
Abstract
Background:
Femoroacetabular impingement (FAI) is a common injury experienced by basketball players. Surgical management with arthroscopic labral repair and femoral osteochondroplasty can lead to successful outcomes for athletes whose nonoperative management fails. Recent studies have demonstrated that athletes undergoing hip arthroscopy in the setting of FAI had favorable return-to-sport (RTS) and sport continuation outcomes.
Purpose:
To evaluate patient-reported outcome measures (PROMs) and RTS rates at minimum 5-year follow-up in basketball players after hip arthroscopy for FAI.
Study Design:
Case series; Level of evidence, 4.
Methods:
All active basketball players at the recreational, high school, and collegiate levels who underwent primary hip arthroscopy with labral repair for FAI between August 2009 and December 2019 were identified. Postoperative RTS, revision rates, and surgery satisfaction at final follow-up were evaluated. PROMs were also analyzed as follows: visual analog scale, Tegner Activity Scale, modified Harris Hip Score, Hip Outcome Score–Activities of Daily Living, and Hip Outcome Score–Sport.
Results:
Fifty-three patients (64 hips) were included with a mean ± SD age of 21.2 ± 6.0 years. Most athletes played recreational or high school basketball (85%), while 15% played college basketball. Forty-three patients attempted to return to basketball. Of these patients, 35 (81%) returned to basketball after surgery, with 32 (91%) returning to the same level of play. Patients who returned to basketball had significantly improved outcomes on the modified Harris Hip Score (P = .006), Hip Outcome Score–Activities of Daily Living (P = .007), Hip Outcome Score–Sport (P = .004), Tegner Activity Scale (P = .010), and visual analog scale with use (P = .041) as compared with those who did not return. High school athletes had decreased odds of RTS when compared with recreational athletes (P = .01). There was significant improvement in all PROMs from baseline to minimum 5-year follow-up (P < .05).
Conclusion:
At minimum 5-year follow-up, basketball players demonstrated durable improvements in PROMs and an RTS rate of 81% after hip arthroscopy for FAI. The majority of athletes returned to the same level of competition. There were significantly improved PROMs in patients who returned to sport versus those who did not. High school athletes had decreased odds of RTS when compared with recreational athletes. However, body mass index, sex, age, alpha angle, and basketball position did not significantly correlate with RTS outcomes.
Femoroacetabular impingement (FAI) is well documented to occur in a young, athletic patient population. Efforts have been made to classify hip pathology across various athletic populations in that different sports place different biomechanical stress on the joint. 14 Basketball athletes engage in cutting, pivoting, sprinting, and jumping motions and are susceptible to FAI.14,18 Notably, basketball players are part of the subset of athletes who face up to a 4-fold increased risk of cam deformity as compared with nonathletes.1-3,7 Hip arthroscopy is the gold standard for the treatment of symptomatic FAI, when patients have failed comprehensive nonoperative measures.
Hip arthroscopy in the setting of FAI has shown favorable outcomes in the literature, with excellent return-to-sport (RTS) outcomes and successful patient-reported outcome measures (PROMs), making it a feasible treatment option for athletes.12,13,16 In basketball players specifically, hip arthroscopy has been studied in smaller cohorts of athletes with reproducible data suggesting that they have high RTS rates and good PROMs postoperatively.4,5,9,15,17 Begly et al 4 studied 18 professional basketball players. The athletes demonstrated a 100% RTS with a mean time to return of 7 months, while Jack et al 8 studied 23 professional basketball players and reported an 87.5% RTS with a mean time of 6.7 months. Despite these reassuring data, there are limited data on midterm outcomes for basketball players at varying levels of competition and with larger cohorts of athletes. Furthermore, there have been efforts to classify variables associated with favorable outcomes after hip arthroscopy for FAI, with one systematic review finding that younger age, male sex, lower body mass index (BMI), Tonnis grade 0, and pain relief from preoperative hip injection were associated with positive outcomes after surgery. 19 Such analysis into preoperative variables that could correlate with postoperative outcomes has not been studied in basketball players.
The purpose of our study was to evaluate midterm outcomes of hip arthroscopy in basketball players with symptomatic FAI in a moderately sized cohort. Specifically, we sought to measure the durability of PROMs, RTS rates, correlation of preoperative demographic data with achieving RTS, and sport continuation at a minimum 5-year follow-up. We hypothesized that basketball athletes would have favorable durability of PROMs and good RTS rates and that there would be no correlation between preoperative demographic data and RTS outcomes.
Methods
Following approval of the institutional review board, a retrospective review of a prospectively collected clinical database from a single institution was conducted to identify all patients who underwent primary hip arthroscopy between August 2009 and December 2019. Inclusion criteria consisted of patients who played basketball at the time of surgery, underwent primary hip arthroscopy for FAI, and intended to RTS after surgery. Exclusion criteria consisted of <5-year follow-up, insufficient basketball documentation in the patient's medical record, or patient declination to participate (Figure 1).

CONSORT diagram of patients returning to basketball after hip scope for femoroacetabular impingement. PROM, patient-reported outcome measure.
Patient medical records were individually reviewed to obtain demographics (age, sex, BMI, basketball participation), preoperative radiographic measurements (Tonnis grade, lateral center-edge angle [LCEA], alpha angle), and preoperative PROMs. Surgical details were also obtained (labral repair, capsulotomy, capsular repair, cam resection) as well as postoperative data (need for revision, RTS, PROMs).
Patients were contacted at minimum 5-year follow-up, when necessary, via telephone. RTS data included player position, current participation in basketball, and level of play. PROMs consisted of modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sport (HOS-Sport), Tegner activity level, visual analog scale (VAS) at rest and with use, 5-point VAS, and 10-point surgery satisfaction scale.
Surgical Technique
Patients were positioned on a modified traction table with distraction of the operative hip. Standard anterolateral and midanterior portals were created in all cases. On a case-by-case basis, additional distal anterolateral or posterolateral portals were created. All patients underwent diagnostic arthroscopy with intraoperative grading of chondromalacia and chondrolabral delamination. Characteristics of surgical procedures performed include labral repair, capsulotomy, femoroplasty, acetabuloplasty, and capsular repair (Table 1). Labral repair with arthroscopic suture anchor placement was performed for all included patients. Patients underwent a T-capsulotomy or interportal capsulotomy as well as femoroplasty and/or acetabuloplasty per surgeon preference. Fifty-one patients (96%) underwent capsular repair and closure. Capsular repair was not performed in all patients owing to surgeon preference and the inclusion of patients since 2009, when it was less routinely performed.
Patient Demographics of Basketball Players a

Bold indicates P < .05.
Laterality total includes patients who had bilateral surgery.
Statistical Analysis
Data were collected and stored utilizing Microsoft Excel and REDCap (REDCap Consortium) software. Data were analyzed in R Studio (R Core Team). Baseline patient characteristics were presented as mean and percentage with standard deviation or 95% confidence interval (95% CI) when appropriate. Pre- and postoperative data were analyzed for parametric/nonparametric assumptions utilizing Shapiro-Wilk normality tests. Continuous variables were then analyzed by Student t tests or Mann-Whitney U tests. Categorical variables were analyzed via χ2 analysis when appropriate. Predictors of RTS outcomes were analyzed with a logistic regression model using the generalized linear model function in R, and odds ratios and 95% CIs were generated. Statistical significance was defined as P < .05.
Results
Patient Demographics
A total of 1925 patients underwent primary hip arthroscopy between August 2009 and December 2019 at a single institution. Of these, 53 patients (64 hips) were included and eligible for 5-year follow-up following inclusion/exclusion criteria. A total of 28 males (53%) were included, and the mean age of the cohort was 21.2 ± 6.0 years with a mean BMI of 27.3 ± 6.3 kg/m2 (Table 1). Most athletes played recreational (34%) or high school (51%) basketball, while 15% played basketball in college. The guard position was the most common position affected (54%). The cohort had a mean preoperative LCEA of 30.5°± 5.4°, Tonnis angle of 5.3°± 4.1°, and alpha angle of 59.7°± 10.4°. Thirty-three patients (62%) had a Tonnis grade of 0; 18 (34%), a Tonnis grade of 1; and 2 (4%), a Tonnis grade of 2. All patients underwent a capsulotomy for capsular management, with interportal capsulotomies (60%) being more common than T-capsulotomies (40%). Forty-eight patients (91%) underwent a femoroplasty and 38 (72%) an acetabuloplasty. Capsular repair was performed in 51 patients (96%).
Return to Basketball
RTS data were available for all 53 patients, with 35 (66%) returning to basketball and 19 not returning. Of the 19 patients who did not return, 10 cited graduating, priorities changing, or other nonmedical reasons and were excluded from further analysis. Therefore, 43 patients attempted to RTS. Of these, 35 patients (81%) returned to basketball after their primary hip arthroscopy, with 32 (91%) returning at the same level at which they were playing before surgery (Table 2). Nine patients were still actively playing basketball at final follow-up. Of the 8 patients who attempted to return but did not, 7 did not return because of hip limitations, and 1 sustained an additional injury. Of the 7 patients who did not return owing to hip limitations, 3 (43%) had a revision hip arthroscopy for recurrent cam/pincer.
Return-to-Sport Outcomes in Basketball Players After Hip Arthroscopy (n = 43) a

After exclusion of those who did not return owing to graduation, changing priorities, or other nonmedical reasons.
Percentage is based on those who returned to basketball.
Subanalysis of all 53 patients, comparing those who returned to sport versus those who did not, indicated significantly improved scores on the mHHS (90.0 vs 79.3), HOS-ADL (93.7 vs 84.1), HOS-Sport (88.0 vs 68.3), Tegner Activity Scale (6.3 vs 4.5), VAS with use (2.2 vs 3.4), and surgery satisfaction scale (8.5 vs 6.9; P < .05 for all) (Table 3).
Comparison of Postoperative PROMs: RTS vs No RTS in Basketball Players a

Bold indicates P < .05. PROM, patient-reported outcome measure; RTS, return to sport; VAS, visual analog scale.
Predictors of RTS
A logistic regression model was performed to analyze predictors of RTS. Analysis compared BMI (≥25 vs <25 kg/m2), sex (male vs female), age (>30 vs ≤30 years), level of play (high school vs recreational, college vs high school), alpha angle (>60° vs ≤60°), LCEA (>40° vs <40°), Tonnis grade (0 vs 1 vs 2), Tonnis angle, and basketball position (forwards vs guards vs centers) with the binary outcome of return to basketball (Table 4). However, no significant associations were found, and the odds of returning to basketball were similar (P > .05), except between high school and recreational athletes in which high school athletes had lower odds of return. Yet, no significant associations were found among only those who tried to RTS, and the odds of returning to basketball were similar between high school and recreational athletes (P = .051).
Logistic Regression Results for Predictors of Return to Basketball After Hip Arthroscopy: All Players a
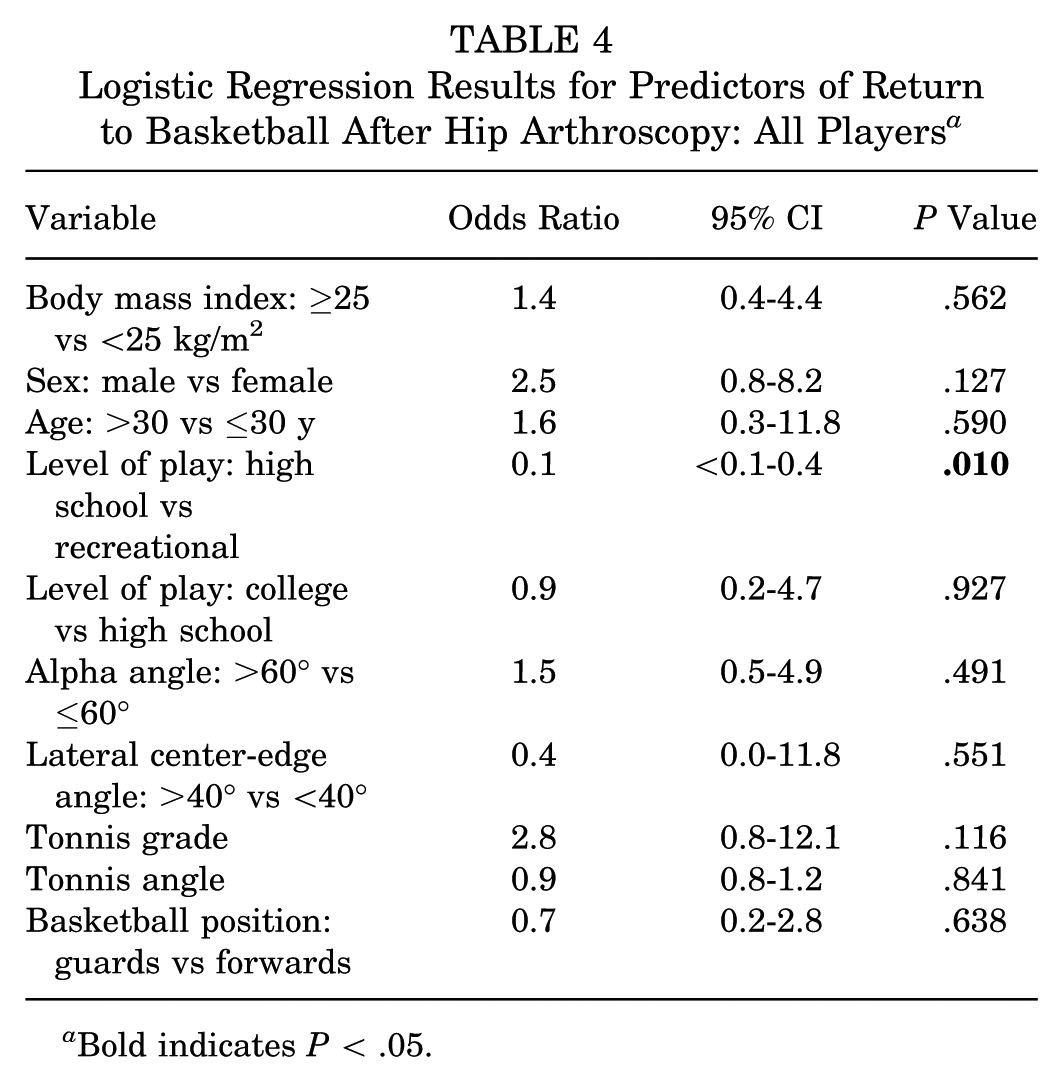
Bold indicates P < .05.
Clinical Outcomes
PROMs were collected for 46 patients (87%) at minimum 5-year follow-up. The mean follow-up postoperatively was 9.1 ± 2.4 years. The mean mHHS was 86.1 ± 13.4 (95% CI, 82.2-89.6), the mean HOS-ADL was 90.2 ± 13.9 (95% CI, 86.1-94.2), and the mean HOS-Sport was 80.9 ± 21.4 (95% CI, 74.6-87.2) (Table 5). The mean postoperative Tegner activity level was 5.7 ± 2.3 (95% CI, 5.0-6.4). Thirty-seven patients (80%) reported their hips feeling slightly better or much better than before surgery. On a 1-10 scale, the mean surgery satisfaction was 7.9 ± 2.6 (95% CI, 7.2-8.6).
Final Follow-up Postoperative PROMs in All Basketball Players a
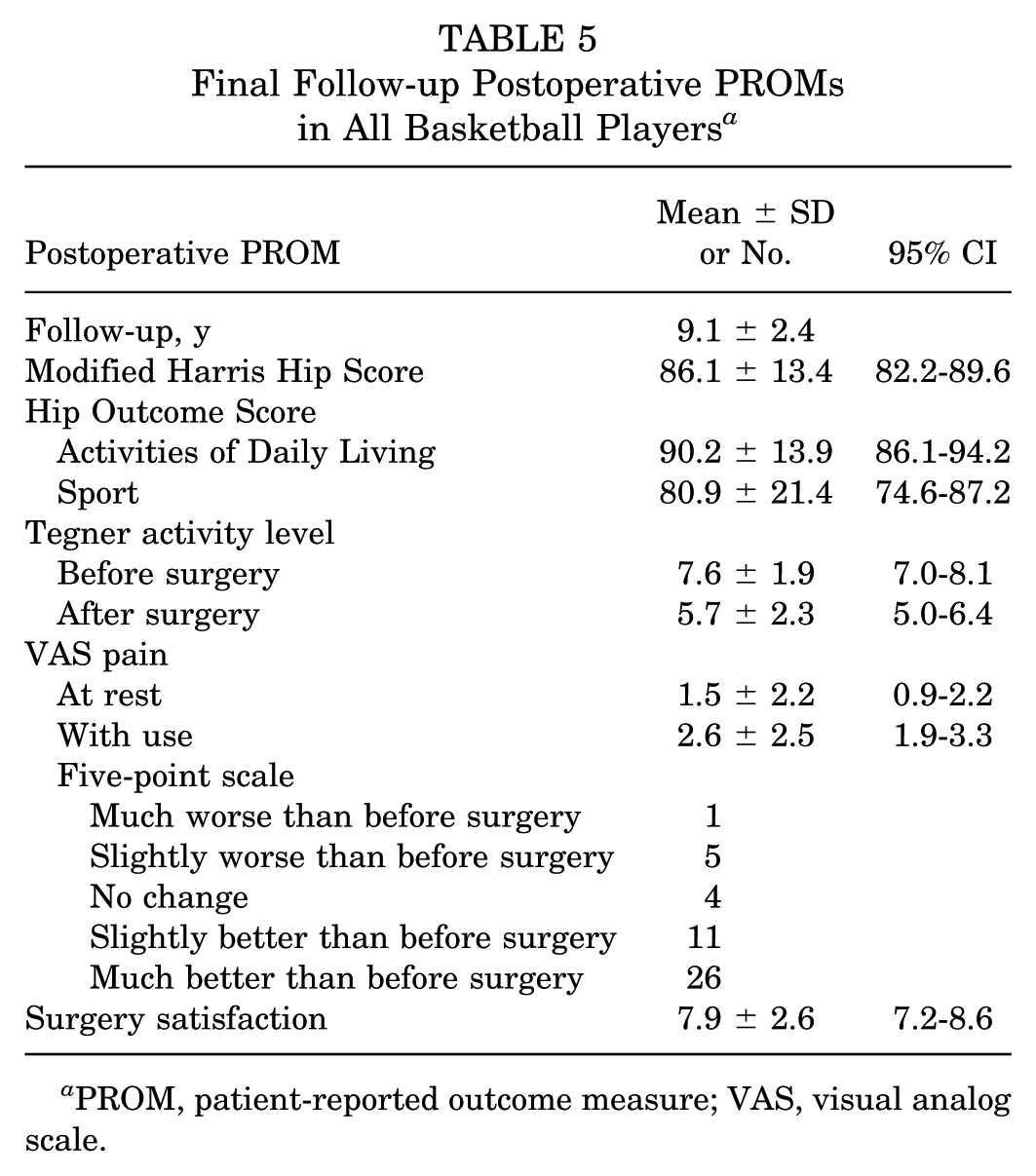
PROM, patient-reported outcome measure; VAS, visual analog scale.
Comparing pre- and postoperative outcome scores revealed significantly increased scores on the mHHS (63.5 vs 86.1), HOS-ADL (70.8 vs 90.2), and HOS-Sport (55.7 vs 80.9) at final follow-up (all P < .001) (Figure 2). VAS pain with use significantly decreased pre- to postoperatively at final follow-up (4.4 vs 2.6; P < .05).

Pre- versus postoperative outcome scores among basketball players. Data are presented as mean ± SD. *P < .05. VAS, visual analog scale.
Complications/Reoperations
Eight patients (15%) had reoperations at a mean 2.0 ± 2.4 years after primary hip arthroscopy (Table 6). Reoperations included 5 patients who underwent revision hip arthroscopy for FAI, 2 who underwent a periacetabular osteotomy, and 1 who had resection of heterotopic ossification.
Reoperations and Revisions a
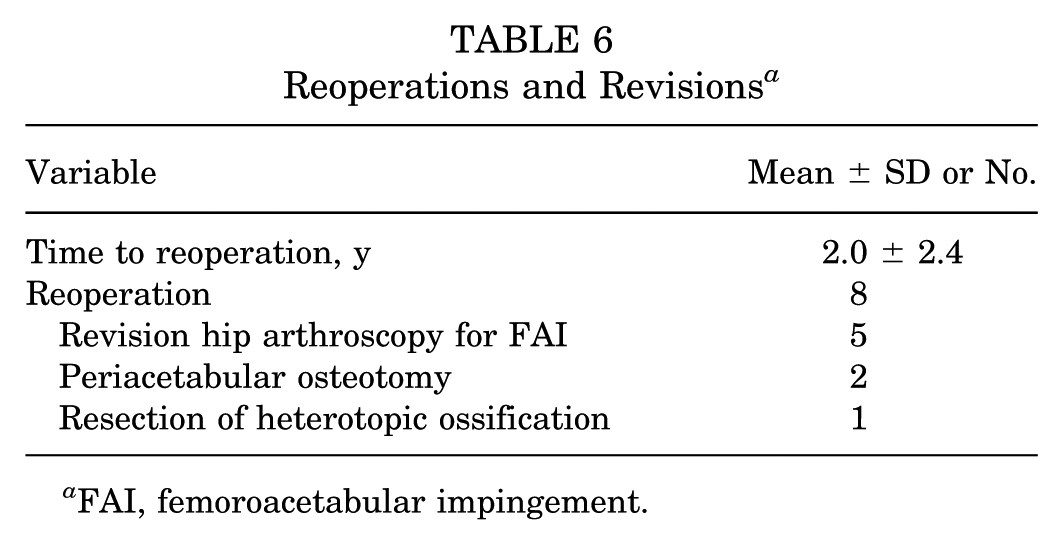
FAI, femoroacetabular impingement.
Discussion
The primary finding in this study is that at a mean follow-up of 9 years, basketball players across various levels of sport had a reasonable RTS rate of 81%, with 91% returning to the same or higher level of play, and that PROMs demonstrated statistically significant improvement (P < .001) when compared with presurgery. Patients who achieved RTS had significantly higher PROMs than those who did not. Furthermore, logistic regression did not reveal that BMI, sex, age, level of play, alpha angle, or position was associated with RTS outcomes in basketball players.
Multiple studies have specifically evaluated professional basketball players and demonstrated very favorable RTS rates of 84.6% to 100%.4,8,9,17 These cohorts represent highly motivated athletes to RTS and are thus less generalizable to the general athletic population. On the contrary, Chen et al 5 evaluated a cohort of primarily recreational basketball players at 2 years and reported a 64.5% RTS rate. Owens et al 15 evaluated basketball players from multiple activity levels and showed an RTS rate of 76.5%. Here, we found that for basketball players who attempted to RTS, their rate of RTS was 81% at a mean 9-year follow-up, with all patients being followed for at least 5 years. This finding is important as it shows continued RTS over a longer term than that of many previous studies, revealing that basketball players have continued clinical benefits at midterm. We noted that of the 7 patients who did not return, almost half (43%) had a revision hip arthroscopy for recurrent impingement pathology. We can hypothesize that this may have accounted for their failure to RTS. For the remaining 4 patients who did not return, it is difficult to discern their specific reasoning given the retrospective nature of our study. In addition, we measured an overall RTS of 66% when we included patients who did not return for nonhip-related reasons (ie, graduation, changed priorities, other nonmedical reasons). It is essential to characterize these separately as, in many cohorts, some patients may not attempt or intend to RTS; thus, the results may be negatively skewed. Ko et al 11 conducted a qualitative review of RTS after hip arthroscopy for FAI. They showed 3 themes in an athlete's ability or inability to achieve RTS: self-efficacy, social support, and resetting expectations. These data support that many factors can influence an athlete's desire or drive to RTS, and when we evaluate RTS rates, reasons beyond their injury/surgery should be considered.
Most patients in our cohort had available PROMs (87%). Patients had significantly increased scores on the mHHS, HOS-ADL, and HOS-Sport and decreased VAS pain with use at final follow-up as compared with presurgery. Furthermore, we show that RTS is associated with improvement in PROMs. Previous literature has shown improved PROMs at short-term follow-up for basketball players.5,15 Domb et al 6 demonstrated that in their cohort of 157 patients, there was an improvement in mHHS, HOS-ADL, HOS-Sports Specific Subscale (SSS), and Non-arthritic Hip Score at 2 years in those who did and did not RTS. The returning athletes had significantly higher HOS-SSS scores correlating with sport-specific movement. Our findings here support the consensus that athletes’ PROMs improve after hip arthroscopy, with additional data showing that this improvement is durable at a mean 9 years postoperatively for basketball players.
Based on preoperative variables, efforts have been made to predict RTS outcomes and favorable PROMs for patients. Sogbein et al 19 conducted a systematic review including 9272 hips to assess for predictors of outcomes after hip arthroscopy for FAI. They showed that patients with younger age, male sex, lower BMI, Tonnis grade 0, and pain relief from preoperative intra-articular hip injection were more likely to achieve positive postoperative outcomes. The logistic regression analysis performed in our cohort of basketball players demonstrated that preoperative predictors of BMI, sex, age, alpha angle, LCEA, Tonnis grade, Tonnis angle, or position could not predict RTS. Only the comparison between high school and recreational level of play demonstrated that high school athletes had lower odds of returning to play. This could likely be due to multiple factors, injury and noninjury related, such as graduation. There was no significant difference in odds between high school and recreational athletes when we excluded those who did not intend or try to RTS (eg, because of graduation), further supporting the idea that this difference in odds could be due to nonhip factors. Our findings here are limited by the relatively smaller sample size and overall high RTS rate, leading to a decreased power to detect any significant difference. Still, previous literature can help guide shared decision-making regarding which patients may benefit from hip arthroscopy, and surgeons should continue to apply this logic to athletic populations.
Hip arthroscopy for athletes has been considered a safe procedure with minimal complication rates. In our cohort, 8 patients (15%) went on to reoperation at a mean 2 years after their primary surgery. No patients went on to total hip arthroplasty during the study period. There were 5 revision arthroscopic procedures and no other reported complications. Jimenez et al 10 studied athletes who returned to the sport and those who did not and noted that 11% of patients went on to revision arthroscopy. Still, there was no significant difference between the RTS and non-RTS rates of revisions. In a basketball-only cohort by Chen et al, 5 3 patients (9.7%) went on to total hip arthroplasty at a mean 35.9 months; however, these were patients >40 years old. The rate of secondary arthroscopy was 12.9% during the 2-year follow-up study. Here, we demonstrate a slightly higher rate of reoperation at midterm. Still, all patients maintained native joint preservation at a mean 9 years postoperation, and there were no other surgical complications.
The primary limitation of this study is that it is a retrospective review of patients. There is a risk of recall bias, given that patients had to complete surveys for their responses at the final follow-up. Also, there may be an element of selection bias in those who were not lost to follow-up having more favorable results. Furthermore, it is important to note that PROMs and RTS may not capture the full spectrum of clinically relevant improvement for athletes; although these are important, further studies may be able to understand more objective metrics of recovery for our athletic populations. Additionally, advancements in hip arthroscopy during this study's period may have resulted in differential management of FAI, or any surgeon-to-surgeon differences could have influenced patient outcomes. Last, the generalizability of these data could be compromised given that all the data were collected at a single large tertiary care center and our cohort does not include professional athletes.
Conclusion
At a minimum 5 years of follow-up, basketball players demonstrated durable improvements in PROMs and an RTS rate of 81% after hip arthroscopy for FAI. The majority of athletes returned to the same level of competition. There were significantly improved PROMs in patients who returned to sport versus those who did not. High school athletes had decreased odds of RTS when compared with recreational athletes; however, BMI, sex, age, alpha angle, and basketball position did not significantly correlate with RTS outcomes.
Footnotes
Final revision submitted September 4, 2025; accepted October 6, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.A.L. receives royalties from Arthrex, Inc; is a paid consultant for Arthrex, Inc; has received nonconsulting fees from Arthrex, Inc; has received travel and lodging from Arthrex, Inc; holds stock or stock options in COVR Medical LLC; and is an editorial or governing board member of the Journal of Knee Surgery, Knee Surgery, Sports Traumatology, Arthroscopy, and Orthopedics Today. M.H. is a paid consultant for DJO-Enovis, Moximed, and Vericel; receives publishing royalties or financial or material support from Elsevier; has received support for education from Smith & Nephew, Inc, Medwest Associates, Foundation Medical, LLC, and Arthrex, Inc; has received honoraria from Encore Medical, LP; has received a grant from Medical Business Services, Inc; and is an editorial or governing board member of the Journal of Cartilage and Joint Preservation. A.J.K. receives royalties from Arthrex, Inc; is a paid consultant for Arthrex, Inc; has received nonconsulting fees from Arthrex, Inc; has received travel and lodging from Arthrex, Inc; has received a grant from Arthrex, Inc; is an editorial or governing board member of The American Journal of Sports Medicine and Springer; and is a board or committee member of the Arthroscopy Association of North America and International Cartilage Repair Society. K.R.O. is a paid consultant for Arthrex, Inc, and Smith & Nephew, Inc; has received nonconsulting fees from Smith & Nephew, Inc, and Synthes GmbH; and has received travel and lodging from Smith & Nephew, Inc, and Synthes GmbH. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.