
Abstract
Background:
Opioids are a fixture of postoperative pain management for hip arthroscopy. However, prescriptions can be wide-ranging and there is a paucity of literature regarding patient utilization of prescriptions.
Purpose:
To (1) quantify patient opioid consumption and disposal methods after primary hip arthroscopy; (2) establish demographic, radiographic, and intraoperative predictors of increased postoperative opioid use; and 3) evaluate preoperative and postoperative NSAID usage.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A prospective cohort study was conducted of patients who underwent hip arthroscopy at a single institution. Patient inclusion criteria included patients aged ≥18 years who were clinically indicated for hip arthroscopy for a symptomatic labral tear secondary to femoroacetabular impingement and returned a completed postoperative pain and medication use log at suture removal. Exclusion criteria included previous surgery on the ipsilateral hip and previous opioid use.
Results:
A total of 77 patients met the inclusion criteria. Postoperatively, patients consumed a mean ± SD 8.3 ± 9.63 of 5-mg oral oxycodone and 37.3 ± 26.8 of 200-mg oral NSAID tablets. Of patients, 23% did not consume any opioid medications postoperatively. The mean number of leftover tablets was 27.4 ± 16.4. The majority of patients did not follow proper disposal guidelines (83.3%). Increased body mass index, Tönnis grade, and alpha angle were significant predictors of increased consumption of opioids (all P < .05). There was a significant positive relationship between the number of opioids and the number of NSAIDs taken postoperatively (P = .017).
Conclusion:
Overall, patients consumed fewer opioids than prescribed and did not correctly dispose of opioid medications, underscoring the need for prescription guidelines and disposal education. NSAID use was also prominent in the patient population, demonstrating that opioids and NSAIDs together can be effective pain management strategy tools for hip arthroscopy patients in the postoperative period.
Overprescription of opioids after orthopaedic surgery has been identified as a major contributing factor to the opioid epidemic in the United States. 33 Several studies have identified that surgical patients receive larger prescriptions for opioids than necessary for postoperative pain relief,4,26,33 leading to prolonged use, potential abuse, and an increased supply of opioids that could be diverted for nonmedical use. Orthopaedic surgeons are routinely among the highest prescribers of opioids across all medical specialties.19,25 Opioid prescribing has been found to vary widely among surgeons, suggesting that individual prescribing habits may drive this inconsistency and contribute to overprescription, illustrating the need for evidence-based guidelines. 36 As orthopaedic patients can have chronic pain before surgery, their anticipated need for pain medications may be higher preoperatively.
Inappropriate use can be further augmented by a lack of education surrounding proper disposal methods for leftover medication,15,17 as surgical patients without educational intervention report improper disposal. Prolonged personal use or the obtainment of opioids meant for someone else can be a consequence of mismatched prescriptions that contribute to abuse. 26 It has been posited that lower-risk drugs for pain management, such as nonsteroidal anti-inflammatory drugs (NSAIDs) can be used to reduce opioid consumption, and possible misuse, for perioperative pain management.6,24
For hip arthroscopy patients, opioids are a fixture of postoperative pain management. However, prescriptions can be wide ranging and there is a paucity of literature regarding patient utilization of prescriptions. 27 Although previous studies have investigated opioid consumption following hip arthroscopy through methods such as pill counting or prescription refill requests at 2- and 6-week postoperative appointments,5,9 few have examined what happens when patients do not take opioids at all, or whether they can rely on nonopioid alternatives like NSAIDs. Additionally, there remains a significant gap in understanding how patients handle leftover opioids, including whether and how they dispose of unused medication. These underexplored areas are critical for developing more responsible patient-centered pain management strategies. There is a growing need to assess opioid use in the perioperative period with greater granularity, capturing the actual number of pills patients consume rather than relying on prescription data or broad time point estimates. Therefore, it is valuable to understand the size of prescriptions that are warranted after hip arthroscopy. To prevent potential community harm, investigation into methods of disposal for narcotics after hip arthroscopy is warranted. 26
The paucity of evidence-based guidelines indicates that further research is needed to assess the size of opioid prescriptions. The purpose of this study is to prospectively (1) quantify patient opioid consumption and disposal methods of narcotics after primary hip arthroscopy; (2) establish demographic, radiographic, and intraoperative predictors of increased postoperative opioid use; and (3) evaluate postoperative NSAID usage.
Methods
Study Design
This study was approved by our institutional review board. This was a prospective study of patients undergoing primary hip arthroscopy by the senior surgeon (S.D.M.) between September 2018 and April 2023. Patients included in this study met the following eligibility criteria: ≥18 years old, completed pain logs regarding medication use, and underwent primary hip arthroscopy for acetabular labral repair secondary to femoroacetabular impingement. Exclusion criteria for this study consisted of patients <18 years old; previous opioid use; previous ipsilateral or contralateral hip surgeries; previous ipsilateral hip conditions such as avascular necrosis, seronegative spondyloarthropathies affecting the hip, or fracture; and incomplete pain logs. All patients included in this study were opioid naïve, meaning they had not used opioids for >7 consecutive days in the past 30 days.
Patients upon initial clinic visit were assessed for indications of acetabular labral tears. This included preoperative evaluation with hip/pelvic radiographs (anteroposterior pelvic, anteroposterior lateral of affected hip, and Dunn lateral views) and physical examinations in which flexion, adduction, and internal rotation as well as flexion, abduction, and external rotation were evaluated for motion limitations or pain. Patients also received a diagnostic and therapeutic intra-articular corticosteroid injection, ≥3 months of physical therapy, and magnetic resonance arthrography. Patients who had persistent pain despite these nonoperative interventions were clinically indicated for hip arthroscopy.
Before surgery, enrolled patients were instructed to use over-the-counter NSAIDs for mild breakthrough pain as needed. After surgery, each patient was prescribed 20 to 60 tablets of 5-mg oxycodone and instructed to take 1 tablet for breakthrough pain of moderate intensity every 4 to 6 hours as needed. As prescription guidelines were not standardized throughout the study period, prescription sizes were based on anticipated need by the senior surgeon. These amounts decreased over the course of the study period as the adverse effects of opioid usage became increasingly recognized. During the surgery, general anesthesia was used without nerve blocks. Additionally, following surgery, patients were instructed to take over-the-counter NSAIDs as needed for mild levels of pain. There were no standardized prescriptions for NSAIDs after surgery.
Patients were provided with a medication and visual analog scale (VAS) pain log to record their daily medication use (opioid and NSAID) and pain levels preoperatively and on postoperative days 1, 5, 10, and at suture removal (between postoperative day 12 and 14 in all patients). The principal investigator (S.D.M.) or a trained research associate explained to the patient how to correctly record information including pain levels using the VAS and medication use each day. Upon suture removal, patients were also queried for their opioid disposal method and provided their completed pain logs to the clinic staff.
All statistical analyses and calculations were performed using R studio (Version 2022.07.02+576). Poisson regressions were used to analyze the directional relationships between pain management and demographic, intraoperative, and radiographic factors. Opioid consumption by the number of 5-mg oxycodone was converted to oral morphine equivalent (OME) for accurate data analysis. 20
Results
A total of 86 patients were eligible for this study, with 77 patients included (6 excluded for incomplete pain logs and 3 for possible previous opioid use) (Figure 1 and Table 1).

CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Baseline Characteristics, Preoperative Imaging, and Intraoperative Findings (N = 77) a

Data are presented as mean (95% CI) or n (%). BMI, body mass index; FAI, femoroacetabular impingement.
Patients were prescribed a mean 35.7 ± 16.3 of 5-mg oral oxycodone pills and took 8.3 ± 9.63 (12.5 ± 14.4 OME) pills (Table 2). Of total patients, 90% consumed <21 pills postoperatively (31.5 OME) and 23% of patients took no pills at all postoperatively. The mean number of days patients took opioids after surgery was 3.61 ± 3.68, and 90% of patients took opioids for <9 days. When patients ceased opioid use, of those who had leftover pills, the majority disposed of opioids incorrectly (83.3%), and the mean number of leftover tablets was 27.4 ± 16.4 (41.1 ± 24.6 OMEs) (Table 3). Over the 2-week period, pain scores as well as opioid and NSAID consumption all decreased, with a mean VAS pain score of 4.9 on day 1 postoperatively and a mean VAS pain score of 2.01 at suture removal (Figure 2). Pain the day after surgery and prescription size had a significant positive relationship with the number of postoperative opioid pills consumed (P < .001).
Mean Amount and Range Taken by Prescription Size

Opioid Disposal Methods (for N = 77 patients)

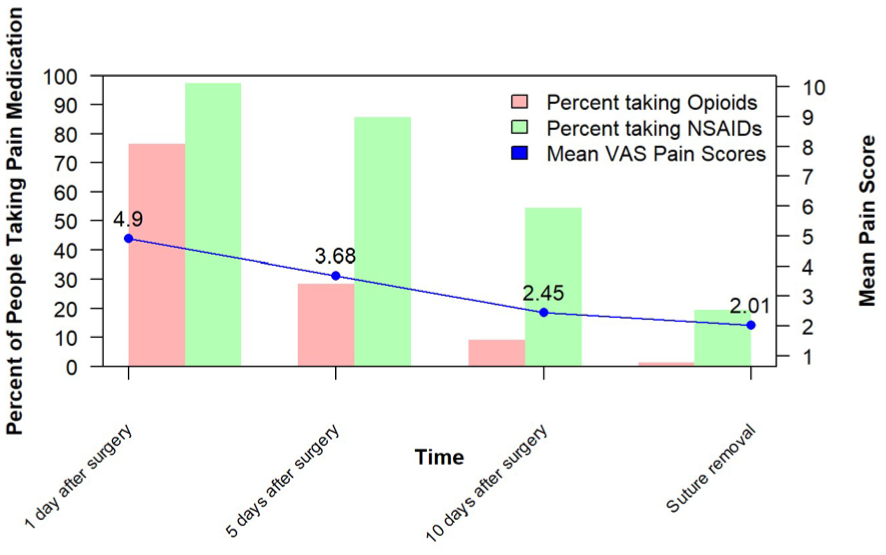
Pain and medication postoperatively. NSAID, nonsteroidal anti-inflammatory drug. VAS, visual analog scale.
On a Poisson regression, the number of opioids taken increased with body mass index (BMI) (P < .001) and decreased with age, although this was not significant (P = .11). In regard to intraoperative and radiographic factors, the number of opioids taken increased with Tönnis grade (P = .002) and alpha angle (P < .001) (Table 4).
Demographic, Intraoperative, and Radiographic Factors by Poisson Regression

Preoperatively, 23 of the 77 patients (29.8%) reported using NSAIDs before surgery, with a mean of 5.5 ± 2.4 per day. The mean number of opioid pills used postoperatively was 9.0 in patients who took NSAIDs preoperatively and 7.2 in those who did not. This difference was not statistically significant (P = .51). Logistic regression showed that preoperative NSAID use was also not a significant predictor of whether a patient used any opioids postoperatively (odds ratio, 1.14; P = .83).
Postoperatively, there was a significant positive relationship between the number of opioids and the number of NSAIDs taken (P = .017). The mean number of NSAIDs taken was 37.3 ± 26.8 pills. The mean number of days patients took NSAIDs after hip arthroscopy was 9.45 ± 4.12 and the maximal number of days reported was 14 (at data collection conclusion). The number of NSAIDs taken increased with increased pain the day after surgery (P < .001).
Discussion
The primary finding of this study is that patients consumed on average 8.3 ± 9.63 5-mg oxycodone pills. Furthermore, 23% of patients managed pain postoperatively without taking any opioids, and 90% of patients took <21 opioid pills after hip arthroscopy. The findings in this study are consistent with previous orthopaedic studies that quantify opioid consumption after primary arthroscopic procedures. Cunningham et al 9 reported that opioid-naive patients often took less than thirty 5-mg oral oxycodone pills after hip arthroscopy at 2 weeks after surgery, with the potential of up to fifty 5-mg oxycodone pills leftover. This potential for overprescription extends to other common arthroscopic procedures, as Sheth et al 27 described in a systematic review, 31%, 34%, and 64% of opioid pills prescribed were left over after shoulder, knee, and hip arthroscopy, respectively. Although there are no standardized guidelines for prescription sizes after hip arthroscopy, twenty 5-mg oxycodone pills are often the maximum recommended to reduce overprescription for other orthopaedic procedures, such as arthroscopic shoulder or ACL repair. 21 Increased prescription sizes, in this study as well as in the literature, have been shown to lead to increased consumption of opioids, likely because patients use prescription size as a tool to gauge their pain management needs. 36
The next key finding is that 83.3% of patients who had leftover opioid pills didn't comply with current disposal guidelines for opioids. Leftover prescription opioid pills that are not correctly disposed are known contributors to the opioid epidemic, either from diversion or misuse.1,22 Current FDA guidelines for the handling of oxycodone when treatment has concluded are to participate in a take-back program, in which opioids are returned to the pharmacy or other drop-off location, or to flush the medication down the sink or toilet. 13 A systematic review of surgical randomized controlled trials related to patient education about opioid disposal has shown that proper disposal of opioids significantly increases when educational material is provided to patients upon surgical discharge, with disposal rates of up to 71%. 12 Furthermore, patient education about opioid disposal can lead to increased awareness that leftovers have the potential to harm others and can reduce instances of purposefully saving for future use. Another study by Stokes et al 30 found that provision of at-home disposal kits in which leftover opioids were neutralized and then deposited in the trash led to significant increases in proper opioid disposal. As only 14.1% of patients in the present study engaged in proper disposal (take-back or flushing), implementation of opioid disposal method education programs in postoperative guidelines and provision of neutralization options/proper disposal tool kits for hip arthroscopy may help to prevent misuse or improper disposal of leftover pills.
This study also took predictive factors of increased opioid use into consideration, including demographics and radiographic variables. As BMI has been previously shown to be a significant predictor of poor postoperative pain management, 35 it is reasonable that this would also be a significant predictor of increased opioid use after hip arthroscopy. Higher BMI may be associated with increased postoperative pain for several reasons, including higher stresses on joints and increased inflammation, higher likelihood of previous chronic pain conditions, and lower pain tolerance.16,23,29,31 Higher Tönnis grade and alpha angles were also associated with increased opioid use after surgery. Previous studies have shown that patients with greater Tönnis grade and alpha angle have significantly greater odds of severe acetabular rim chondral damage and pain. Therefore, patients with greater Tönnis grade and alpha angle may require a higher level of personalized postoperative pain management. 35 These findings could be taken into consideration if prescription size were to be individualized. Shared decision making between patient and provider regarding care has been recommended to account for individualized circumstance and reduce prescription sizes.2,28
The final key finding of this study was that greater proportions of the study cohort utilized NSAIDs for pain management in combination with or instead of opioids. As it has been shown that decreasing opioid prescription sizes does not affect patient satisfaction with postoperative care, 18 encouraging NSAID usage has the potential to be beneficial to hip arthroscopy patients while mitigating the risks of large opioid prescriptions. This is illustrated in the current study, as 23% of patients were able to engage in postoperative pain management without the use of opioids entirely. NSAIDS also have been previously illustrated to have the added potential of decreasing the risk of heterotopic ossification in hip arthroscopy patients. 3 Although there are potential risk factors associated with prolonged NSAID use, such as gastrointestinal, cardiovascular, or renal issues, appropriate use in the short postoperative period has not been shown to increase the risk of any organ dysfunction. 8 NSAIDs in combination with acetaminophen (paracetamol) have also been shown to be effective in managing pain in orthopaedic patients as well as in the postoperative period.7,10,32 Finally, Gormley et al 14 found in a systematic review of randomized trials that NSAIDs taken with opioids can reduce opioid consumption after common orthopaedic procedures. Thus, when taken in conjunction with opioids, NSAIDS may be a meaningful tool to lower risk for pain management after hip arthroscopy.
Furthermore, our analysis examined whether preoperative NSAID use influenced postoperative opioid consumption, given that NSAIDs are commonly used for pain management before hip arthroscopy. Nearly 30% of patients reported using NSAIDs before surgery; however, we found no significant difference in postoperative opioid use between patients who did and did not use NSAIDs preoperatively. Logistic regression further supported that preoperative NSAID use was not a significant predictor of postoperative opioid requirements. This finding aligns with a recent systematic review, 11 which found that preemptive or preventive administration of NSAIDs before surgery resulted in no clinically meaningful differences and had no effect on opioid-related adverse events in orthopaedic and other surgical settings. Our findings also suggest that presurgical NSAID analgesia may not affect postoperative opioid needs in this patient population.
Limitations
This study should be interpreted in the context of several limitations. As prescription sizes were not standardized, it is possible that some patients took more opioids or took them over a longer period simply by having higher access to them, rather than based off their analgesic needs. However, this discrepancy was addressed by analyzing the between-group differences when sorted by prescription size, with the finding that one patient who was prescribed 50 pills reported taking all 50, an outlier that significantly brought up the mean of that group. Furthermore, the findings in this study may only be generalizable to the opioid-naive population, as presurgical opioid use has been shown to be a predictor of increased opioid use after surgery. 34 Finally, given the relatively small sample size and variability in preoperative NSAID dosing, future studies with larger cohorts and standardized analgesic protocols are warranted to fully elucidate any potential effects. Further studies can also be done to address the effect of opioid disposal education on hip arthroscopy patients and the effectiveness of combination NSAID and acetaminophen for pain control in this population.
Conclusion
Overall, patients consumed fewer opioids than prescribed and did not correctly dispose of opioid medications, underscoring the need for prescription guidelines and disposal education. NSAID use was also prominent in the patient population, demonstrating that opioids and NSAIDs together can be effective pain management strategy tools for hip arthroscopy patients in the postoperative period.
Footnotes
Acknowledgements
The authors thank the Coinine Family Fund for Joint Preservation for their continued research support and Mark Cote, PT, DPT, MSCTR, for statistical assistance.
Final revision submitted August 22, 2025; accepted September 30, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional review board of Massachusetts General Hospital.