
Abstract
Background:
Professional soccer players are exposed to considerable impact on the knee during growth that may affect bone morphology and accessory ossicles.
Purpose:
To identify differences in knee bone morphology, including accessory ossicle development, between soccer players and controls.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
The soccer group included male professional soccer players (n = 334 knees) who had medical checkups at the authors’ hospital from 2013 to 2023. Controls were male, age-matched patients at the same hospital (n = 223 knees). Knee radiographs (bilateral anteroposterior, lateral, and sky-line views) were obtained from patients. Each radiograph was evaluated to determine the Insall-Salvati ratio, tuberosity height ratio (THR), posterior tibial slope (PTS), ossicles associated with Osgood-Schlatter disease (OOSDs), Sinding-Larsen-Johansson disease, and bipartite patella (BP).
Results:
The soccer group had a significantly higher THR (0.276), PTS (9.42°), and incidences of OOSD (10.8%) and BP (6.3%) than the control group (0.213, 8.23°, 3.1%, and 0.45%, respectively) (P < .001, P < .001, P = .002, and P = .001, respectively). In the soccer group, THR and PTS were significantly higher on the dominant side (0.289 and 9.84°, respectively) than on the nondominant side (0.269 and 9.0°, respectively) (P = .049 and P = .009, respectively).
Conclusion:
Elite male soccer players had a larger prominence on the tibial tuberosity, steeper PTS, and higher OOSD and BP incidence. Additionally, they had greater tibial tuberosity prominence and PTS on the dominant side. These findings suggest that repetitive mechanical loading during growth may influence knee bone morphology.
Keywords
Early specialization is controversial across multiple sports. Research in baseball suggests that the practice is associated with a relatively high frequency of serious injuries.1,38 In soccer, professional players begin training for their career at a young age and thus experience considerable knee stress from childhood, particularly on the tibial tuberosity and patella.7,15,22 Although soccer players have a higher prevalence of genu varum, few reports are available on other characteristic bone morphological features, such as accessory ossicles.12,39 Notably, knee extension stress affects the posterior tibial slope (PTS). 9 A steeper PTS has been associated with an increased risk of anterior cruciate ligament (ACL) injury, and thus has attracted significant clinical and research attention.27,36 Furthermore, although forceful concentric contraction of the quadriceps produces shear stress in the anterior proximal tibia through the patellar tendon and ACL,21,35 no reports clearly demonstrate the relationship between this stress and prominence size on the tibial tuberosity. While intense sports activities during the growth period have been associated with cam-type deformity of the femoral head and humeral retrotorsion, such investigations have not been conducted for the knee.10,23,30,31
Accessory ossicles affecting the knee extension mechanism include those associated with Osgood-Schlatter disease (OSD), Sinding-Larsen-Johansson disease (SLJD), and bipartite patella (BP). In patients with OSD, secondary ossification centers on the tibial tuberosity often develop into ossicles (ossicles associated with OSD [OOSDs]).3,6,24 While surgery is rarely required for OSD, 31 intervention may be necessary to treat residual symptoms from OOSD.4,11,24 SLJD typically occurs in 10- to 14-year-old boys and develops through repeated traction of the patellar tendon on the infrapatellar pole during quadriceps contraction, a common movement in sports such as soccer, volleyball, and gymnastic.32,37 Finally, BP develops when secondary ossification centers fail to fuse. Most common in athletes, it has a 0.6% to 2% incidence and a 2% symptomatic rate.16-18 Although the symptomatic rate is relatively low, such ossicles may become clinically significant in athletes due to high functional demands.
To better understand how professional soccer affects its players’ knee bone morphology, including accessory ossicle number, we compared these traits between soccer players and controls. We hypothesized that male professional soccer players would have a greater prominence on the tibial tuberosity, steeper PTS, and higher OOSD, SLJD, and BP incidences.
Methods
Study Population
This study was approved by the ethics committee and institutional review board of our hospital (ID No. 2023-27). The soccer group consisted of professional male soccer players belonging to teams in the Meiji Yasuda J1 League (aged 16-35 years) who underwent medical checkups at the hospital from 2013 to 2023, with the most recent data used in cases of multiple visits. Female soccer players were not investigated in this study. The checkups included obtaining player data (age, height, weight, and playing position) and radiographs showing the bilateral anteroposterior, lateral, and sky-line views of the knee. The control group consisted of age-matched male patients with knee radiographs of the same 3 views, taken during the years 2016 to 2023. Patients with patellar dislocation (n = 5), collagen disease with bone lesions (n = 2), or ACL reconstruction using a bone–patellar tendon–bone graft (n = 2) were excluded from the control group. In addition, we excluded individuals with known histories of participation in organized sports at a professional or elite level.
Radiographic Analysis
Measurements of PTS followed a previously reported method, using standard lateral radiographs of the proximal tibia (Figure 1). 9 To evaluate the prominence of the tibial tuberosity, the tuberosity height ratio (THR) was measured using a method previously reported by Visuri et al 33 (Figure 1).

Lateral radiograph showing the measurement method for the tuberosity height ratio (THR) and posterior tibial slope (PTS). The THR is b divided by a. a: distance from the yellow line (representing tibial axis throug the midpoint [red dot] at 5 and 10 cm from the joint line) to the blue line (representing the tangent of the anterior margin of the tibia); b: distance from the blue line to the tibial tuberosity tip. The PTS is the angle between the red line (perpendicular to the yellow line) and the green line (tangent to the medial tibial plateau).
Knee radiographs were used to determine OOSD, SLJD, and BP incidence (Figure 2). These variables, along with the incidence of accessory ossicles, were compared between the soccer and control groups. The Insall-Salvati ratio (ISR) was also measured following published methods. 24

Representative images of bone lesions on knee joint radiographs. (A) Lateral radiograph showing ossicle associated with Osgood-Schlatter disease (arrow). (B) Lateral radiograph showing Sinding-Larsen-Johansson disease (arrowhead). (C) Anteroposterior and sky-line view radiographs showing the bipartite patella (arrows).
Radiographs were examined by 2 orthopaedic surgeons (T.K., R.S.). Each measurement was performed twice by one examiner with a >3-month interval to calculate intraobserver reliability, and once independently by a second examiner to calculate interobserver reliability.
In the soccer group, the variables above were compared between the dominant and nondominant sides. In the soccer group, leg dominance was determined based on the self-reported preferred kicking leg, or confirmed using information available on the official team website.
Statistical Analysis
Between-group differences in knee morphological measurements were determined using Student t tests. The Pearson chi-square test evaluated between-group differences in accessory ossicle incidence. Significance was set at a P value <.05. Interclass correlation coefficients were assessed by 2 researchers (T.K., R.S.), whereas intraclass correlation coefficients were assessed twice (with a >3-month separation) by a single researcher (T.K.). The 95% confidence interval and standard errors of kappa were calculated. All analyses were performed in EZR Version 1.61 (Saitama Medical Center, Jichi Medical University, Saitama, Japan). 13
Results
We examined 334 and 223 knees from the soccer and control groups, respectively. The mean ages of the soccer and control groups, 23.6 years (range, 16-35 years) and 24.7 years (range, 16-35 years), respectively, did not exhibit a significant difference (P = .050) (Table 1). Participants in the soccer group started playing at a mean age of 6.2 years. The mean height was significantly greater in the soccer group (178 ± 7.67 cm) compared with the control group (172 ± 5.91 cm) (P < .001). The mean body weight was 71.3 ± 7.78 kg in the soccer group and 70.0 ± 12.5 kg in the control group, with no significant difference observed (P = .150). The playing position distribution in the soccer group was as follows: forwards (19.7%), midfielders (39.5%), defenders (27.5%) and goalkeepers (13.2%).
Comparison of Characteristics Between the Soccer and Control Groups

The soccer group had significantly higher THR, PTS, and incidence of OOSD and BP than the control group (P < .001, P < .001, P = .002, and P = .001, respectively) (Table 2). There were no significant differences in ISR (P = .307) or SLJD incidence (P = .664) between the soccer and control groups (Table 2). In the soccer group, THR and PTS were significantly higher on the dominant side than on the nondominant side (P = .049 and P = .009, respectively) (Table 3). Representative radiographs of the soccer and control groups are presented in Figure 3.
Comparison of Bone Morphology Parameters and Incidence Rates of Accessory Ossicles Between the Soccer and Control Groups a
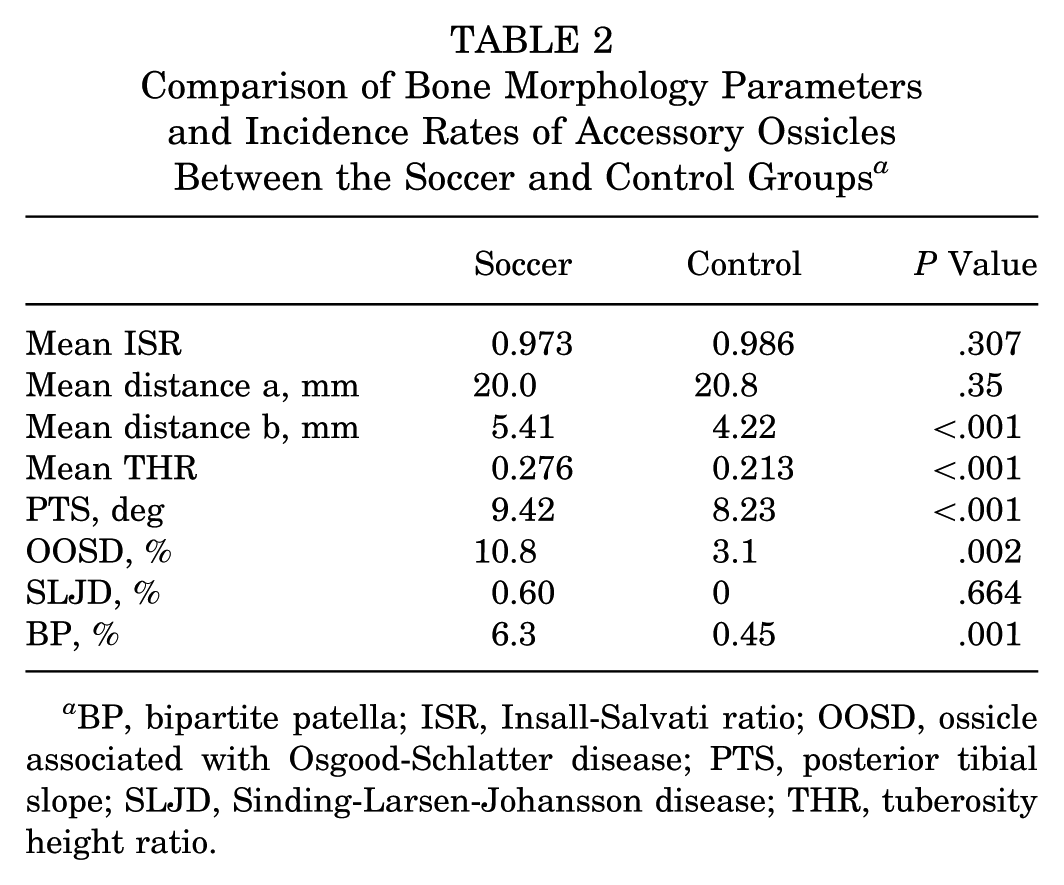
BP, bipartite patella; ISR, Insall-Salvati ratio; OOSD, ossicle associated with Osgood-Schlatter disease; PTS, posterior tibial slope; SLJD, Sinding-Larsen-Johansson disease; THR, tuberosity height ratio.
Comparison of Bone Morphology Parameters and Incidence Rates of Accessory Ossicles on the Dominant and Nondominant Sides in the Soccer Group a
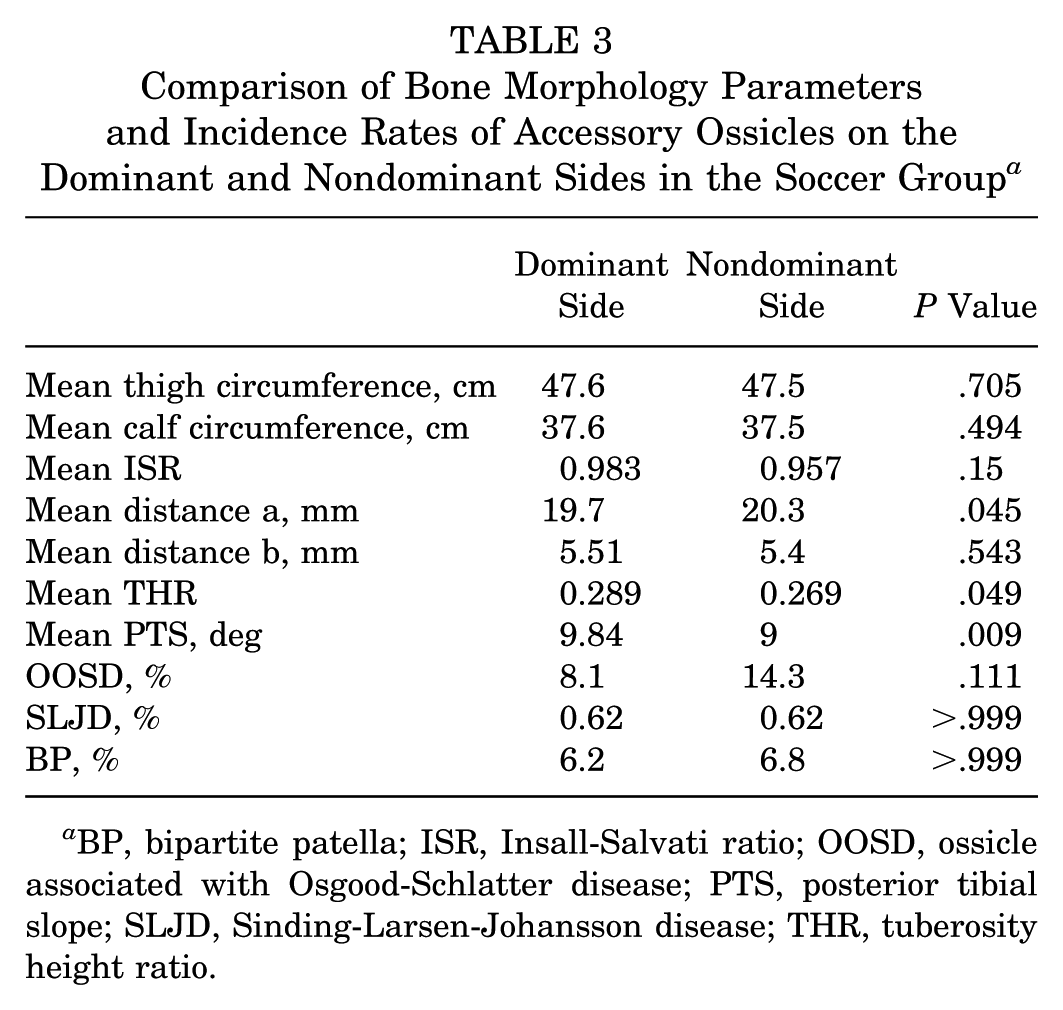
BP, bipartite patella; ISR, Insall-Salvati ratio; OOSD, ossicle associated with Osgood-Schlatter disease; PTS, posterior tibial slope; SLJD, Sinding-Larsen-Johansson disease; THR, tuberosity height ratio.

Representative images showing the knee bone morphology of the soccer (A and B) and control (C) groups. (A) A characteristic case in the soccer group with a large prominence on the tibial tuberosity and substantial posterior tibial slope (PTS). (B) Another representative case in the soccer group with enlarged prominence on the tibial tuberosity and steeper PTS. (C) A representative case in the control group with normal tibial tuberosity and PTS.
Table 4 shows intraclass correlation coefficients for the inter- and intraobserver reliability per parameter. Table 5 shows the interobserver reliability for detecting accessory ossicles.
ICCs for Interobserver and Intraobserver Reliability of Each Parameter a

ICC, intraclass correlation coefficient; ISR, Insall-Salvati ratio; PTS, posterior tibial slope; THR, tuberosity height ratio.
Interobserver Reliability for the Detection of Accessory Ossicles a

BP, bipartite patella; OOSD, ossicle associated with Osgood-Schlatter disease; SLJD, Sinding-Larsen-Johansson disease.
Discussion
Supporting our hypothesis, we demonstrated that male professional soccer players exhibited a larger prominence on the tibial tuberosity, greater PTS, and higher OOSD and BP incidence. These changes may result from quadriceps muscle traction on the superior patella, traction of the tibial tuberosity via the patellar tendon, and traction of the anterior tibial plateau through the ACL, all common occurrences during typical soccer motions (Figure 4A). In particular, kicks involving forceful contact with a rapidly approaching ball impose considerable mechanical stress on the tibial tuberosity (Figure 4B). This mechanical stress may be greater on the dominant leg, which is more frequently used for kicking. Supporting this, Gaulrapp and Nührenbörger 7 reported a significantly higher incidence of OSD in the dominant leg among adolescent soccer players. Excessive stress on the epiphyseal cartilage before epiphysis closure can alter bone morphology, including humeral retrotorsion, prevalent in baseball, and proximal femoral cam deformity, more commonly observed in soccer and basketball.19,23
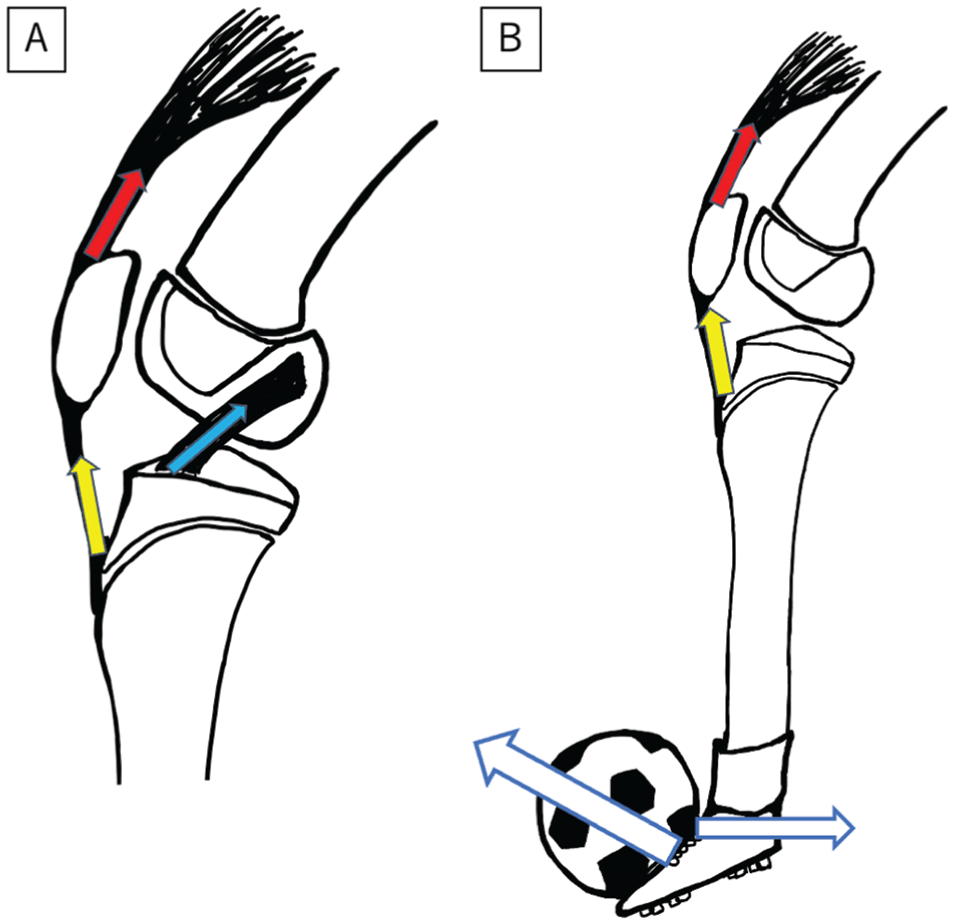
Schematic illustrating the knee loading mechanism in soccer players. (A) Traction of the quadriceps muscle on the superior patella (red arrow), traction on the tibial tuberosity through the patellar tendon (yellow arrow), and traction on the anterior tibial plateau via the anterior cruciate ligament (blue arrow) occur during soccer motions. (B) Kicks involving forceful contact with a rapidly approaching ball impose considerable mechanical stress on the tibial tuberosity.
Similarly, stress on the tibial epiphysis can enlarge the prominence on the tibial tuberosity and increase PTS. Both of these conditions are further exacerbated by forceful eccentric contraction of the quadriceps. This mechanical action produces shear stress in the anterior proximal tibia via the patellar tendon and ACL, thus causing flexion-type Salter-Harris type 2 and Watson-Jones type 4 fractures.21,35 Other contributors include loading the anterior portion of the tibia through the extensor mechanism via the patellar tendon.9,25 Patients with OSD and tibial tuberosity fractures have steeper PTS, 29 in turn increasing tibial shear force, anterior tibial translation, and ACL load. 28 These changes further increase the prominence on the tibial tuberosity and PTS, generating a negative cycle. A steeper PTS is also associated with ACL injury,27,36 a high risk in soccer players. 8 Moreover, previous studies have shown that a greater PTS is associated not only with an increased risk of primary ACL injury but also with a higher risk of graft failure after ACL reconstruction. 27
Tibial tuberosity ossification typically appears at 10 years of age, extends by 14 years of age, and fuses by 16 years of age. 20 The ossification center of the BP appears at 10 to 12 years of age. 20 In soccer players, heavy foot and ankle loading from childhood appears to increase accessory ossicle incidence in these regions. 14 The elevated incidence of OOSD and BP in our soccer group may thus stem from childhood loading on the tibial tuberosity and patella. Both OOSD and BP can be symptomatic (the latter in 2% of cases), predominantly in athletes.11,17,18
In soccer players, injuries are generally more common in the dominant leg regardless of sex. 3 However, ACL injuries are occurring more frequently in the nondominant (support) leg for women and the dominant leg for men.2,5,26,34 Our study demonstrated that male soccer players had a steeper PTS in the dominant leg. This characteristic is associated with a higher risk of ACL injury27,36 and may explain higher occurrence in the dominant leg for men. In contrast, OSD tends to be more common in the support leg of soccer players.7,34 Finally, to the best of our knowledge, this was the first study that investigated OOSD incidence rate; we did not find a significant difference in OOSD occurrence between the dominant and nondominant legs.
Limitations
This study had several limitations. First, we only examined male participants. Second, some control participants may have played soccer or similar sports in childhood, and their activity level was unclear. In addition, patients with a history of ACL reconstruction were not excluded, which may represent a potential source of selection bias. Third, the soccer group had a significantly greater mean height compared with the control group. Because body size may influence tibial morphology, this difference represents a potential confounding factor and should be considered when interpreting the morphological comparisons between groups. Fourth, the PTS was measured using the proximal portion of the tibia only, which may not reflect the alignment of the entire tibia and represents a methodological limitation. Fifth, data on clinical symptoms were not consistently available and thus were not analyzed in this study. Finally, the cross-sectional design meant causal relationships were unclear.
Conclusion
Elite male soccer players had greater prominence of the tibial tuberosity, steeper PTS, and a higher incidence of OOSD and BP. Additionally, they had greater tibial tuberosity prominence and PTS on the dominant side. These findings suggest that repetitive mechanical loading during growth may influence knee bone morphology.
Footnotes
Final revision submitted September 1, 2025; accepted September 24, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from (ID No. 2023-27).