
Abstract
Background:
The success of anterior cruciate ligament (ACL) reconstruction is influenced by precise anatomic knowledge, which may vary across populations. Despite extensive research on ACL anatomy, direct comparisons between Asian and Western populations remain unexplored.
Purpose/Hypothesis:
The purpose of this study is to systematically compare the footprint size and location of ACL and its individual bundles in Asian and Western populations. It was hypothesized that the ACL footprint size and location of the Asian population would differ from those in the Western population.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review and single-arm meta-analysis were conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Studies on ACL footprint anatomy were included and stratified into subgroups based on the origin of the data (Asian or Western regions). Meta-analyses were performed for femoral and tibial footprint locations of the entire ACL and its anteromedial and posterolateral bundles. The ACL femoral and tibial footprint areas were also compared. Statistical heterogeneity was assessed using a random-effects model.
Results:
A total of 50 studies with 1652 knees were included in the meta-analysis, with 25 studies per subgroup.The center of the ACL femoral footprint was located at 35.2% and 27.3% from the posterior edge of the lateral femoral condyle in the Asian and Western subgroups, respectively (P < .001), and 39.4% and 33% from the Blumensaat line, respectively (P = .049). The Asian subgroup exhibited smaller femoral footprint areas (96.3 mm2 [95% CI, 81.1-111.4] vs 126.8 mm2 [95% CI, 103.5-150]; P = .03). No significant difference was found in the tibial footprint location or size.
Conclusion:
This meta-analysis demonstrated that the ACL femoral footprint in the Asian population is located more anteriorly and distally than in the Western population, and the femoral footprint size is smaller. These findings provide valuable insights for population-specific surgical strategies in the future.
Keywords
Significant interest continues to be shown in exploring theanatomy of the anterior cruciate ligament (ACL) in the 21st century because of its complex structure.4,12,25,47,50,58,78,82 According to Morales-Avalos etal, 55 >2700 articles on ACL anatomy and approximately 14900 articles covering ACL-related topics have been published in the past decade. It is suggested that precise anatomic ACL reconstructions (ACLR) could achieve significantly better joint stability and knee joint functionality.8,17,34,70
Previous studies have highlighted differences in knee ligamentous anatomy between Asian and Western populations.21,42 A recent systematic review of the knee anterolateral ligament 21 revealed its presence in 82% of North Americans, 65% of Europeans, and only 46% of Asians. Previous systematic reviews on ACL anatomy have reported high variability among included anatomic studies. However, no study has yet compared ACL anatomy among different ethnic groups.
Furthermore, the emergence of novel anatomic measurement techniques, such as 3-dimensional (3D) magnetic resonance imaging (MRI) reconstruction74,81,82 and 3D histological reconstruction,32,69 has led to new findings and data—including the precise footprint locations of the anteromedial band and posterolateral bundles of the ACL or the extensive femoral insertion of the ACL's fan-like fibers.
The present study aimed to systematically compare the ACL footprint size and location between Asian and Western populations using a meta-analysis that strictly includes comparable, quantitative, and updated anatomic data. This study aimed to provide a practical understanding of the differences in ACL footprint and inform population-specific surgical strategies.
Methods
Data Sources and Search Strategy
This study was conducted by following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guideline. A search of the Web of Science and PubMed databases was performed in July 2024. Search strategy for Pubmed database was ((("Anterior Cruciate Ligament"[Mesh] OR "ACL" OR "cruciate ligament") AND ("Anatomy"[Mesh] OR "morphometry" OR "morphology" OR "size" OR "dimensions" OR "structure" OR "footprint" OR "location")) NOT ("Child"[Mesh] or "Children" or "pediatric" or "paediatric")).
The search strategy for Web of Science database was TS= (("Anterior Cruciate Ligament" OR "ACL" OR "cruciate ligament") AND ("anatomy" OR "morphometry" OR "morphology" OR "size" OR "dimensions" OR "structure" OR "footprint" OR "location")) NOT TS = ("child*" OR "children" OR "pediatric*" OR "paediatric*") AND PY = (1994-2024).
Inclusion and Exclusion Criteria
The criteria for inclusion were met if studies (1) were published from Asia, North America, or Europe; (2) studies published in English or abstract in English, which included all necessary data; (3) studies on human adults; and (4) studies that measured the anatomy of ACL femoral or tibial footprints through cadaveric dissection, radiological images, histologic analysis, or arthroscopic measurements.
To conduct a meta-analysis between Asian and Western groups, studies were excluded based on the following criteria: (1) studies containing only descriptive anatomic results without precise data measurement of the ACL femoral or tibial footprint; (2) case reports, editorials, reviews, letters, and other nonoriginal research papers; (3) studies where cadaveric specimens or patients were not consistent with their publication region; (4) studies measuring intraoperative femoral or tibial tunnel sizes or locations instead of natural ACL footprints; (5) For femoral and tibial footprint location studies, those not using the standard quadrant method were excluded; (6) Studies that did not report the footprint size area in either mm2 or cm2 were excluded; and (7) For studies published by the same author using the identical cadaveric specimens, only 1 study was included to avoid duplication.
The inclusion and exclusion flowchart following the PRISMA guidelines is shown in Figure 1.
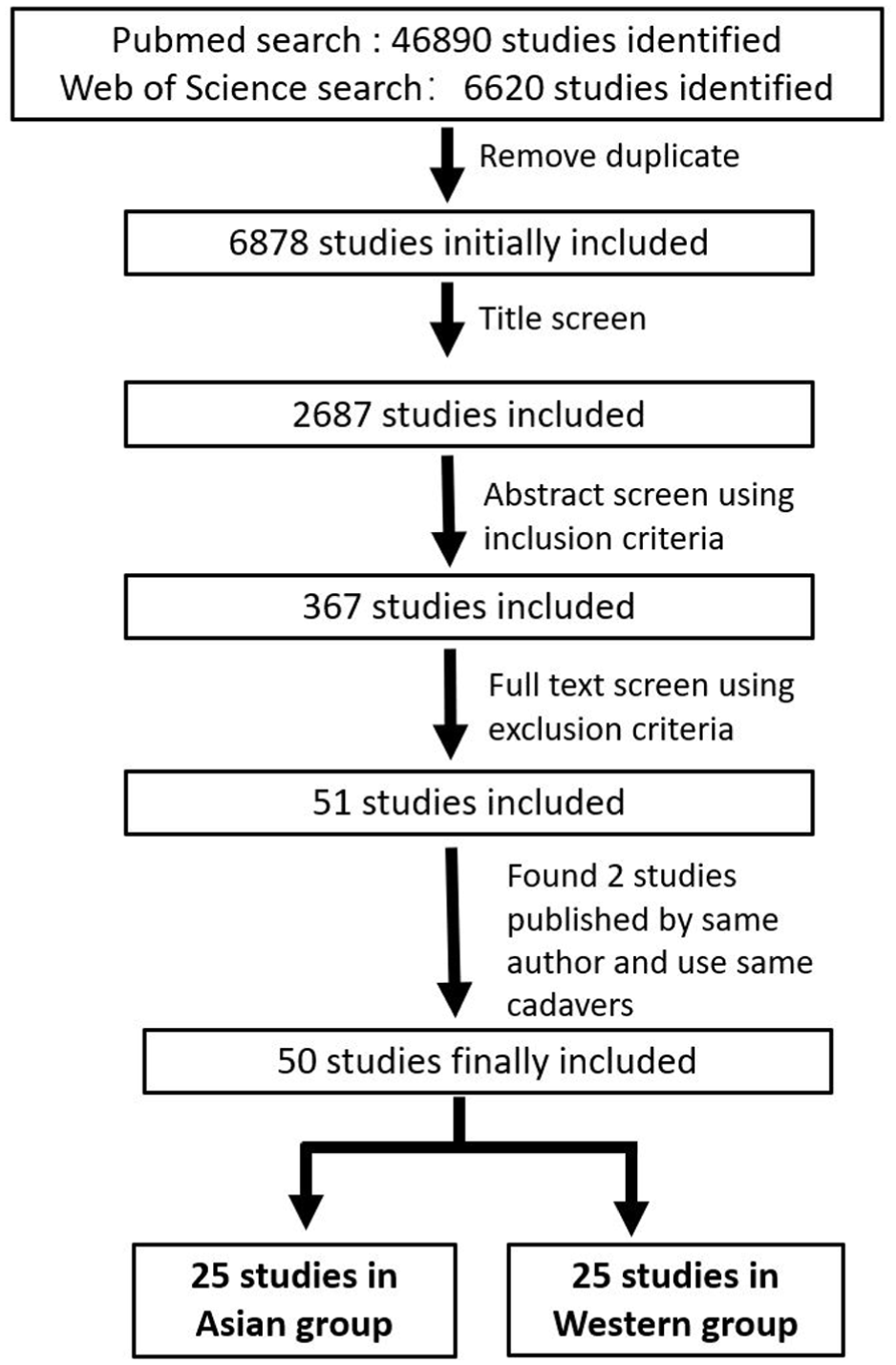
Flowchart of study screening based on the inclusion and exclusion criteria.
Data Extraction and Outcomes
Data extraction focused on (1) basic information—including author, publication year, and region; (2) study materials—including sex, mean age of cadaveric specimens, or adult patients; (3) methods for measuring ACL footprint—including cadaveric dissection, radiograph-based measurement, MRI reconstruction, computed tomography (CT) reconstruction, or histologic reconstruction; and (4) anatomic measurement data—including femoral footprint location, tibial footprint location, and footprint size (in mm2 or cm2).
Femoral Footprint Location
The femoral footprint of the native ACL was measured using various methods. To reduce heterogeneity among the included studies and minimize statistical bias, only studies that used the quadrant method were included. Such a method was first described by Bernard etal 2 in 1997 and has been the most frequently used method.
The quadrant measurement was conducted on a true lateral radiography of the knee with superimposed medial and lateral condyles or on a standard photograph of the medial side of the lateral condyle (Figure 2). A grid was drawn to fit the distal lateral femoral condyle, with its upper border aligned to the Blumensaat line, and other borders tangential to the cartilage surface of the lateral femoral condyle on the anterior, bottom, and medial sides. The locations of the ACL center or the anteromedial (AMB)/posterolateral (PLB) bundle were expressed as a percentage within the grid (Figure 2A).

(A) Quadrant measurement method on the lateral femoral condyle. The red dot represents the mean location of the ACL footprint center in the Asian group, and the blue dot represents the mean location in the Western group.ACL, anterior cruciate ligament.
Tibial Footprint Location
The quadrant method for tibial footprint location was conducted using an axial view of the tibial plateau photograph or a 3D CT reconstruction image. A grid was aligned with the tibial plateau, with borders tangential to the anterior, medial, and posterior edges of the medial tibial plateau and the lateral border of the lateral tibial plateau. The location of the ACL center or the AMB/PLB bundle was expressed as a percentage within the grid (Figure 2B).
Subgroup Allocation
Final included studies were allocated to the Asian group if both the publication region and the cadaveric specimens/patients originated in Asia. Studies were assigned to the Western group if both the publication region and cadaveric specimens/patients originated from Europe or North America.
Risk of Bias and Quality Assessment
To evaluate bias and quality in this single-arm meta-analysis, we adopted a risk-of-bias assessment approach based on a method specifically designed for single-arm studies. 22 Article quality was assessed using the Newcastle-Ottawa Scale, with a focus on the reliability of outcome measurements. 61 A detailed summary of the bias evaluation and quality grading of the included studies is provided in the supplementary 5.
Statistical Analysis
Baseline characteristics comparisons between subgroups were performed in SPSS Statistics, Version 23.0 (IBM). The mean age was compared using a 1-sample t test. Noncontinuous data—including sex distribution and the number of knees investigated by radiographic method—were compared using the chi-squared test.
A single-arm meta-analysis was performed using RStudio Version 2024.09.01 (Posit PBC) for all extracted continuous data—including femoral or tibial footprint locations and areas.
To conduct the single-arm meta-analysis, the meta package was first installed in RStudio. The metamean function was then executed using mean values, sample sizes, and standard deviations. A random-effect model was applied to account for variations between studies. Weighted means were calculated using the inverse variance method, and the heterogeneity parameter was estimated using restricted maximum likelihood.
After the analysis, the overall effect size results provided the mean estimate and 95% CI. Subgroup analyses presented the mean estimates and heterogeneity metrics for each group, with subgroup differences assessed using the Q-test.
The threshold for statistical significance was set at P < .05. When standard deviation data were not provided in the original article, they were calculated based on similar studies.
Heterogeneity within subgroups and between the 2 subgroups was evaluated using the I2 value. Heterogeneity was classified as minimal, moderate, and significant when I2 values were between 0% and 30%, 30% and 60%, or >60%, respectively. 61
Results
A total of 50 studies, involving 1652 knees, were included in this study. Among these, 25 studies were assigned to the Asian group, with 704 knees. § The remaining 25 studies were allocated to the Western group, with 948 knees. ‖ Basic characteristics of the 2 groups are shown in Table 1. A total of 649 knees in the Asian group and 448 knees in the Western group had reported sex distributions, with male-to-female ratios of 1.16 and 1.3, respectively. No significant differences were observed in terms of sex distribution, mean age, or study methods. However, a significant difference was observed in publication years, with a higher percentage of knees in studies published within the past 10 years in the Asian group than in the Western group (65% vs 61%).
Basic Characteristics of Included Studies in Both Subgroups a

Data are provided as the mean ± SD, unless otherwise indicated. The P value indicates a significant difference.
The results of the single meta-analysis are summarized in Table 2.
Summary of Single-Arm Meta-analysis Results a

Data are presented as mean % [95 CI %]. Bold P values indicate statistical significance. ACL, anterior cruciate ligament; AMB, anteromedial; AP, anteroposterior; HL, high-low; ML, mediolateral; PLB, posterolateral; SD, shallow-deep.
The mean location of the ACL footprint center in the Asian group and the Western group was demonstrated in Figure 2.
Footprint Locations
For femoral footprint locations of the whole ACL (Figure 3 with detailed data in supplementary 1) in the shallow-deep direction, the mean femoral footprint center was located at 35.2% and 27.3% from the posterior edge of the lateral condyle in Asian and Western groups, respectively (P < .001). In the high-low direction, the center was located at 39.4% and 33% from the Blumensaat line, respectively (P = .049).
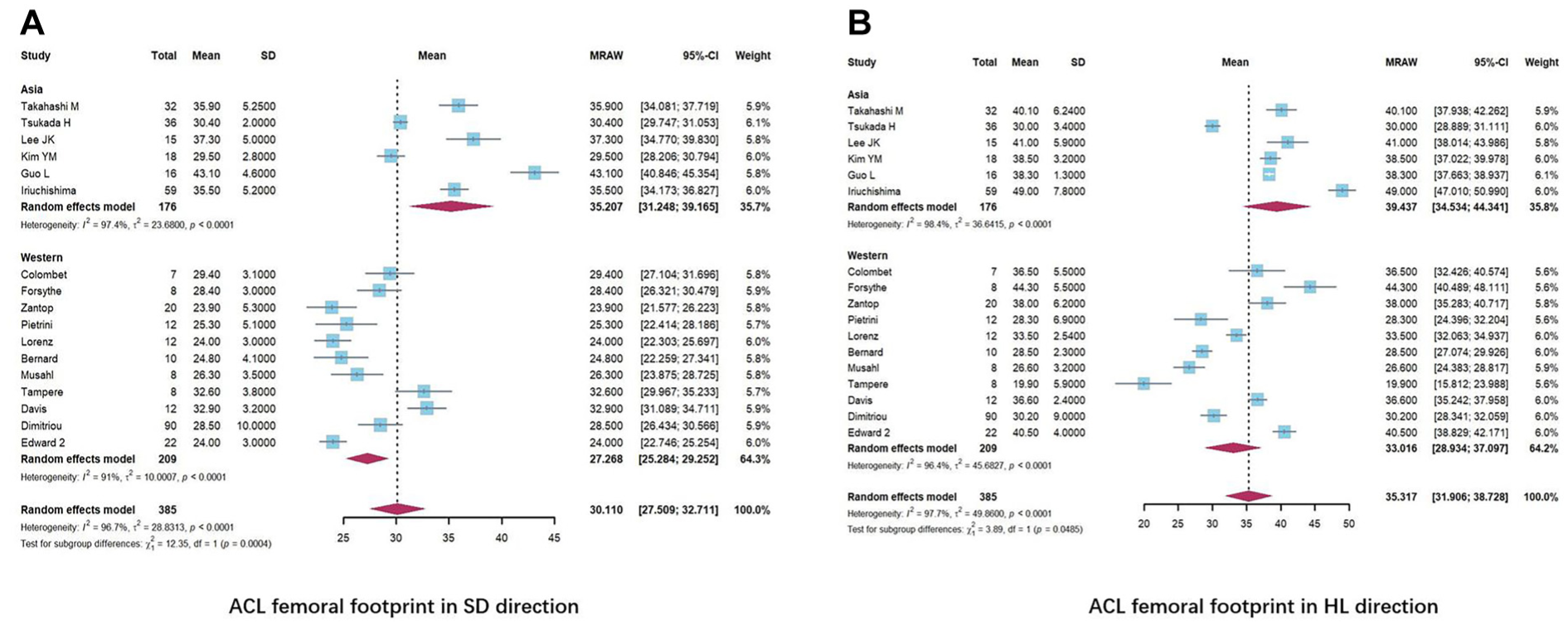
(A) Forest plot of single-arm meta-analysis results for the ACL femoral footprint center location in the SD direction. (B) Forest plot of single-arm meta-analysis results for the ACL femoral footprint center location in the HL direction. ACL, anterior cruciate ligament; HL, high-low; SD, shallow-deep.
For the tibial footprint locations of the entire ACL (Figure 4 with detailed data in supplementary 2), no significant differences were observed between Asian and Western groups in the anteroposterior direction (P = .26) and mediolateral direction (P = .95).
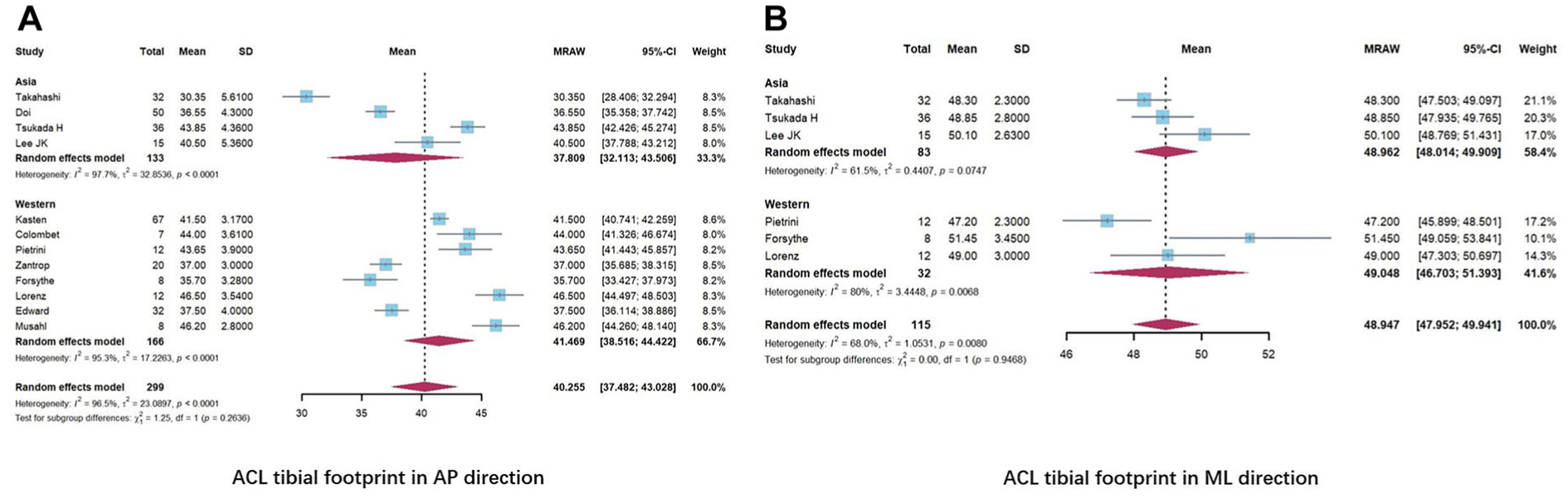
(A) Forest plot of single-arm meta-analysis results for the ACL tibial footprint center location in the AP direction. (B) Forest plot of single-arm meta-analysis results for the ACL tibial footprint center location in the ML direction. ACL, anterior cruciate ligament; AP, anteroposterior; ML, mediolateral.
For the AMB and PLB bundles (Supplementary Figures 6 and 7), (1) a significant difference was observed in the femoral shallow-deep direction (P = .004 and P = .005, respectively); and (2) no significant differences were found in the femoral high-low direction or the tibial anteroposterior and mediolateral directions.
Footprint Size
For the femoral footprint size (Figure 5A; detailed data in Supplementary 3), 17 studies from the Asian group (479 knees) and 12 studies from the Western group (585 knees) were included. The mean area of the ACL femoral footprint was 96.3 mm2 [95% CI, 81.1-111.4] in the Asian group and 126.8 mm2 [95% CI, 103.5-150] in the Western group (P = .03).

(A) Forest plot of single-arm meta-analysis results for ACL femoral footprint size. (B) Forest plot of single-arm meta-analysis results for ACL tibial footprint size. ACL, anterior cruciate ligament.
For the tibial footprint size, 10 studies from the Asian group (301 knees) and 9 studies from the Western group (255 knees) were included (Figure 5B and Supplementary 4). The mean area of the ACL tibial footprint was 125.2 mm2 [95% CI, 115.3-135.2] in Asian and 148 mm2 [95% CI, 123.1-173] in Western groups (P = .09).
Discussion
The most significant findings of our study were that substantial differences in the ACL footprint anatomy between Asian and Western groups were primarily observed on the femoral side—including the location and size of the femoral footprint. Using the quadrant method on the distal femoral lateral condyle, the center of the ACL footprint was located at 32.5% in the Asian group and 27.3% in the Western group from the posterior edge of the lateral condyle. Meanwhile, from the upper border, which corresponds to the Blumensaat line, the distances were 39.4% and 33% in the Asian and the Western groups, respectively.
To our knowledge, this is the first meta-analysis to systematically compare all eligible data from Asian and Western studies regarding ACL footprint anatomy. These results indicate that the ACL femoral insertion in the Asian population is located significantly shallower than in the Western group.To facilitate an understanding of the exact difference regarding ACL femoral footprint locations in clinical practice, our findings can also be interpreted to suggest that the ACL femoral footprint in the Asian population is more anteriorly and distally located. We also found that the total ACL femoral footprint area was significantly smaller in the Asia population.
With the advancement of ACLR techniques, additional surgical considerations arise during surgery—including graft choices and fixation methods.48,64,70 However, placing the femoral and tibial graft tunnels as close as possible to the native ACL insertion, along with appropriate graft size selection, remains crucial for postoperative knee joint stability and functional recovery.68,71 Our study greatly enhances the understanding of ACL footprint anatomy, particularly highlighting an important aspect that may have been overlooked: the significant differences between ethnic groups, which should be considered when performing reconstruction surgeries for patients of different ethnic groups.
Recent ACL anatomy studies40,51,77,79,83 have widely accepted the concept that the ACL ligament is primarily composed of 2 bundles: the AMB and PLB. Therefore, more anatomical data regarding the AMB and PLB bundles have been reported, particularly in the past 10 years. As the most up-to-date data were included in our study, we were able to analyze the footprint locations of both AMB and PLB bundles. Our results revealed that the femoral centers for both bundles were located significantly shallower in the Asia group, consistent with our main finding regarding the ACL femoral footprint location, and further supporting the differences between subgroups.
The ideal location for the femoral tunnel in anatomic ACLR remains controversial. Some recent studies from Aisa18,40,43 have found that the outcomes of ACL femoral footprint location tend to be shallower than reported in earlier data. Lee etal 40 suggested that this discrepancy could be due to the technical evolution of measurement methods in the 21st century. As a result, some previous systematic reviews intentionally excluded studies before 2000. However, as we observed, several studies2,20,56 published before the 21st century, which were included in the current study, used reasonable cadaveric resources and the same quadrant measurement method. Intentionally excluding these studies could introduce potential selection bias.
A recent 3D-MRI reconstruction study from Asia also reported femoral footprint locations that were 25% and 45% and 23.8% and 37.3% in the deep-shallow direction and 41% and 48% and 26.6% and 44.3% in the high-low direction, for Asian and Western groups, respectively. 43 The authors described this tendency for Asian femoral footprints but did not further analyze the underlying reasons. Notably, the 2 earlier studies they compared with were both conducted in Western countries (Norway and the USA).62,66
For the tibial footprint, no significant differences were found in either the footprint location or size. In the mediolateral direction, the footprint center was located almost in the middle of the tibial plateau, with a distance of 49% from the medial edge of the tibial plateau for both the Asian and Western groups. In the anteroposterior (AP) direction, there was also no significant difference regarding the footprint center. However, caution should be exercised when interpreting results in the AP direction, as differences in the definition of the anterior tibial ridge across studies may affect the accuracy of the findings. The study by Tsukada etal 83 in the Asian group and by Zantop etal 87 in the Western group applied the Staubli method, while other studies used the Amis and Jakob method 75 (Figure 6). After excluding the 2 studies that used the Staubli method, no significant difference was found between the subgroups.

Comparison of 2 methods for defining the tibial anterior ridge.
Our results indicated that, based on the quadrant method, the femoral footprint center in Asians is, on average, 7.9% shallower and 6.4% lower than in Western populations. According to Moon etal, 53 the fitting rectangle for the distal lateral femoral condyle using the quadrant method has a mean length of 44 mm for the longer side and 22 mm for the shorter side. Clinically, this suggests that surgeons should place the ACL footprint approximately 3.5 mm shallower and 1.4 mm lower when performing ACLR for Asian patients to align with native anatomy.
Biomechanically, Brophy etal 3 revealed that a more posteriorly located femoral graft is more susceptible to strain during knee extension and internal rotation, contributing to a higher failure rate in the posterolateral bundle of the ACL graft. Given the significant differences in femoral footprint location across ethnic groups observed in our study, we hypothesized that ACLs in different ethnic groups would experience varying tension at specific knee positions. This warrants further biomechanical testing for verification. A large-scale retrospective study by Navarro etal 59 reported that Asian, Hispanic, and Black patients have a lower ACL revision rate compared with White patients. We propose that differences in femoral insertions between races described in our study may be 1 contributing factor.
Previous biomechanical studies have demonstrated that the position of the femoral footprint significantly influences knee stability and graft tension throughout the range of motion.44,67 Loh etal 44 showed that altering the femoral tunnel orientation from the 11 o'clock to the 10 o'clock position—closer to the center of the posterolateral (PL) bundle located more anteriorly and distally—resulted in significantly improved knee stability under rotatory loads. Sakane etal 67 showed that the PL bundle, located more anteriorly and distally, exhibits higher in situ force at lower knee flexion angles (0°-45°). In contrast, the AM bundle has a higher in situ force at higher knee flexion angles (45°-90°). Based on these findings, further biomechanical studies focusing on ethnic differences are warranted to investigate the relationship between femoral footprint variation and knee stability.
Another biomechanical study comparing different ethnic populations found that Japanese individuals exhibit a significantly greater knee flexion angle compared with Caucasians. 41 It would then be reasonable to investigate whether the more anterior and distal positioning of the ACL femoral footprint, as observed in the Asian population, could lead to increased knee flexion among Asians.
One concern in the present meta-analysis is the potential selection bias resulting from the mixture of cadaveric-based measurements ¶ and radiological measurements—including plain radiographs # , 3D CT,16,45,76,80 or MRI reconstructions.10,39,43,74,82 However, previous studies have confirmed that no significant differences exist among these techniques. Lee etal40 specifically designed a study to verify this, concluding that both plain radiographs and 3D CT images showed highly reliable correlations with anatomic dissection measurements, with no significant differences between the methods.
Han etal 19 found that measuring the ACL footprint with 3D MRI or open cadaveric dissection yielded no significant differences and could be used interchangeably. These findings support the notion that selection bias is limited and acceptable, as both radiographic and direct measurement techniques are included in our meta-analysis.
Notably, the baseline characteristics analysis showed that both groups were highly comparable with respect to sex distribution, mean age, and study methods. Specifically, the percentages of knees in each group, as determined by radiographic methods or direct dissection, were similar. This comparability further mitigates the potential bias originating from the inclusion of studies using different techniques. Funnel plots were also generated to evaluate publication bias (Figure 7). The distributions of studies across all 3 analyses appeared generally symmetrical, suggesting a low likelihood of substantial publication bias in this review. Additionally, several authors have reported that the anatomy of the ACL may vary between men and women.47,78 Our analysis indicated no significant difference in sex distribution between the 2 groups, further strengthening the reliability of our findings.

(A) Funnel plot of included studies in the analysis of the femoral footprint size. (B) Funnel plot of included studies in the analysis of the femoral footprint center in the shallow-deep direction.
This study also has certain limitations. First, because not all included studies were randomized controlled trials or cohort studies with control groups, the evidence level is lower, and only a single-arm meta-analysis could be performed. However, this limitation is inherent in the characteristics of previous studies in this field and represents an external factor. Second, as with any single-arm meta-analysis, some results may exhibit a high amount of statistical heterogeneity.52,60 The I2 value in our results indicated that heterogeneity within and between subgroups was significant (>60%). However, because large individual variations in ACL anatomy have been widely reported even within the same ethnic group,5,9,16,79,85 we believe that the high heterogeneity primarily stems from natural anatomic variations of ACLs among individuals, rather than from the limitations of the meta-analysis. Third, according to the bias assessment of the present study, no included studies were identified as having a high risk of bias.
Despite these internal and external limitations, our study is the first meta-analysis to systematically include all eligible quantitative data on ACL footprints and to demonstrate anatomic differences between Asian and Western populations. We believe that these findings will significantly contribute to the development of more precise anatomic reconstruction techniques in the future.
Conclusion
This meta-analysis demonstrated that the ACL femoral footprint in the Asian population is located more anteriorly and distally than in the Western population, and the femoral footprint size is smaller. These findings provide valuable insights for population-specific surgical strategies in the future.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671251397407 – Supplemental material for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations
Supplemental material, sj-docx-1-ojs-10.1177_23259671251397407 for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations by Chen Wang, Ying Ren Mok, Ming Wang, Xin Ma, James Hoi Po Hui and Dave Yee Han Lee in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-docx-2-ojs-10.1177_23259671251397407 – Supplemental material for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations
Supplemental material, sj-docx-2-ojs-10.1177_23259671251397407 for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations by Chen Wang, Ying Ren Mok, Ming Wang, Xin Ma, James Hoi Po Hui and Dave Yee Han Lee in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-docx-3-ojs-10.1177_23259671251397407 – Supplemental material for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations
Supplemental material, sj-docx-3-ojs-10.1177_23259671251397407 for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations by Chen Wang, Ying Ren Mok, Ming Wang, Xin Ma, James Hoi Po Hui and Dave Yee Han Lee in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-docx-4-ojs-10.1177_23259671251397407 – Supplemental material for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations
Supplemental material, sj-docx-4-ojs-10.1177_23259671251397407 for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations by Chen Wang, Ying Ren Mok, Ming Wang, Xin Ma, James Hoi Po Hui and Dave Yee Han Lee in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-docx-5-ojs-10.1177_23259671251397407 – Supplemental material for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations
Supplemental material, sj-docx-5-ojs-10.1177_23259671251397407 for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations by Chen Wang, Ying Ren Mok, Ming Wang, Xin Ma, James Hoi Po Hui and Dave Yee Han Lee in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-jpg-6-ojs-10.1177_23259671251397407 – Supplemental material for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations
Supplemental material, sj-jpg-6-ojs-10.1177_23259671251397407 for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations by Chen Wang, Ying Ren Mok, Ming Wang, Xin Ma, James Hoi Po Hui and Dave Yee Han Lee in Orthopaedic Journal of Sports Medicine
Supplemental Material
sj-jpg-7-ojs-10.1177_23259671251397407 – Supplemental material for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations
Supplemental material, sj-jpg-7-ojs-10.1177_23259671251397407 for Comparative Meta-Analysis of ACL Footprint Anatomy Between Asian and Western Populations by Chen Wang, Ying Ren Mok, Ming Wang, Xin Ma, James Hoi Po Hui and Dave Yee Han Lee in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted August 24, 2025; accepted September 24, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.