
Abstract
Background:
While surgical interventions for ulnar collateral ligament (UCL) injuries in throwing athletes have improved return-to-sport rates, predicting individual recovery timelines and the risk of complications remains a challenge. The influence of a patient's preoperative status, captured through patient-reported outcomes (PROs), on postoperative recovery milestones and complication risks is not well-defined.
Purpose/Hypothesis:
The purpose of this study was to determine if baseline PROs and specific surgical variables predict critical postoperative milestones and adverse outcomes following UCL surgery. It was hypothesized that better baseline PROs would be associated with improved postoperative outcomes.
Study Design:
Cohort study: Level of evidence, 3.
Methods:
Data for this study were obtained from The Pitch Registry, a multi-institutional database of baseball players with UCL injuries, analysis conducted between 2019 and 2023. Of 506 screened patients, 146 were included based on having ≥2 years of follow-up and complete preoperative PROs. Baseline PROs, including the American Shoulder and Elbow Surgeons (ASES) score, Kerlan-Jobe Orthopaedic Clinic (KJOC) score, and Youth Throwing Score (YTS), were collected. Postoperative outcomes, including time to return to throwing (RTT) and return to mound (RTM), and the presence of surgical complications, were documented. Intraoperative variables, such as the type of UCL procedure (repair or reconstruction), were also recorded.
Results:
A total of 146 patients were included for analysis, and their surgical breakdown included 39 (26.7%) repairs, 69 (47.3%) palmaris reconstructions, and 38 (26.0%) gracilis reconstructions. Reported level of play included high school (30%), college (56%), minor league professional (10%), and major league professional (1%). Better baseline total ASES scores were significantly associated with a faster RTT (coefficient −0.09 weeks/point; P = .003) and decreased odds of postoperative complications (odds ratio [OR] 0.97; 95% CI, 0.94-0.99; P = .01). Worse baseline ASES intensity of pain scores significantly predicted longer RTT (coefficient 0.5 weeks/point; P = .01) and increased odds of complications (OR, 1.3; P = .005), revision surgery (OR, 1.3; P = .04), and ulnar nerve symptoms (OR, 1.2; P = .04). The repair group demonstrated significantly shorter RTT (mean, 14.8 weeks) and RTM (mean 31.7 weeks) compared with both palmaris (RTT: 18.9 weeks, P < .001; RTM: 41.7 weeks, P < .001) and gracilis groups (RTT: 22.4 weeks, P < .001; RTM: 42.1 weeks, P < .001). No significant differences were found in complication, reoperation, or ulnar nerve symptom rates among the surgical groups (repair vs palmaris vs gracilis). Other PROs (KJOC, YTS) and surgical variables (ulnar nerve transposition, scope) did not consistently predict these outcomes.
Conclusion:
Better baseline PROs, particularly better total ASES scores and better ASES intensity of pain scores, are associated with faster RTT and a reduced risk of postoperative complications and adverse events following UCL surgery. UCL repair was associated with significantly faster RTT and RTM timelines compared to reconstruction with either palmaris or gracilis autografts. These findings suggest that specific preoperative PROs can aid surgeons in managing patient expectations and counseling regarding postoperative recovery.
Keywords
The escalating incidence of ulnar collateral ligament (UCL) injuries among throwing athletes,3,6,7,20,25,27 particularly in baseball, presents a significant challenge across all levels of play—from youth players,17,25 to college athletes, 12 to Major League Baseball (MLB) professionals.5,9 While surgical interventions for UCL tears have seen considerable advancement10,21,31 since the pioneering work of Dr. Frank Jobe, 23 leading to generally high rates of return to sport,4,13,15,26 the recovery pathway remains arduous and variable. Athletes often face prolonged rehabilitation periods,4,14,16,18,22,28,29 with critical milestones such as the initiation of rehabilitation throwing programs dictating the overall recovery timeline, 1 which can extend to a year or more. 6 Furthermore, the preoperative prediction of individual patient recovery trajectories, the likelihood of achieving preinjury performance levels,4,14,16,22,24 and the risk of postoperative complications remains a complex endeavor. Prior studies investigating surgical technique and reconstruction type have failed to identify consistent predictors of return to sport, further highlighting the gap in knowledge for predicting recovery.19,34
Patient-reported outcomes (PROs) are increasingly recognized for their value in capturing a patient's preoperative status and potentially reflecting factors beyond simple injury mechanics, such as their overall well-being or perspective on their condition, which may influence recovery.2,8,30,32,33 Identifying which specific PROs, or their subcomponents, might correlate with or predict critical postoperative outcomes could significantly enhance clinical decision-making. Such insights would empower surgeons to set more accurate expectations, tailor rehabilitation strategies, and provide more individualized counsel to patients regarding their anticipated recovery and potential risks.
This study, therefore, aimed to investigate the relationship between various preoperative PROs and subsequent postoperative milestones. We sought to determine if these baseline PROs, along with specific surgical variables (UCL repair or reconstruction, concomitant ulnar nerve transposition, and arthroscopic debridement), could predict the time to initiation of throwing programs, as well as the incidence of postoperative complications, reoperations, and ulnar nerve symptoms. We hypothesize that better baseline PROs will predict improved postoperative outcomes. The ultimate goal is to provide clinicians with evidence-based factors that can aid in optimizing patient counseling and managing expectations following UCL surgery.
Methods
Study Design
Data for this study were sourced from The Pitch Registry, a multi-institutional, prospectively maintained database of baseball players with UCL injuries, which is hosted by MLB. Our study was conducted in accordance with approval from the Columbia University Medical Center institutional review board.
Data Collection
The Pitch Registry receives contributions and is maintained by participating investigators from Columbia University, MLB, Rothman Orthopaedic Institute, Cleveland Clinic, UCHealth Steadman Hawkins Clinic, and Vanderbilt University Medical Center. It is hosted by MLB as a collaborative effort. The database exclusively features baseball players, encompassing all levels of play from Little League through major league professionals. The data utilized for this study included players aged 13 to 39. Data were collected prospectively, encompassing preoperative, intraoperative, and postoperative time points. Patients were followed longitudinally through numerous postoperative visits and throughout their interaction with the health system.
Preoperatively, patient demographics and PROs were collected. PROs included the American Shoulder and Elbow Surgeons (ASES) Standardized Shoulder Assessment Form, Kerlan-Jobe Orthopaedic Clinic (KJOC) score, and Youth Throwing Score (YTS). While The Pitch Registry contains numerous intraoperative variables, those selected for this study included the type of UCL procedure (repair, reconstruction with palmaris autograft, or reconstruction with gracilis autograft), concomitant ulnar nerve transposition, and any associated arthroscopic debridement. For analysis, patients were categorized into 3 surgical groups: the repair group (UCL repair alone), the gracilis group (UCL reconstruction with gracilis autograft), and the palmaris group (UCL reconstruction with palmaris autograft). The treating surgeon (C.A.) determined the surgical method. If the UCL was suitable for repair, a repair was performed. For reconstructions, a palmaris autograft was the standard, but a gracilis autograft was used if the palmaris was unavailable. There were no specific exclusion criteria; all operatively managed UCL injuries were eligible for inclusion.
Patients were included if they met the following criteria: (1) underwent surgical UCL management between January 2019 and April 2023, allowing for a 2-year postoperative follow-up assessment period (though not requiring an office visit at 2 years for inclusion); and (2) had complete baseline PROs (ASES, KJOC, and YTS scores). Follow-up documentation including return-to-throwing (RTT) and return-to-mound (RTM) dates were also recorded. Surgical complications were identified from The Pitch Registry and supplemented by a review of the electronic health record for any additional relevant hospitalizations or office visits that also represented postoperative complications. The determination for initiating a throwing program and advancing to mound throwing was made by the treating surgeon and physical therapist (F.A.) based on their clinical judgment of the patient's progress and readiness. Although all 146 players were included in this analysis, pitchers comprised 128 of these players, according to their self-reported primary position. The majority of patients not included in analysis for this study within The Pitch Registry were because of incomplete data.
Complications occurring at any postoperative time point were documented. Ulnar nerve–related postoperative complications were categorized as temporary/minor ulnar nerve symptoms (sensory only, lasting <1 week) or significant ulnar nerve symptoms (lasting >1 week or requiring revision surgery, such as an ulnar nerve transposition). A “scope for loose body” was documented if a patient underwent postoperative arthroscopy for a previously unidentified loose body. Flexor tendon strain was defined based on clinical diagnosis and/or magnetic resonance imaging (MRI) findings. UCL-related postoperative complications included partial retear (postoperative MRI signal change without an identifiable tear, not requiring revision surgery) and full retear (MRI findings of a complete UCL retear requiring revision surgery).
Timelines for RTT and RTM were documented and initiated based on the clinical evaluation of each patient's recovery and readiness. Prior to initiating either RTT or RTM, patients were screened by the physical therapist to confirm readiness for throwing. The standard flat ground throwing program, initiated at the RTT milestone, spanned 18 weeks. All players underwent the same rehabilitation protocol.
Statistical Analysis
Statistical analysis was conducted using MATLAB (Version R2025b; MathWorks) and Microsoft Excel (Microsoft Corp). The choice of statistical test was dependent on the nature of the variables being analyzed. A P value <.05 was considered statistically significant for all analyses.
Pearson correlation coefficients were used to assess interrelationships between baseline PRO scores. Multivariable linear regression models were used to examine the relationship between baseline PROs (or surgical factors) and continuous outcomes such as RTT and RTM timelines. For comparing baseline PROs (such as KJOC, ASES, or YTS scores) across the 3 surgical groups, 1-way analysis of variance (ANOVA) was used when assumptions of normality and homogeneity of variances were met; otherwise, the Kruskal-Wallis H test was employed. When comparing RTT and RTM timelines across these surgical groups, because of violations of parametric assumptions, Kruskal-Wallis H tests were utilized, followed by pairwise Mann-Whitney U tests with Bonferroni correction for post hoc analysis where significant overall differences were found. Logistic regression was used for analyses with binary outcomes, such as complications, ulnar nerve symptoms, and revision surgery. Associations between categorical variables, such as surgical group and the incidence of postoperative complications, were assessed using chi-square tests of independence or Fisher exact tests where appropriate. The specific statistical test conducted is reported with each finding.
Results
Demographics
A total of 506 patients from The Pitch Registry were screened for inclusion, of whom 146 were selected based on the inclusion criteria outlined in the Methods section. A total of 360 of 506 patients (71.1%) were excluded from this study. The primary reasons for exclusion were inadequate follow-up (n = 299; 83%), insufficient baseline data (n = 40; 11%), and incomplete surgical data (n = 22; 6%) (Figure 1). The mean age of participants was 19.9 years. Detailed baseline demographics and a surgical breakdown are presented in Table 1.
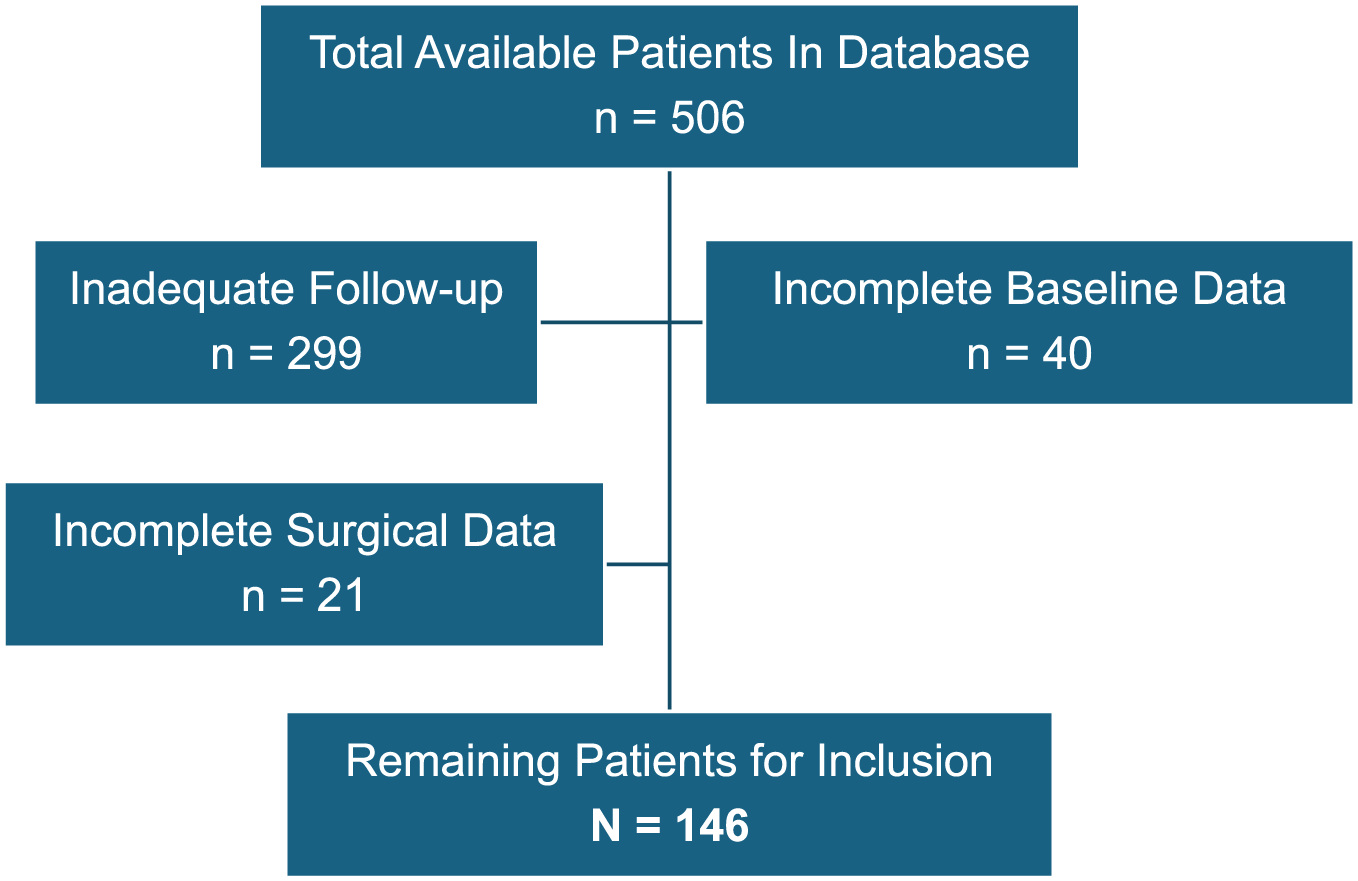
Flowchart illustrating the reasons for exclusion from analysis.
Baseline Patient Demographics for All Patients Included in Analysis (N = 146) a

Data are reported as mean ± SD or n (%).
Comparing Baseline PROs Among Repair, Gracilis, and Palmaris Groups
Baseline PROs were analyzed and compared among the 3 surgical groups: repair, palmaris, and gracilis. Table 2 presents the baseline PRO findings. The repair, palmaris, and gracilis groups showed no significant differences with respect to their baseline KJOC scores (ANOVA F = 0.558; P = .57) or YTS scores (ANOVA F = 0.165; P = .85). For the baseline ASES score, an overall Kruskal-Wallis H test indicated no statistically significant difference among the groups (H = 3.850; P = .15); however, a direct pairwise comparison of baseline ASES scores revealed that the repair group had significantly higher scores (mean, 78.25) than the palmaris group (mean, 70.87; Mann-Whitney U = 1023.5; P = .04).
Mean Baseline PROs for All Patients and Repair, Palmaris, and Gracilis Subgroups a

ASES, American Shoulder and Elbow Surgeons; KJOC, Kerlan-Jobe Orthopaedic Clinic; PRO, patient-reported outcome; YTS, Youth Throwing Score.
Kruskal-Wallis H test.
One-way analysis of variance.
Indicates significance between values P < .05 (Mann-Whitney U test).
Baseline ASES scores showed a significant positive correlation with YTS scores (Pearson r = 0.289; P < .001), while YTS scores also demonstrated a significant positive correlation with KJOC scores (Pearson r = 0.323; P < .001); however, the correlation between ASES and KJOC scores was not statistically significant (r = 0.141; P = .09).
Predicting Postoperative Complications
The overall rates of complication and reoperation, along with their subcategorizations, are depicted in Table 3. The overall complication rate was 13.7%, and the reoperation rate was 5.5%. There was no statistically significant difference in postoperative complication rates among the repair (n = 3; 7.69%), palmaris (n = 9; 13.04%), and gracilis (n = 8; 21.05%) surgical groups (χ2(2) = 2.954; P = .23). Additionally, no significant differences were found among the repair, palmaris, and gracilis groups with respect to reoperation rates (χ2(2) = 0.026; P = .99) or postoperative ulnar nerve symptoms (χ2(2) = 2.284; P = .32).
Total Complication and Reoperation Rate, With Subcategories (N = 146) a

UCL, ulnar collateral ligament.
In a multivariable logistic regression analysis (LRR) examining the association between baseline PROs and postoperative complications (n = 146; 20 events), higher baseline ASES scores were found to be significantly associated with decreased odds of complications (odds ratio [OR], 0.97; 95% CI, 0.94-0.99; P = .01), whereas baseline YTS and KJOC scores were not significant predictors in this model. Surgical variables, including UCL procedure type (repair/palmaris/gracilis), the presence of an ulnar nerve transposition, or an arthroscopic debridement, did not significantly predict the rate of complications (LRR, P = .42).
Notably, for the cohort as a whole, when examining the ASES intensity of pain subscore, worse baseline pain intensity significantly predicted a longer time to RTT (coefficient = 0.53; P = .01). Additionally, worse baseline ASES intensity of pain was associated with increased odds of postoperative complications (OR, 1.29; 95% CI, 1.08-1.54; P = .005), revision surgery (OR, 1.33; 95% CI, 1.02-1.74; P = .04), and postoperative ulnar nerve symptoms (OR, 1.24, 95% CI, 1.02-1.53; P = .04). Baseline ASES intensity of pain did not significantly differ among the repair, palmaris, and gracilis groups (Kruskal-Wallis H test; P = .57).
Predicting RTT and RTM Timelines
The mean time to RTT for all patients was 18.7 weeks, and the mean time to RTM was 38.9 weeks, as detailed in Table 4. A Kruskal-Wallis H test revealed a statistically significant difference in RTT among the repair, palmaris, and gracilis groups (H = 47.009; P < .001). Post hoc Mann-Whitney U tests with Bonferroni correction revealed that the repair group had a significantly shorter RTT compared with both the palmaris (P < .001) and the gracilis (P < .001) groups, while no significant difference was observed between the palmaris and gracilis groups (P = .07). When examining RTM, a Kruskal-Wallis H test indicated a statistically significant difference in RTM among the repair, palmaris, and gracilis groups (H = 35.370; P < .001). Post hoc Mann-Whitney U tests with Bonferroni correction revealed that the repair group had a significantly shorter RTM compared with both the palmaris (P < .001) and the gracilis (P < .001) groups; no significant difference in RTM time was observed between the palmaris and gracilis groups (P = .26).
Mean Times for Initiating RTT and RTM Program for All Patients and Repair, Palmaris, and Gracilis Subgroups a

Data are reported as mean ± SD. RTM, return to mound; RTT, return to throwing.
Designations a, b, c, and d represent significance between the 2 values with the same letter (P < .05, Mann-Whitney U test).
A multivariable linear regression analysis evaluating the association of baseline PROs with RTT revealed that better baseline ASES scores were significantly associated with a shorter RTT (coefficient −0.09; P = .003), while baseline YTS and KJOC scores (both P > .5) were not significant predictors in the model (overall model R2 = 0.084; F(3,130) = 3.966; P = .01). No baseline PROs significantly predicted RTM in a separate multivariable linear regression analysis (R2 = 0.021; F(3,85) = 0.594; P = .62). Neither an ulnar nerve transposition nor an arthroscopic debridement during the index surgery was a significant predictor of RTT or RTM (all P > .05).
Discussion
This study is among the first to demonstrate that preoperative PROs predict not only the time to important postoperative milestones, including RTT programs, but also the risk of experiencing postoperative complications. Additionally, it was identified that worse baseline ASES intensity of pain scores were associated with increased odds of experiencing a postoperative complication, revision surgery, and ulnar nerve symptoms, as well as longer RTT timelines. Finally, we identified how the utility of practical and widespread PROs can vary when predicting outcomes among important UCL surgical subgroups, including UCL repairs and UCL reconstructions with either a palmaris or a gracilis autograft.
Interpreting how better baseline ASES scores correlate with quicker RTT and lower complications requires an understanding of the player and his specific injury. While an obvious interpretation of the data could suggest that a better starting point (ie, a higher or more favorable baseline ASES score) leads to superior outcomes (shorter RTT, fewer complications) simply due to this initial advantage, we would argue for a more nuanced explanation. Numerous publications have previously outlined how a preoperative patient mindset, which can be reflected in PROs, can affect orthopaedic outcomes in teens and young adults following orthopaedic procedures such as hip preservation,30,32 spine surgery, 8 total hip arthroplasty, 2 and anterior cruciate ligament reconstruction. 33 For our patients, the variability in each player's unique UCL injury was relatively narrow considering the specificity of players included in this study (isolated UCL tear). Given this, while pain is subjective and can certainly vary among patients, their baseline injury severity was therefore considered relatively consistent across the cohort. Thus, it is possible that the variation observed in baseline PROs, and the ASES pain intensity in particular, reflected not only their perceived pain and function but also the patient's mindset regarding his injury. Within this interpretive lens, whereby worse baseline PROs represented not only worse pain/function but also a more negative mindset or preoperative perspective, our findings are consistent with those of other studies suggesting that a more negative preoperative mindset portends worse outcomes, potentially due to its influence on patient expectations.
The predictive value of the ASES score is underscored by the finding that it was the sole variable associated with RTT timelines, complications, revision surgeries, and ulnar nerve symptoms, whereas no surgical factors were. While the individual occurrences of complications, ulnar nerve symptoms, and revision surgeries were low, the type of procedure (repair vs reconstruction) was not associated with any of these outcomes. It is reasonable to assume that complication rates may be greater in reconstruction than repair given the surgical complexity. 11 However, this assumption would not invalidate our finding that baseline PROs affect outcomes.
Using baseline PROs, with the ASES and its pain intensity subscore being of particular importance in players with a UCL injury, surgeons are better equipped to manage expectations, predict timelines, and counsel patients on complications. It was interesting to note that during the Pearson correlation analysis, the ASES, YTS, and KJOC scores showed varied intercorrelations, with some not being strongly associated with each other. This suggests some PRO questionnaires may offer more predictive value than others. For example, while the ASES provided significant predictive value for multiple outcomes in this study, the YTS and KJOC PROs did not.
The descriptive findings regarding timing of RTT programs (both flat ground and mound) also provide additional value to this study. This represents a direct comparison using a unified study cohort that allows head-to-head analysis of throwing milestones in UCL repair and reconstruction patients. This enables surgeons to provide more accurate recommendations and a better understanding of the postoperative course. It is not surprising that the repair cohort returned to throwing earlier, as this is allowed for in the postoperative protocol compared with reconstructions.
Clinically, these ASES findings are highly relevant. For every 1-point increase in the baseline total ASES score, the time to RTT was significantly shorter by 0.09 weeks. Moreover, each point indicating worse baseline ASES intensity of pain was associated with a 0.53-week longer RTT and elevated odds of postoperative complications (OR, 1.29), revision surgery (OR, 1.33), and ulnar nerve symptoms (OR, 1.24). These associations underscore that patients presenting with lower baseline ASES scores, particularly those reporting higher pain intensity, warrant comprehensive counseling regarding potentially prolonged recovery timelines and heightened risk of adverse events.
Limitations
This study is not without its limitations. First, the number of complications was relatively low. This low event number can generate relatively wide confidence intervals and demands close attention to statistical analysis and the interpretation of significance. We employed appropriate statistical methods to account for these factors where possible. Second, while the surgical procedure type was categorized as repair, palmaris, and gracilis, there may have been small nuances in the procedures being performed. These slight differences (ie, which suture type being used) are unlikely to represent any clinically meaningful difference, but they are worth mentioning. Third, we did not perform subgroup analyses based on level of play (high school, college, or professional) for RTT, RTM, or complication rates. However, as the majority of our cohort consists of high school and college players, the generalizability of the overall findings remains sound for this primary demographic. Finally, while prospective in nature, this is still an observational study and comes with its inherent limitations.
Conclusion
Better preoperative PROs, particularly higher ASES scores, were correlated with a faster initiation of RTT programs and a reduced risk of postoperative complications. Patients with better baseline ASES intensity of pain scores had reduced odds of experiencing a postoperative complication, revision surgery, and ulnar nerve symptoms, as well as faster RTT timelines. Finally, this study identified significant differences in timelines for the initiation of throwing programs (RTT and RTM) among UCL surgical subgroups (repairs vs reconstructions), with repairs demonstrating significantly faster progression as expected.
Footnotes
Final revision submitted October 7, 2025; accepted October 9, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
This study received approval from the Columbia University Medical Center institutional review board (protocol No. IRB-AAAV6636).