted August 26, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ministry of Health and Welfare (IRB No. 2023-0470-001).