
Abstract
Background:
Rotator cuff tears (RCTs) are common in older athletes and are a leading cause of shoulder pain and movement limitation. Nevertheless, the prevalence and associated factors of RCTs in older baseball players remain unclear.
Purpose:
To determine the prevalence, symptoms, and associated factors of RCTs in older baseball players.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 260 older baseball players (520 shoulders; mean age, 69.3 ± 6.1 years) who participated in league games organized by the Kanagawa Over–60 Rubber Baseball Association were included. RCTs were diagnosed using ultrasonography. Variables assessed included age, total years of baseball experience, smoking history, history of present illness (hypertension, diabetes, and hyperlipidemia), and playing position. After determining the prevalence of RCTs and the proportion of shoulder pain, we performed a logistic regression analysis to identify factors related to RCTs on the throwing side.
Results:
Among the 260 participants (520 shoulders), the overall prevalence of RCTs was 37.7%. Also, 26.5% had a tear on the throwing side, 22.3% on the nonthrowing side, and 11.2% on bilateral sides, with no significant difference between sides. Among the 69 participants (mean age, 71.2 ± 5.6) with RCTs on the throwing side, 46 (66.7%) were asymptomatic. Using logistic regression analysis, we identified older age (odds ratio [OR], 1.06 [95% CI, 1.01-1.12]) and total years of baseball experience (OR, 1.02 [95% CI, 1-1.04]) as factors associated with RCTs on the throwing side. After excluding players with RCTs on the bilateral sides, total years of baseball experience (OR, 1.03 [95% CI, 1-1.05]) and participation frequency per week (OR, 1.40 [95% CI, 1.04-1.89]) were significantly associated with RCTs on the throwing side.
Conclusion:
This study revealed that 26.5% of older baseball players had RCTs in their throwing shoulder, of which two-thirds were asymptomatic. Additionally, the prevalence of RCTs was similar on the throwing and nonthrowing sides. Age was the most relevant factor associated with RCTs on the throwing side. However, after excluding those with RCTs on the bilateral sides, a high frequency of weekly participation was more strongly associated with the presence of RCTs than was age.
Participating in sports activities promotes physical and mental health in older adults, contributing to extended healthy life expectancy and reduced health care costs. 35 Baseball requires a range of whole-body movements—including throwing, hitting, running, and catching—and it can be played by older adults. At the recreational level, the physical effort required for baseball is equivalent to brisk walking, 13 making it a feasible and safe activity for this population. In Japan, the Japan Over–60 Rubber Baseball Association, which welcomes participants aged ≥60 years, has over 20,000 registered members. 15 To address age-related physical limitations, the association modifies standard baseball rules, similar to those in youth baseball, where rubber balls are used, reducing the distance between bases to 25 meters and that from the pitcher's plate to home base to 16.3 meters, as well as adopting a 7-inning format. These changes reduce physical demands and promote participation among older adults.
Older adults are susceptible to pain and disability due to age-related declines in physical function, potentially hindering their ability to continue sports activities. A previous study revealed that shoulder joint pain is the most prevalent musculoskeletal complaint among baseball players aged ≥60 years. 14 Rotator cuff tears (RCTs) are a leading cause of shoulder pain in the older population, with increasing prevalence in those aged >60 years. 36 The cause of RCTs is not fully understood; however, their occurrence is attributed to multiple mechanisms—including age-related degenerative changes, repetitive mechanical stress, and external trauma.2,11 Risk factors for RCTs include intrinsic factors such as advancing age, high body mass index, smoking, hypertension, and diabetes, as well as extrinsic factors such as repetitive overhead motions and prolonged shoulder elevation during activity.1,4,7,8,42 Consequently, older adults who frequently use their shoulder joints are at an increased risk of developing RCTs.
RCTs can be symptomatic or asymptomatic, with a reported prevalence of >30% in the general older population. 36 Approximately two-thirds of RCTs are asymptomatic 24 and do not immediately impair shoulder function. Nonetheless, the tear may progress over time in some individuals with RCTs, regardless of whether symptoms are present or absent.6,40 This progression can eventually lead to functional impairments such as developing shoulder pain, reduced range of motion, and muscle weakness.3,17,21,27,37 Therefore, early detection of asymptomatic RCTs and prevention of their progression to symptomatic stages are essential for older players to continue playing baseball. However, effective strategies for early detection remain limited owing to the absence of apparent symptoms in daily life.
As older baseball players are particularly susceptible to RCTs due to the combined effects of age-related degeneration and repetitive mechanical stresses from throwing, this population may exhibit a higher prevalence of RCTs than the general older population reported in previous studies.24,39 In contrast, many individuals may have asymptomatic RCTs and continue playing baseball without being aware of their condition. In addition, playing positions that involve frequent throwing (pitcher and catcher) and longer baseball experience may contribute to the development of RCTs. Examining the prevalence and associated factors of RCTs in older baseball players may contribute to the development of strategies for early diagnosis and intervention, including those for asymptomatic cases. Therefore, in this study, we aimed to determine the prevalence of RCTs and identify their associated factors in older baseball players. We hypothesized that the prevalence of RCTs in the throwing shoulder of older baseball players exceeds that reported in the general older population in previous epidemiological studies,24,39 and that this condition is associated with specific factors of the game, such as playing position and years of experience.
Methods
In this observational, cross-sectional study, we invited 920 male baseball players from the Kanagawa Over–60 Rubber Baseball Association between January and February 2024. The association allows participation for those who turn 60 within the league year, permitting entry from the age of 59 years. Those who regularly play baseball (at least once per month) and participate in the Kanagawa Over–60 Rubber Baseball Association league games were included. We addressed potential sources of bias by excluding those who (1) were aged <59 years, (2) had <6 months of recent competitive experience, (3) had a history of rotator cuff repair, and (4) developed shoulder pain on the throwing side within 2 weeks before the examination.
Before the examination, participants completed structured questionnaires to collect demographic and clinical data—including age, total years of baseball experience (excluding blank periods), main playing position (pitcher, catcher, or fielder), dominant throwing side, frequency of participation per week, history of current illness (hypertension, diabetes mellitus, and hyperlipidemia), heavy labor experience (construction, fishery, forestry, and agriculture), smoking status, and with a history of rotator cuff surgery and shoulder pain during throwing. In this study, symptomatic was defined as throwing-related pain in the throwing shoulder that had persisted for at least 2 weeks at the time of the survey. 33 Pain intensity was assessed using the visual analog scale (VAS). Symptoms and functional limitations on the throwing side were evaluated using the Quick Disabilities of the Arm, Shoulder and Hand Questionnaire (QuickDASH). Body composition (skeletal muscle index and body fat) was measured using a multifrequency bioelectrical impedance analysis (MF-BIA: MC-780A-N; TANITA Corp).
RCTs were assessed in bilateral shoulders using ultrasonography performed with the SNiBLE yb device equipped with a 12-MHz linear array probe (Konica Minolta). All assessments were conducted by a single experienced musculoskeletal physical therapist (M.A.) with >10 years of clinical expertise to minimize interobserver variability. Participants were seated with elbows flexed at 90° and shoulders slightly extended. After obtaining short-axis images of the long head of the biceps tendon, the probe was rotated 90° and shifted upward and posteriorly to capture long-axis views of the superior and middle facets of the greater humeral tubercle. Each facet was recorded twice per shoulder. These imaging techniques followed the guidelines of the Ultrasound Subcommittee of the European Society of Musculoskeletal Radiology. 22
Before the examination, intra-examiner reliability was evaluated using 34 shoulders from 17 older baseball players through 2 assessments conducted 1 hour apart, yielding a kappa coefficient of 1.0.
Ultrasonographic images were reviewed in a blinded manner by a single experienced shoulder surgeon (Y.S.), who diagnosed full-thickness RCTs defined as tendon discontinuity, thinning, defects, or a concave rotator cuff surface.24,39 Only full-thickness tears were considered in RCTs, as ultrasound has lower sensitivity for detecting partial-thickness tears compared with magnetic resonance imaging.5,32 Written informed consent was obtained from all participants. The Research Ethics Committee of the Faculty of Medicine, Juntendo University, approved this study protocol (E22-0335).
Statistical Analysis
Epidemiological data were reported as the mean and standard deviation, and percentages where appropriate. Data normality was assessed using the Shapiro-Wilk test. Participants who had RCTs on the throwing shoulder (regardless of the presence or absence of RCTs on the nonthrowing side) were categorized into the With RCTs group, while the remaining participants were in the Without RCTs group. Unpaired t tests, Mann-Whitney U tests, or chi-square tests were used for group comparisons where appropriate. The prevalence of RCTs between the throwing and nonthrowing shoulders was compared using the McNemar test. To identify factors associated with RCTs on the throwing side, logistic regression analysis was performed using independent variables—including age, hypertension, diabetes, smoking, total years of baseball experience, playing position, and weekly baseball frequency. In addition, after excluding participants with bilateral RCTs, separate logistic regression analyses were performed to evaluate baseball-related factors associated with RCTs on the throwing and nonthrowing sides. Independent variables in this analysis were age, total years of baseball experience, playing position, and weekly baseball frequency. These variables were selected using factors identified in a previous review41,42 and those found to be significant in the univariate analysis. Correlational analysis was also performed considering multicollinearity among the independent variables. The number of independent variables was sufficient for the sample size (n = 260), according to Peduzzi et al. 31 Analyses were conducted using the Statistical Package for Social Sciences Version 29.0 (IBM), with significance set at P < .05.
Results
A total of 280 participants provided informed consent, and bilateral shoulders were examined in all cases. After excluding 17 participants based on the exclusion criteria, 263 participants (526 shoulders) were included in the study. After excluding the 3 participants with incomplete data, 260 participants (520 shoulders; mean age, 69.3 ± 6.1 years) were included in the final analysis (Figure 1).

Flowchart showing the inclusion and exclusion criteria for this study.
The ultrasonography results showed that the prevalence of RCTs was 26.5% (69 of 260 participants) in the throwing shoulder, 22.3% (58 of 260 participants) in the nonthrowing shoulder, 11.2% (29 of 260 participants) in bilateral shoulders, and 37.7% (98 of 260 participants) in either or bilateral shoulders (Figure 2). The prevalence of RCTs did not differ significantly between the throwing and nonthrowing sides.
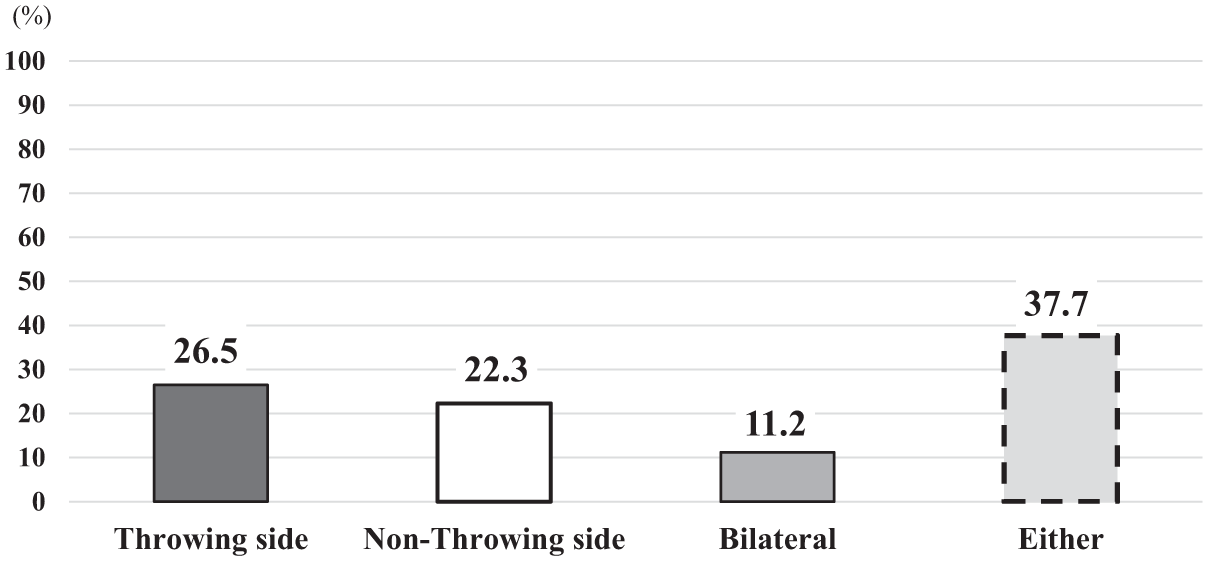
Prevalence of RCTs. RCTs, rotator cuff tears. Either includes those who had RCTs on either the left or right shoulder, as well as those with bilateral sides.
The With RCTs group was significantly older, had a longer playing history, and played more frequently per week than did the Without RCTs group (Table 1). Details are presented in Table 1 and Appendix Table A1.
Characteristics of Throwing Side Rotator Cuff Tears and Nonrotator Cuff Tears Groups a

Data are shown as n (%), mean (SD), and number. The Skeletal Muscle Index was calculated by dividing the sum of the arm and leg muscle mass by the square of height. Bold values indicate statistical significance at P < .05. BMI, body mass index; RCTs, rotator cuff tears.
No significant difference was observed between the With RCTs and Without RCTs groups in the prevalence of shoulder symptoms during throwing, VAS scores, or QuickDASH scores (Table 2). Notably, the prevalence of symptoms was nearly identical between the With RCTs group (33.3%) and the Without RCTs group (33.5%).
Prevalence of RCTs and Symptomatic Shoulder During Throwing a
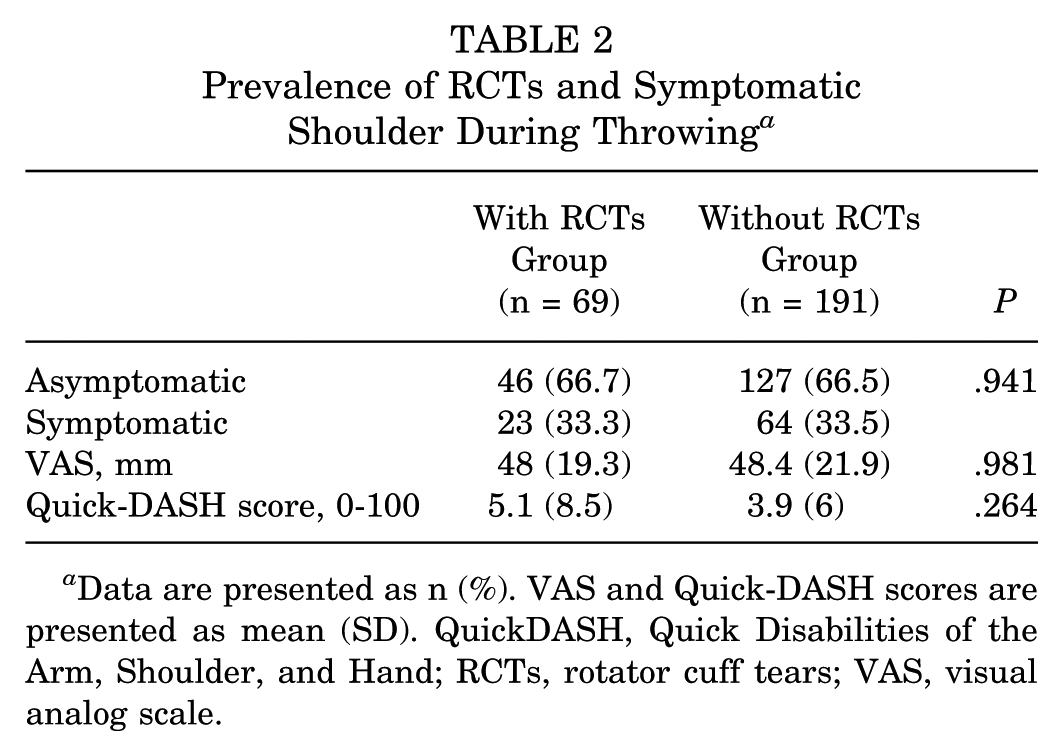
Data are presented as n (%). VAS and Quick-DASH scores are presented as mean (SD). QuickDASH, Quick Disabilities of the Arm, Shoulder, and Hand; RCTs, rotator cuff tears; VAS, visual analog scale.
Logistic regression analysis revealed that the variables associated with RCTs on throwing side were age (odds ratio [OR], 1.06 [95% CI, 1.01-1.12]) and total years of baseball experience (OR, 1.02 [95% CI, 1-1.04]) (Table 3). Moreover, excluding players with RCTs on the bilateral sides, the total years of baseball experience (OR, 1.03 [95% CI, 1-1.05]) and frequency of participation per week (OR, 1.40 [95% CI, 1.04-1.89]) were significantly associated with RCTs on the throwing side (Table 4). The presence of RCTs on the nonthrowing side was not significantly associated with the independent variables. Multicollinearity assessment revealed no correlation coefficients exceeding R2 >0.4 among the independent variables.
Independent Factors Associated With RCTs on the Throwing Side a

Bold values indicate statistical significance at P < .05. OR, odds ratio; RCTs, rotator cuff tears.
Independent Factors Associated with RCTs on the Throwing Side and the Nonthrowing Side, Excluding Those With RCTs on the Bilateral Sides a

Bold value indicates statistical significance at P < .05. OR, odds ratio. RCTs, rotator cuff tears.
Discussion
In this study, we examined the prevalence and associated factors of RCTs in older baseball players. Ultrasonographic evaluation revealed that, overall, 37.7% RCTs were observed, which is comparable to previously reported rates of 15.2% to 50% in the general older population.24,39 Thus, the prevalence of RCTs in older baseball players may not be significantly higher than that in the general older population. Notably, 26.5% of participants had RCTs in the throwing shoulder, with two-thirds of the cases being asymptomatic. Symptom prevalence was comparable between groups regardless of RCT status, suggesting that symptoms alone are not a reliable indicator for identifying the RCTs. Increasing age and total years of baseball experience were significantly associated with RCTs in the throwing shoulder. When participants with bilateral RCTs were excluded, total years of baseball experience and the frequency of weekly participation emerged as significant factors. However, the ORs were small across variables (OR, 1.02-1.40), suggesting limited clinical significance. Overall, while RCTs are common, their prevalence in older baseball players does not appear markedly higher than in the general older population, and many individuals continue to play without symptoms.
Generally, aging is the most significant risk factor for RCTs in the older population, as it causes impaired blood flow to the rotator cuff, thinning of the collagen fibers at the attachment site, and a decrease in mechanical strength due to degeneration.12,20,34,38 Given the repetitive overhead motions and mechanical stress associated with baseball, it was expected that older baseball players would have a higher prevalence of RCTs. However, our findings showed that the prevalence of RCTs in older baseball players was 37.7% overall and 26.5% in the throwing shoulder. Previous studies have reported that the prevalence of RCTs is higher in community-dwelling older adults and increases with age. Minagawa et al 24 reported that the prevalence of RCTs in older adults aged 60 to 80 years ranged from 15.2% to 36.6%, and Yamamoto et al 39 reported a prevalence of 25.6% to 50%. In short, the prevalence of RCTs in this population was similar to that reported in previous studies of the same age group. McMahon et al 23 reported a prevalence of 21.3% in nonoverhead athletes aged 60 to 84 years who participated in the Senior Olympics, while Harada et al 10 reported a 35% prevalence of RCTs in the dominant arm of older tennis players aged 60 to 77 years. Similar to the studies by McMahon et al 23 and Harada et al, 10 our study focused on an active older population, who may exhibit higher physical function compared with the general older population. These findings suggest that participation in baseball does not negatively affect RCT prevalence in older players.
Furthermore, our findings showed that 66.7% of RCTs were asymptomatic, suggesting that many participants with RCTs can continue to participate in baseball without significant impairment. Previous studies have shown that the rate of asymptomatic RCTs ranges from 60% to 70% in active and general older populations.10,23,24 It has been suggested that upper extremity use and activity levels were not significantly related to tear size or progression rates.16,18,40 This reinforces the idea that, despite the high load placed on the shoulder joints in baseball, repetitive pitching motions may not be associated with progression or symptoms. In addition, the Kanagawa Over–60 Rubber Baseball Association, to which the players in this study belong, has modified the game rules to reduce physical strain. Specifically, the pitching and base distances have been shortened by 2 m compared with those in standard baseball regulations, and each game is limited to 7 innings, thereby decreasing the load on the shoulder joint during pitching and the total pitch count. Using rubber balls (138 g), which are slightly lighter than standard hardballs (142 g), may also help reduce the mechanical load on the shoulder joint. The findings of this study suggest that modifying game rules can enable older individuals to continue participating in baseball sustainably while minimizing excessive strain on the shoulder joint. In contrast, this finding appears inconsistent with the current results, which indicate that a long history of baseball participation was associated with RCTs. Nonetheless, the low OR of 1.02 suggests that its impact on RCTs occurrence is minimal.
When bilateral RCTs were excluded, a higher frequency of baseball participation was associated with RCTs, suggesting that an increased frequency of play may elevate the risk of RCTs. Nevertheless, since the prevalence of RCTs did not differ between the throwing and nonthrowing sides, playing baseball itself does not appear to be inherently harmful or initiate the onset of RCTs. Indeed, participants in this study also demonstrated lower prevalence rates of hypertension and diabetes compared with those of the general older population, in which these rates are approximately 60% to 70% and 20%, respectively. 25 Therefore, while maintaining baseball participation at a moderate frequency may contribute positively to overall health in this population, caution should be taken to avoid excessive play, given the potential increased risk of RCTs.
Notably, the prevalence of symptoms was similar regardless of RCT status. A longitudinal cohort study of patients aged ≥45 years with shoulder pain reported that 61.3% (163 of 266) had RCTs. 9 These findings indicate that while health care providers should recognize the high likelihood of RCTs in older patients presenting with shoulder pain, pain alone is not a reliable screening marker for detecting RCTs in older individuals engaged in sports requiring extensive shoulder use, such as baseball. Clinical symptoms associated with RCTs include pain, restricted range of motion, muscle weakness, and narrowing of the acromiohumeral distance.19,26,37 Future studies should prospectively evaluate the relationships between such objective measures and the presence of RCTs in older baseball players.
The primary treatments for RCTs include conservative treatments, such as physical therapy, and surgical treatments, such as rotator cuff repair. There is no difference in clinical outcomes between the 2 treatment methods in the short term (2-3 years); however, surgical treatment is reportedly superior to conservative treatment in the long term (≥5 years).27-30 Therefore, early detection and appropriate treatment of RCTs, regardless of symptoms, are essential for maintaining long-term sports participation in older adults. However, it remains unclear whether these previous findings can be directly applied to older adults who consistently engage in moderate shoulder exercise, such as baseball, as observed in the present study. Ultrasonography is beneficial for the early detection of RCTs. However, further research is warranted to better clarify the limitations of conservative treatment and indications for surgical intervention in older baseball players with RCTs.
Limitations
This study has some limitations. First, only older persons who can currently play baseball were included. Therefore, those unable to play owing to symptoms or underlying conditions may have been systematically excluded, leading to selection bias. Thus, current findings may not be fully generalizable to the broader population of older baseball players. Moreover, because rubber baseballs were used and rule modifications were specific to this association, the findings may not be generalizable to older adults participating in standard baseball using hardballs. Second, data collection relied on self-reported injuries from the past year, which may introduce recall bias. Third, bone morphology factors, such as the critical shoulder angle, were not assessed despite their association with RCTs. Fourth, the use of ultrasonography limited the evaluation of tear quality— including size and fatty degeneration. Consequently, the findings of this study should be interpreted with caution. On the other hand, the ultrasonography used to assess RCTs in this study is cost-effective and easy to use, offering particular advantages in detecting asymptomatic RCTs without needing a visit to a medical institution.
This is the first report to examine the relationship between the prevalence of RCTs and shoulder complaints in older adults participating in competitive baseball. Understanding the pathophysiology of shoulder complaints in older adults is crucial for them to enjoy baseball in the long term. Further research is needed to develop strategies that support continued sports activities among older adults despite RCTs.
Conclusion
Our findings show that approximately 26.5% of older baseball players had RCTs in their throwing shoulder, with 66.7% being asymptomatic. The prevalence on the nonthrowing side was 22.3%. These findings suggest that participation in baseball is unlikely to induce excessive RCTs or shoulder pain. Age was the most relevant factor associated with RCTs on the throwing shoulder. Conversely, when those with bilateral RCTs were excluded, a high frequency of participation was more strongly related to the presence of RCTs than was age. Furthermore, no significant difference was observed in symptom prevalence between players with and without RCTs, indicating that symptom monitoring is not a reliable approach for identifying RCTs in this population.
Footnotes
Appendix
Prevalence of Throwing Side RCTs by Position a

| With RCTs Group | Without RCTs Group | |
|---|---|---|
| Pitcher, n= 46 | 15 (32.6) | 31 (67.9) |
| Catcher, n = 20 | 5 (25) | 15 (75) |
| Infielders, n = 118 | 31 (26.3) | 87 (73.4) |
| Outfielders, n = 69 | 16 (23.2) | 53 (76.8) |
| Designated Hitter, n = 7 | 2 (28.6) | 5 (71.4) |
Data are presented as n (%). RCTs, rotator cuff tears.
Acknowledgements
All data were collected from the Kanagawa Over 60 Rubber Baseball Association. The authors thank the association's officials, players, and staff for their support in collecting the data.
Final revision submitted October 5, 2025; accepted October 14, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Written informed consent was obtained from all participants. The Research Ethics Committee of the Faculty of Medicine, Juntendo University, approved this study protocol.