
Abstract
Background:
Although acellular dermal matrix (ADM) patch augmentation is known to reduce retear rates compared with repair without augmentation, clinical outcomes have varied across previous studies due to cohort heterogeneity.
Hypothesis:
ADM patch augmentation would lead to improved outcomes compared with single-row repair alone in a propensity score–matched cohort of patients with large-to-massive rotator cuff tear.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective study investigated patients who underwent arthroscopic rotator cuff repair for large-to-massive posterosuperior tears between March 2019 and February 2024. Propensity score matching was performed to minimize selection bias, resulting in 32 patients each in the group that had single-row repair and the group that had single-row repair with ADM patch augmentation. Clinical outcomes and range of motion were compared at the 2-year follow-up. Structural integrity was assessed using magnetic resonance imaging at the 6-month follow-up. Multivariate logistic regression was conducted on the entire cohort to quantify the efficacy of patch augmentation in improving structural integrity.
Results:
After propensity matching, the baseline characteristics were similar between groups. Both groups demonstrated significant improvements in clinical outcomes and range of motion compared with preoperative status (all P < .001). Clinical outcomes and range of motion did not differ significantly between groups. However, the retear rate was significantly lower in the ADM patch augmentation group (12.5%) compared with the matched single-row repair group (34.4%; P = .039). In the multivariate analysis of the entire cohort of 160 patients, ADM patch augmentation showed reduced odds of retear compared with single-row repair alone (odds ratio, 0.292; P = .013).
Conclusion:
In large-to-massive rotator cuff tears, ADM patch augmentation appeared to play a protective role in maintaining structural integrity. However, further studies are warranted to evaluate its long-term clinical outcomes.
Large-to-massive rotator cuff tears (RCTs) pose significant challenges due to severe tendon retraction, poor tissue quality characterized by fatty infiltration, and reduced vascularity. As a result, these tears remain associated with high retear rates ranging from 34% to 94%,9,14 and clinical outcomes remain suboptimal at mid- to long-term follow-up.18,36 To address these difficulties, advanced arthroscopic techniques such as aggressive interval release, tendon medialization, and muscle advancement have been developed.12,22,25,27,28 Although these methods improve intraoperative tendon mobility, they do not fully resolve fundamental issues, including compromised tendon quality and insufficient tendon remnants.
To augment the healing environment, acellular dermal matrix (ADM) patches have been introduced as biological scaffolds that facilitate tenocyte migration, neovascularization, and extracellular matrix remodeling.17,37 Biomechanical studies have shown that ADM augmentation can enhance the initial load to failure and reduce gap formation, offering potential benefits in both mechanical protection and biological support during early healing.19,33 Despite promising biomechanical and histologic data, clinical studies on ADM patch augmentation report mixed outcomes. 34 Some randomized controlled trials and cohort studies have indicated reduced retear rates and improved shoulder function, especially in large or revision tears.3,10,32 However, others have found no significant improvement in clinical scores or range of motion (ROM) compared with standard repair.6,7,39 Given the high failure rate of conventional repairs in large-to-massive RCTs and the increasing use of ADM patches, further investigation is needed. In particular, studies that control for confounding variables are essential to determine the true efficacy of ADM augmentation.
The purpose of this study was to compare the clinical, functional, and radiologic outcomes of single-row repair versus ADM patch augmentation in large-to-massive RCTs. We hypothesized that the use of ADM augmentation would lead to improved outcomes compared with a matched cohort treated with single-row repair alone.
Methods
Study Population
This retrospective study investigated patients who underwent arthroscopic rotator cuff repair for posterosuperior tears at a single institution between March 2019 and February 2024. Surgical indications included persistent pain or functional impairment that did not improve after a minimum of 6 months of nonoperative treatment. Single-row repair was performed in the early phase, and ADM augmentation was adopted later for large-to-massive RCTs upon the availability of ADM. Patients with large-to-massive RCTs confirmed intraoperatively who underwent either single-row repair or repair with patch augmentation were included in this study. The exclusion criteria were as follows: (1) <2 years of follow-up after surgery (n = 21); (2) partial repair (n = 5); (3) revision surgery (n = 2); (4) absence of postoperative magnetic resonance imaging (MRI) evaluation (n = 18); and (5) evidence of subscapularis retear on follow-up MRI (n = 4). Ultimately, 160 patients were included in the final analysis. Institutional review board approval was obtained, and the requirement for informed consent was waived.
Radiologic and Functional Evaluations
Preoperative MRI scans were obtained using a 3.0-T system (Magnetom Tim Trio; Siemens) to evaluate RCT size and the degree of fatty infiltration. Fatty infiltration was assessed on the most lateral T1-weighted sagittal oblique slice at the junction of the scapular spine and body using the Goutallier classification as applied by Fuchs et al 13 to MRI. Postoperative MRI was performed at 6 months after surgery to evaluate tendon integrity, with healing status classified according to the Sugaya classification; types 4 and 5 were considered indicative of a retear. 38
Two fellowship-trained shoulder orthopaedic surgeons independently assessed fatty infiltration and tendon healing twice, with a 4-week interval between evaluations. In cases of disagreement between the 2 observers, the final decision was made by the senior surgeon.
Functional outcomes were evaluated preoperatively and at the 2-year follow-up using the visual analog scale for pain, the American Shoulder and Elbow Surgeons (ASES) score, the University of California–Los Angeles score, and the Subjective Shoulder Value. ROM measurements included active forward flexion in the scapular plane, external rotation at the side, and internal rotation to the highest spinal level reached. Internal rotation levels were converted to numeric scores for statistical comparison (eg, T1-T12 = 1-12, L1-L5 = 13-17, sacrum = 18). 24
Surgical Technique
All arthroscopic rotator cuff repairs were performed by a single surgeon with the patient positioned in the beach-chair position under general anesthesia. Initial diagnostic arthroscopy was conducted through a standard posterior portal to assess the presence of subscapularis tendon tears and other intra-articular abnormalities. In cases with suspected subscapularis involvement, a 70° arthroscope was used, and the arm was placed in internal rotation to enhance visualization. For Lafosse grade I subscapularis tears involving <50% of the tendon thickness, simple debridement was performed. For Lafosse grade I tears involving >50% of the tendon thickness, repair was carried out using 1 or 2 suture anchors, depending on the extent of the tear. When degenerative changes of the long head of the biceps tendon were identified, biceps tenotomy or tenodesis was performed. Subsequent evaluations of the tear configuration and tendon mobility were carried out from the lateral portal within the subacromial space. The torn and retracted supraspinatus tendon was pulled toward its anatomic footprint to assess potential coverage. If full coverage of the footprint was not achievable without excessive tension, suture anchors were placed as medially as possible within the medial half of the footprint to reduce tension after the repair. Using a suture passer through the anterolateral portal, the surgeon repaired tendon in a simple, single-row fashion.
In the patch augmentation group, after the initial repair was completed, the residual footprint defect was measured precisely using an arthroscopic probe. On the back table, a 3 to 4 mm–thick ADM was selected and trimmed to the dimensions of the uncovered footprint defect as measured intraoperatively. A medial traction suture was inserted through the Neviaser portal and passed between the supraspinatus and infraspinatus tendons. The medial traction suture was passed through the medial side of the graft to facilitate delivery (Figure 1). Two of the sutures were used for single-row repair, and the remaining suture was used to place mattress sutures at the anteromedial and posteromedial aspects. The patch was introduced through an anterolateral portal using a cannula to establish a passage. All sutures were retrieved and carefully aligned to prevent entanglement. The surgeon gently delivered the ADM into the subacromial space using a knot pusher while simultaneously pulling the traction sutures to guide the patch into position. Once the patch was seated over the repaired rotator cuff, the medial side was secured using the prepositioned traction sutures. The lateral side was then fixed using 2 knotless anchors in a suture-bridge configuration, securing both the rotator cuff and the patch together.
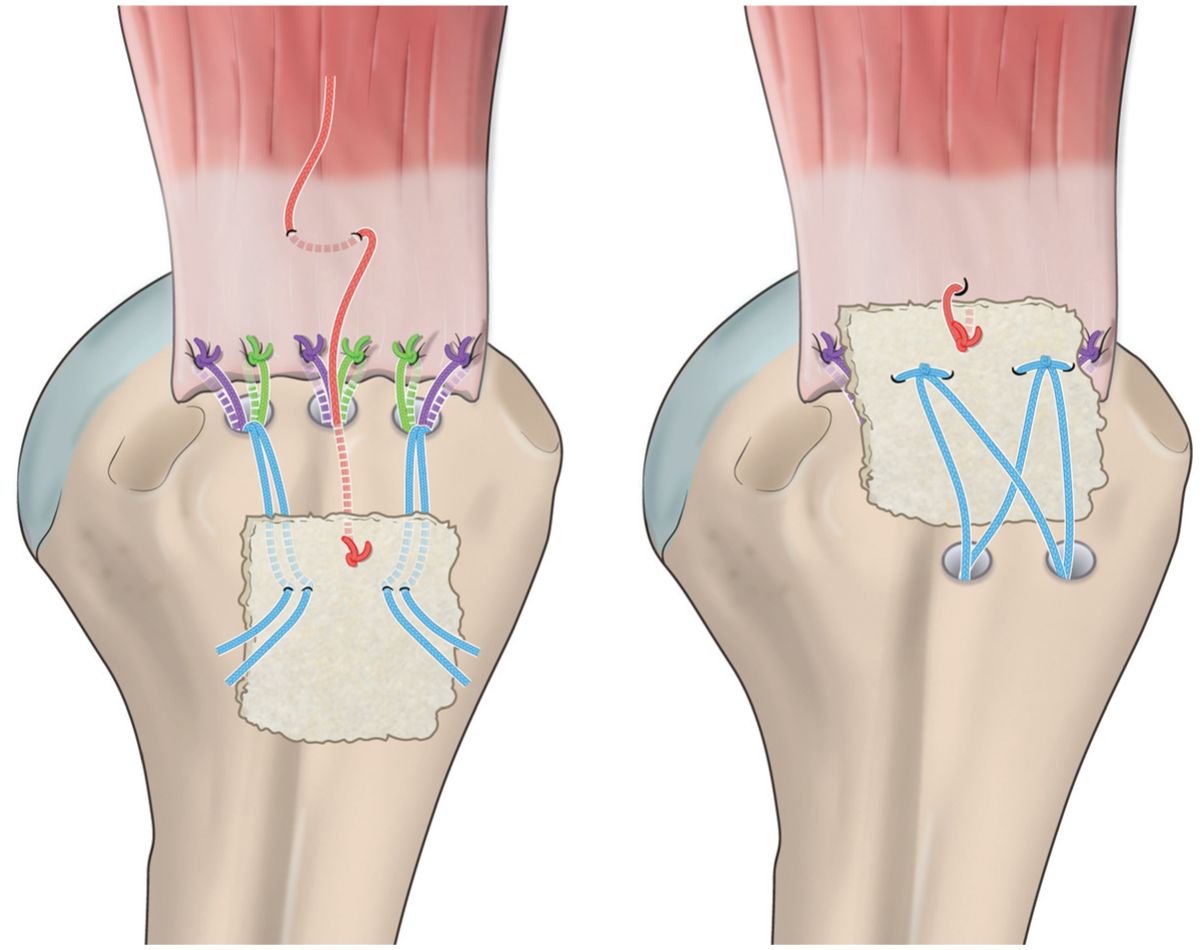
Illustration of the surgical technique. (Left) A traction suture was passed through the medial side of the graft to facilitate delivery, and 1 pair of sutures from each triple-loaded anterior and posterior anchor was passed through the graft. (Right) The traction suture and medial anchor sutures were tied, followed by fixation of the graft with lateral anchors.
Postoperative Rehabilitation
Patients were immobilized in an abduction brace for 6 weeks postoperatively. Passive stretching exercises were initiated thereafter, followed by active-assisted ROM at 8 weeks and isotonic strengthening at 3 months. Return to full activity and sports participation were allowed after 6 months, depending on individual recovery.
Statistical Analysis
To ensure sufficient statistical power for comparative analysis after propensity score matching, a sample size estimation was conducted. Based on an expected minimal clinically important difference of 12 points on the ASES score and assuming a power of 80% and an alpha of .05, a minimum of 32 matched pairs was deemed necessary to detect a clinically meaningful difference.11,31
Propensity score matching is a statistical technique used to reduce confounding by estimating the probability of assignment to a specific group and matching participants based on covariates to achieve balance between groups.2,5 In this study, a 1:1 propensity score matching was conducted, resulting in 32 matched participants in both the single-row repair group and the patch augmentation group. Matching was based on key prognostic factors for rotator cuff healing, which included age, sex, smoking status, and the degree of fatty infiltration.23,40
The normality of continuous variables was assessed using the Shapiro-Wilk test. For paired comparisons, either the paired t test or the Wilcoxon signed-rank test was applied, depending on the normality of the data. For independent comparisons, either the independent t test or the Mann-Whitney U test was used, as appropriate. Categorical variables were analyzed using either the chi-square test or Fisher exact test. Univariate logistic regression analysis was performed on the entire cohort to identify factors associated with retear, and multivariate logistic regression was subsequently used to adjust for potential confounding variables and to determine whether ADM augmentation remained a protective factor against retear. Multicollinearity was assessed using variance inflation factors; variables with variance inflation factors >10 were excluded from the analysis. Interrater reliability between 2 fellowship-trained shoulder surgeons for MRI assessments, including tendon retear and fatty infiltration grading, was evaluated using weighted Cohen κ. Weighted Cohen κ values were 0.79 for posterosuperior cuff retear, 0.72 for subscapularis retear, and 0.81, 0.79, and 0.72 for fatty infiltration of the supraspinatus, infraspinatus, and subscapularis, respectively. All statistical analyses were performed using SPSS Version 27.0 (IBM Corp), with statistical significance set at P < .05 and a 95% CI.
Results
A total of 128 patients underwent single-row repair, and 32 received patch augmentation (Table 1). Among the baseline characteristics, the sex distribution was significantly different between the groups (P = .031). After propensity score matching, 32 patients were included in each group (Table 2). No statistical differences were found in patient characteristics between the groups.
Comparison of Single-Row Repair and Patch Augmentation Groups a

Data are presented as mean ± SD or n (%).
Tear size was assessed arthroscopically according to the Lafosse classification.
Grade of fatty infiltration was determined based on magnetic resonance imaging findings using the Goutallier classification.
Characteristics of Matched Single-Row Repair and Patch Augmentation Groups a

Data are presented as mean ± SD or n (%).
Tear size was assessed arthroscopically according to the Lafosse classification.
Grade of fatty infiltration was determined based on magnetic resonance imaging findings using the Goutallier classification.
Preoperatively, the matched single-row repair and patch augmentation groups showed no significant differences in functional outcomes or ROM (Table 3). At the 2-year follow-up, both groups showed improvements in functional outcomes and ROM compared with their preoperative status (P < .001 for all values), with no significant differences between the groups.
Functional Outcomes of Matched Single-Row Repair and Patch Augmentation Groups a

ASES, American Shoulder and Elbow Surgeons; SSV, subjective shoulder value; UCLA, University of California–Los Angeles; VAS, visual analog scale. Data are expressed as mean ± SD.
The retear rate was significantly lower in the patch augmentation group than in the matched single-row repair group (Table 4). To further validate this finding, we conducted univariate and subsequent multivariable logistic regression analyses on the entire cohort of 160 patients to identify factors associated with retear (Table 5). After adjustment for potential confounders, patch augmentation remained significantly protective, with an odds ratio of 0.263 (P = .018). Among patients in the patch augmentation group, patch margin folding was observed on postoperative MRI in 3 patients (9.4%), and subacromial bursitis was noted in 2 patients (6.2%) (Figure 2). However, the structural integrity of the repair was maintained in all cases.
Comparison of Retear Rates for the Matched Single-Row Repair and Patch Augmentation Groups a

Data are expressed as n (%).
Regression Analysis of Factors Associated With Retear After Rotator Cuff Repair

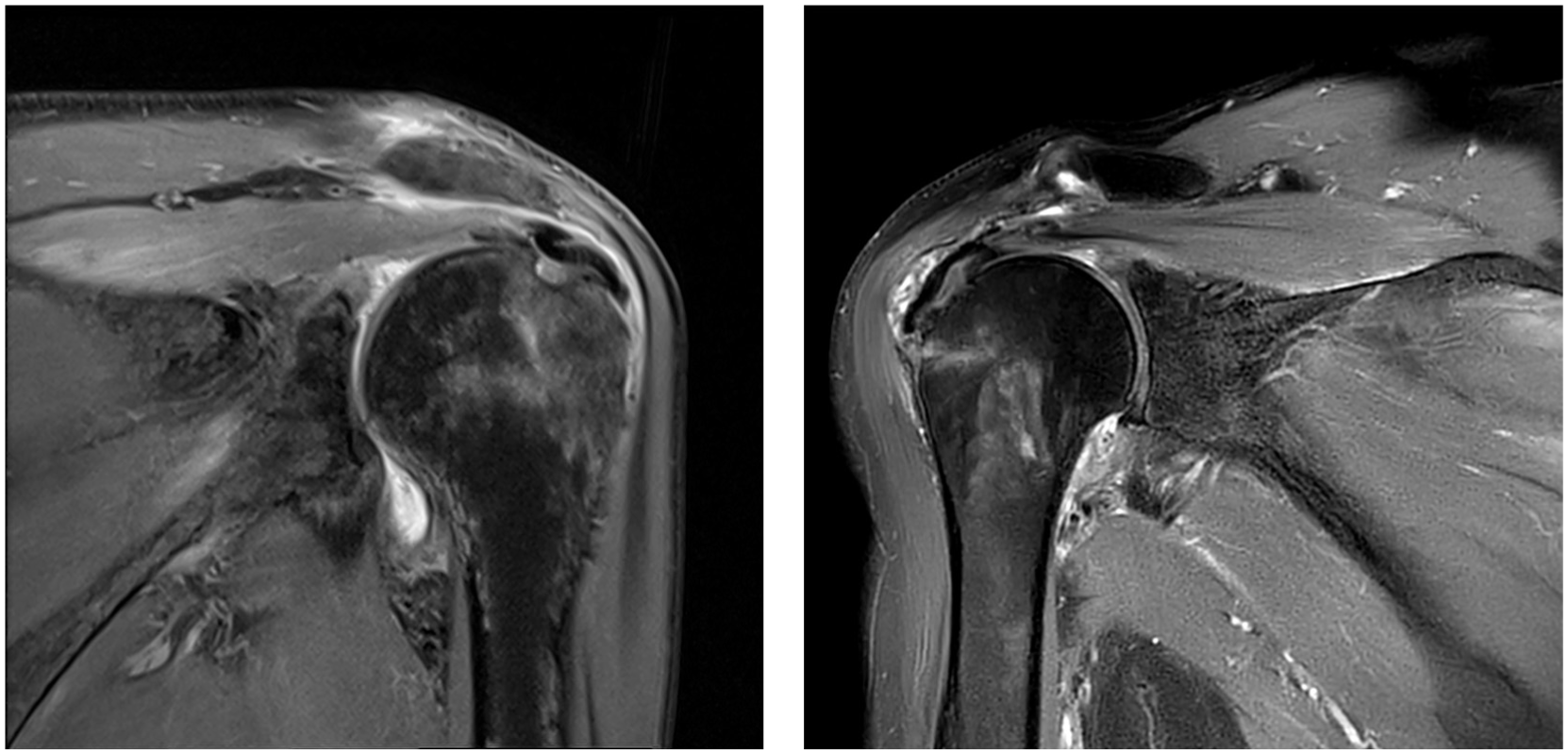
Marginal folding of the graft (left) and subacromial bursitis (right) observed on the 6-month follow-up magnetic resonance imaging scan.
Discussion
The primary finding of this study is that ADM patch augmentation played a protective role in maintaining structural integrity after the repair of large-to-massive RCTs. This protective effect not only was confirmed through propensity score-matched analysis but also was quantified using multivariate logistic regression across the entire cohort. Even after adjustment for potential confounders, ADM augmentation significantly reduced the odds of retear by approximately 73% (odds ratio, 0.263), underscoring its biomechanical and biological efficacy. However, this improvement in tendon integrity did not directly translate into superior functional outcomes at the 2-year follow-up.
The structural benefit of patch augmentation is further supported by biomechanical evidence. Large-to-massive tears typically involve substantial tendon retraction, leading to high tensile stress at the repair site and predisposing to failure. ADM augmentation helps mitigate this stress by distributing loads across the repair construct. McCarron et al29,30 demonstrated that augmented repairs had greater load to failure and reduced gap formation in cadaveric models, and Barber et al 4 found that dermal grafts improved footprint contact and pressure, enhancing the mechanical environment for healing. Acting as an internal brace, the ADM patch supports early repair strength while also promoting biological integration through host cell infiltration and neovascularization.1,8,37
Previous clinical studies have reported similarly reduced retear rates with patch augmentation, particularly in large or massive tears.15,21 Orozco et al 34 recently conducted a systematic review of randomized clinical trials and concluded that ADM augmentation was associated with a significantly lower incidence of retears. Despite these encouraging structural results, functional outcomes remained inconsistent across studies. This variability may be attributed to heterogeneity in study design, including differences in graft material (eg, submucosal tissue, dermal allografts, and xenografts) and the wide range of surgical indications (from small to irreparable tears). 34 Unlike many prior investigations, the present study minimizes selection bias through propensity score matching, controlling for critical prognostic variables such as age, sex, smoking status, and fatty infiltration. This methodological rigor provides a more reliable estimate of the true clinical value of ADM augmentation. Furthermore, the use of multivariate analysis in the full cohort allowed not only confirmation of the protective effect but also quantification of its magnitude—an aspect often underexplored in earlier comparative studies.
Despite the clear structural advantages, the functional improvements remained variable, highlighting the importance of patient-specific factors. Jeon et al 18 reported reduced retear rates with ADM augmentation but no significant differences in ASES or Constant scores. Similarly, a multicenter trial by Barber et al 3 showed improved tendon integrity but no corresponding improvements in subjective outcomes. Although structural failure after rotator cuff repair is relatively common, its impact on clinical outcomes remains a subject of debate. Recent studies suggest that although short-term to midterm clinical outcomes may not be significantly affected, structural failure could lead to deterioration over the long term. Moreover, in superior capsular reconstruction using an ADM graft, one report indicated that a progressive reduction in graft volume over time may be associated with declines in clinical outcomes, suggesting that continued observation may be necessary to better understand the clinical implications. 26
In our study, 2 patch-related imaging findings were observed, although they were not classified as complications. First, marginal folding of the graft was identified in 3 patients on their 6-month follow-up MRI scans, despite no evidence of folding intraoperatively. These phenomena may be comparable to “dog-ear” deformities, which often remodel over time and appear to have limited clinical impact. 35 Second, subacromial bursitis was noted in 2 patients. We interpret this condition as a possible immune response to residual DNA or major histocompatibility complex proteins remaining in the graft, despite decellularization. 20 Further histologic studies are warranted to elucidate the underlying mechanisms mediating this process.
This study has several limitations. First, the minimum follow-up duration was 2 years, which may be insufficient to evaluate the long-term durability of ADM augmentation. Second, most retears occur within the first 6 months postoperatively 16 ; however, late retears can still occur beyond this period. Third, although propensity score matching improved group comparability, the matched sample size was smaller than that of the full cohort used in the regression analysis. Additionally, the sample size was determined via power analysis and was considered sufficient to detect meaningful differences in outcomes; however, the relatively small, matched groups may still have been underpowered to detect subtle differences in clinical outcome scores. Larger studies will be needed to validate these findings in the future. Fourth, factors such as the surgeon's learning curve, incremental changes in repair techniques, and variations in patient compliance over time were not controlled for and could have influenced outcomes.
Conclusion
In large-to-massive RCTs, ADM patch augmentation appeared to play a protective role in maintaining structural integrity. However, further studies are warranted to evaluate the long-term clinical outcomes of this repair approach.
Footnotes
Acknowledgements
We thank MID (Medical Illustration & Design), as a member of the Medical Research Support Services of Yonsei University College of Medicine, for providing excellent support with medical illustration.
Final revision submitted October 27, 2025; accepted October 28, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.