
Abstract
Background:
The inferior glenohumeral ligament (IGHL) contributes to anterior stability of the shoulder and elongates during anterior dislocation. However, the relationship between shoulder position and IGHL strain has not been fully elucidated. While previous studies have investigated ligament strain in abducted and externally rotated positions, no studies have examined ligament strain during internal and external rotation in a horizontally extended arm position. Furthermore, no studies have quantitatively evaluated IGHL elongation by replicating actual anterior dislocation.
Purpose:
To (1) measure strain in the IGHL in various shoulder positions and determine which positions contribute to anterior stability and to (2) assess strain in the IGHL and quantify ligament elongation after dislocation simulating anterior shoulder dislocation.
Study Design:
Descriptive laboratory study.
Methods:
Eight fresh-frozen cadaveric shoulders were used. The specimens were fixed in a custom-designed testing apparatus, and transducers were attached to the IGHL and axillary pouch to measure strain. The glenohumeral joint was fixed at 60° of abduction relative to the scapula. The angle of horizontal flexion-extension was varied from 30° of horizontal flexion to 30° of horizontal extension in 10° increments. Additionally, internal and external rotation angles were varied from maximal internal rotation to maximal external rotation. Strain in the IGHL was recorded for each position. Next, the arm was held at 60° of abduction and maximal external rotation and was manually extended horizontally until an anterior dislocation occurred. Strains and humeral head displacement during dislocation were measured. After dislocation, histopathological examination of specimens was performed.
Results:
The IGHL strain increased with the increase of horizontal extension and external rotation angles. In contrast, the strain in the axillary pouch did not change significantly with the increase of horizontal extension or external rotation angles. Anterior dislocation occurred in all shoulders. Two shoulders had Bankart lesions, 4 had bony Bankart lesions, and 2 had capsular tears. The mean maximal strain of the IGHL during dislocation was 19.9% ± 5.5%, while the maximal strain of the axillary pouch was 18.7% ± 7.5%. Histological analysis showed fiber discontinuity and disruption near both bony attachment sites, compared with the central portion of the IGHL.
Conclusion:
IGHL strain increased as horizontal extension and external rotation angles increased. The IGHL experienced a maximal strain of approximately 20% during an anterior dislocation.
Clinical Relevance:
The results of this study demonstrated that the IGHL undergoes a maximal strain of approximately 20% during an anterior dislocation. This finding may serve as a reference for determining the appropriate amount of ligamentous plication during Bankart repair. It might be appropriate to shorten the IGHL by 20% during Bankart repair.
It has been reported that anterior shoulder dislocation is often accompanied not only by a Bankart lesion but also by various associated injuries, including soft tissue injuries such as rotator interval lesions, inferior glenohumeral ligament (IGHL) elongation, capsular tears, and subscapularis elongation, as well as osseous lesions such as Hill-Sachs lesions and glenoid bone loss.8,14,19,23 When performing arthroscopic Bankart repair, the displaced anteroinferior labral–IGHL complex is first elevated from the glenoid rim and then shifted superiorly before reattaching to the glenoid. However, the degree of superior shift varies among surgeons. This variation exists because the extent of capsuloligamentous elongation due to dislocation is unknown, making it difficult to determine the appropriate amount of shift.
During shoulder dislocation, the glenoid labrum detaches from the glenoid and, simultaneously, the IGHL undergoes elongation. A biomechanical study using cadaveric shoulders and an optical tracking system reported that the capsule was strained by a mean of 3.5% during simulated dislocation. 15 A previous study that tested the failure strength and strain of the IGHL by applying traction along the ligamentous fibers in fresh cadaveric specimens found that the strain at ligament failure ranged from 16.8% to 27% in the entire IGHL and from 9.3% to 10.9% in the central portion.1,19,20 Another study that applied traction force to the IGHL in 90° of abduction and external rotation reported a mean failure strain of 7.2%. 19 Additionally, a biomechanical study measuring IGHL strain during subluxation reported irreversible strain of 3% to 7%, 12 with the primary strain occurring at the glenoid attachment site. 6 However, none of these experiments reproduced actual anterior dislocation; rather, they measured strain by applying traction force along the ligamentous fibers until failure. Therefore, the precise extent of IGHL elongation during actual dislocation remains unclear.
Recent motion analysis studies5,18 have shown that shoulder dislocation can occur not only in abduction and external rotation but also in hyperflexion or hyperabduction. Shoulder dislocations can also occur during a head-first slide 4 or with direct impact to the shoulder. 9 These findings suggest that Bankart lesions can occur in positions other than a so-called dislocation position, which is defined as abduction and external rotation. Thus, it is understandable that the IGHL becomes taut in various arm positions and that further anterior translation of the humeral head leads to Bankart lesion formation. However, few studies have investigated the extent of IGHL strain across different shoulder positions. We hypothesized that IGHL strain would be greatest in either abduction and maximal external rotation or maximal horizontal extension. Furthermore, we anticipated that the maximal strain during dislocation would exceed 3% to 10.9%1,11,17 previously reported. The purpose of this study was (1) to measure strain in the IGHL in various shoulder positions and determine which positions contribute to anterior stability and (2) to assess strain in the IGHL and quantify ligament elongation after simulating anterior shoulder dislocation in the abduction and external rotation position.
Methods
Specimens
This study used 8 shoulders from 4 fresh cadavers (mean age, 81 years; 3 males, 1 female). Cadavers with visible deformities, surgical scars, or shoulder joint contracture (defined as passive elevation ≤90° or external rotation ≤20°) were excluded. Specimens were prescreened using plain radiographs, and those with significant bony deformities or moderate to severe osteoarthritic changes were excluded. Additionally, shoulders with a macroscopically confirmed full-thickness rotator cuff tear were excluded. For histological comparison, 1 shoulder (age, 66 years) was used as a control. The youngest available control specimen was used, as it was considered to exhibit the least histological degeneration and to represent the most physiologically healthy condition. In this study, shoulder range of motion (ROM) was defined as the humeral angle relative to the scapula. The ROM of the cadaveric shoulders (mean ± SD) was as follows: 89°± 9° in abduction, 55°± 29° in horizontal extension, 37°± 12° in internal rotation at 0° of abduction, 58°± 23° in external rotation at 0° of abduction, 32°± 12° in internal rotation at 60° of abduction, and 69°± 24° in external rotation at 60° of abduction.
Specimen Preparation
The cadavers were stored at −40°C and thawed at room temperature 1 day before the experiment. The rotator cuff muscles and joint capsule were preserved, while the skin, subcutaneous soft tissue, and deltoid muscle were removed. The humerus was transected at the midshaft, and a custom-made rod was inserted into the medullary canal and fixed with resin for stabilization in the experimental apparatus. The subscapularis muscle was dissected at the muscle belly to expose the anterior capsule. The IGHL could be palpated and confirmed from outside the joint by placing the shoulder in an abducted and externally rotated position. The attachment sites for strain measurement were marked with 4-0 nylon sutures. The marking sites were 3 mm from the glenoid attachment of the IGHL and 15 mm along the fiber direction of the IGHL. Similarly, for measuring strain in the anterior axillary pouch, markings were made along its fibers from the 5-o’clock position of the glenoid. Before securing the specimen in the experimental apparatus, arthroscopy was performed via a posterior portal to evaluate the shoulder joint to check for the presence of Bankart lesions, bony lesions, and IGHL morphology and attachment sites. The location of the 4-0 nylon markers placed on the IGHL was also confirmed arthroscopically. During the experiment, water was sprayed every 5 minutes to keep the specimen hydrated, and the room temperature was maintained at 24°C.
Experimental Apparatus
The specimens were secured in a custom-designed experimental apparatus (Figure 1). To allow humeral head displacement measurement using a magnetic sensor, the apparatus was constructed entirely from acrylic, avoiding metal components. The moment of dislocation was recorded using a video camera. The scapula was firmly fixed by sandwiching the scapular body between acrylic plates. Resin was poured into any gaps to ensure rigid fixation. The scapular body was positioned perpendicular to the floor, aligning the humeral head's rotational center with the center of the apparatus. The intramedullary rod inserted into the humerus was connected to the apparatus. Based on a previous biomechanical study, 25 traction forces were applied to the subscapularis (10 N), supraspinatus (3.5 N), and infraspinatus (8.5 N) muscles to maintain the humeral head in the centered position. To measure rotational angles, a 1.5-mm Kirschner wire was inserted anteriorly into the humerus at the neutral rotation position. Angles were measured using a goniometer. The neutral rotation position was defined relative to the trunk and corresponded to 30° of external rotation relative to the scapular plane.

Custom-designed shoulder-positioning apparatus. A custom rod was connected to the humeral shaft, allowing the shoulder to be fixed in specific positions on the device. Arrowheads indicate the magnetic sensors attached to the lateral aspect of the greater tuberosity and the acromion. The square indicates the magnetic source.
Measurements
Strain was measured using strain transducers (Differential Variable Reluctance Transducer [DVRT]; MicroStrain). This transducer consists of a sliding core within a cylindrical housing that detects changes in electrical potential corresponding to tissue elongation or shortening. Each transducer was precalibrated by the manufacturer, allowing strain calculation based on voltage changes. The transducer had a measurement range of 6 mm, a resolution of 1.5 μm, and an accuracy of ±1.5%. 11 The transducers were secured to the IGHL and anterior axillary pouch using 4-0 nylon sutures previously placed. Nylon sutures were tied around the transducer rods wrapped in double-sided tape to ensure fixation (Figure 2). The transducers were connected to a 2-channel chart recorder (wireless voltage and temperature logger; Hioki E.E. Corp) for continuous data acquisition.
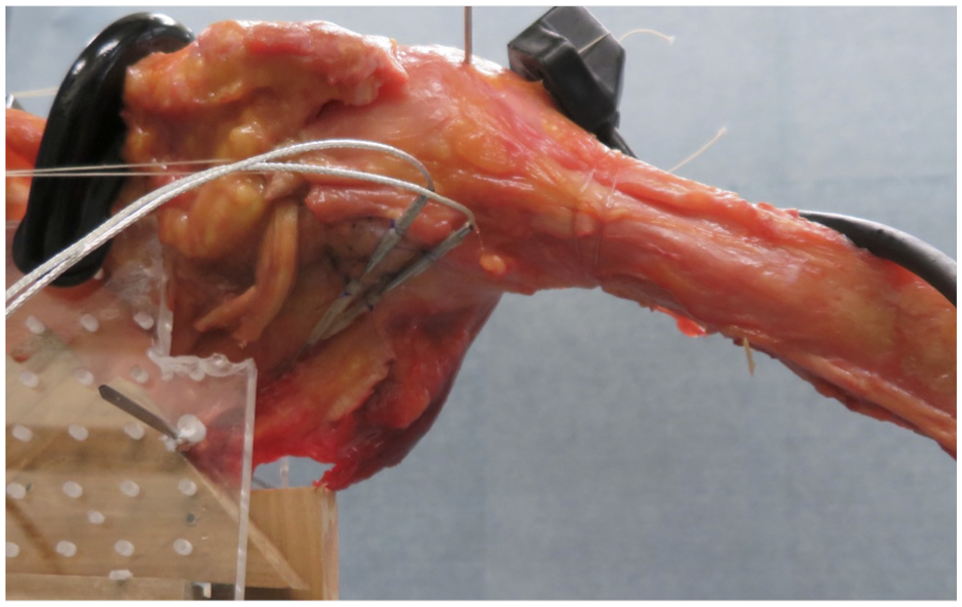
Placement of the transducers. The proximal transducer was positioned at the central width of the inferior glenohumeral ligament, 15 mm along the ligamentous fibers from its glenoid attachment. The other transducer was placed 15 mm from the 5-o'clock position of the glenoid, along the fibers of the anterior axillary pouch attachment.
Humeral head displacement during dislocation was measured using a magnetic tracking system (Fast Track System 4; Polhemus Navigation Sciences Division, McDonnell Douglas Electronics Co). The measurement accuracy of this system was a positional accuracy of 0.76 mm, an angular accuracy of 0.15°, and a response time of 4 ms. 17 The magnetic source was positioned adjacent to the dislocation apparatus, and sensors were attached to the proximal humerus and scapular spine. This coordinate system was defined as follows: the x-axis represented the anteroposterior direction, the y-axis represented the mediolateral direction, and the z-axis represented the vertical direction relative to the horizontal plane. Humeral head displacement relative to the glenoid was recorded in 3 dimensions.
Experimental Procedure
Strain Measurement in Various Shoulder Positions. The shoulder joint was fixed at 60° of abduction. The horizontal flexion-extension (HF-HE) angle was changed from 30° of HF to 30° of HE in 10° increments. At each flexion-extension position, internal and external rotation angles were adjusted from maximal internal rotation to maximal external rotation in 10° increments. Strain in the IGHL and anterior axillary pouch were also recorded at each position.
Anterior Shoulder Dislocation. After completing strain measurements across all positions, the shoulder was dislocated. Dislocation was performed manually following the method described by Etoh et al. 7 The shoulder was positioned in 60° of abduction and maximal external rotation, and horizontal extension was forcefully applied to translate the humeral head anteriorly, resulting in dislocation. To closely simulate real dislocations, horizontal extension was applied as rapidly as the experimental setup allowed. Strain and humeral head displacement were recorded continuously during the dislocation.
Micro–Computed Tomographic Examination. After dislocation, the specimen was removed from the apparatus, and the posterior capsule was incised to assess the anterior capsule from inside the joint. Macroscopic evaluation included identifying Bankart lesions, capsular or labral injuries, and bony defects. Bone-ligament-bone specimens, including the IGHL and anterior axillary pouch with their glenoid and humeral attachments, were harvested as 1-cm blocks. High-resolution micro–computed tomography (micro-CT; Latheta LCT-200, Hitachi Aloka Medical) was performed to analyze glenoid rim and ligament attachment sites. Imaging slices were aligned parallel to the IGHL fibers. The resolution of this micro-CT was 48 μm.
Histological Analysis
After micro-CT scanning, the specimens were sectioned along the IGHL fiber direction. The samples were decalcified, embedded in paraffin, and stained using Elastica-Masson for histological examination. For comparison, 1 shoulder that we did not dislocate was processed and analyzed using the same methods.
Sample Size and Power Analysis
The primary objective of this study was to quantitatively evaluate the elongation ratio of the IGHL during anterior shoulder dislocation. To assess the adequacy of the sample size, preliminary evaluations were conducted. Assuming a mean ± SD elongation of 20% ± 5%, the theoretical 95% CI with 8 specimens was approximately 16.5% to 23.5%, corresponding to a precision of ±3.5%, which was deemed acceptable for this study. In addition, a power analysis using a 1-sample t test (20% ± 5%; P = .05; power, 0.8) indicated a required sample size of approximately 3 specimens. Therefore, a sample size of 8 was considered sufficient for the purposes of this investigation.
Results
Observation of the Glenohumeral Joint
Arthroscopic inspection showed that the glenoid attachment of the anterior band of the IGHL was located between a mean of 2:54 o'clock (range, 1:30-4:00 o’clock) and 4:36 o'clock (range, 4:00-5:00 o’clock), with a mean central attachment at 3:00 o'clock (right shoulder orientation). The attachment of the middle glenohumeral ligament was located at a mean of 1:00 o'clock, while that of the superior glenohumeral ligament was at 0:40 o'clock on average. No Bankart lesions or labral tears were observed. Cartilage thinning was found in 2 glenoids and 1 humeral head. Three out of 8 shoulders had small, bursal-sided partial rotator cuff tears.
Strain in IGHL and Anterior Axillary Pouch Across Different Shoulder Positions
The strain measurements for IGHL in various shoulder positions are shown in Figure 3. IGHL strain increased with increasing external rotation and horizontal extension angles, with correlation coefficients of 0.34 (P < .001) and 0.27 (P < .001), respectively. Comparing IGHL strain among various external rotation angles, the strain at 80% of maximal external rotation angle and at maximal external rotation angle showed significantly greater strain compared with the 0% of maximal external rotation angle (P = .002 and .008, respectively). Additionally, the strain at maximal external rotation angle had significantly greater than the 20% of maximal external rotation angle (P = .02) (Figure 4). The highest IGHL strain was observed at 30° of horizontal extension and maximal external rotation, with a mean ± SD strain of 4.7% ± 4.8%. The correlation coefficient between IGHL strain at maximal external rotation and horizontal extension angle was 0.41 (P < .009).

Inferior glenohumeral ligament strain at different shoulder positions. HE, horizontal extension; HF, horizontal flexion. The x-axis represents external rotation as a percentage of the maximal external rotation angle (100%), and the y-axis shows IGHL strain (%). In HF10°, neutral (N), HE10°, HE20°, and HE30°, IGHL strain increased with greater external rotation. In HF20° and HF30°, IGHL strain remained relatively unchanged, even with increased external rotation.

Relationship between external rotation angle and inferior glenohumeral ligament strain. The x-axis represents the external rotation angle, normalized to 100% at maximal external rotation. The y-axis shows IGHL strain (%). The IGHL was significantly strained at 80% and 100% of the maximal external rotation angle compared with 0% external rotation. The IGHL was also significantly strained at maximal external rotation compared with 20% external rotation. Asterisks indicate statistical significance (P < .05)
The strain measurements for the anterior axillary pouch among different positions are shown in Figure 5. No significant strain increase was observed with changes in external rotation or horizontal extension angles.

Strain in the anterior axillary pouch at different shoulder positions. HE, horizontal extension; HF, horizontal flexion. The x-axis represents external rotation angle, normalized to 100% at maximal external rotation, and the y-axis shows strain in the anterior axillary pouch (%). No significant increase in strain was observed in the anterior axillary pouch with increasing external rotation across all positions.
Macroscopic Findings After Dislocation
After anterior dislocation, Bankart lesions were observed in 2 of the 8 shoulders, bony Bankart lesions in 4 shoulders, and capsular tears in 2 shoulders. The high incidence of bony Bankart lesions and capsular tears may be attributed to the use of elderly cadaveric specimens. The bony fragments associated with bony Bankart lesions corresponded precisely to the IGHL attachment site on the glenoid and included both cortical bone and part of the articular cartilage. No Hill-Sachs lesions were observed in any of the dislocated specimens.
IGHL Strain During Dislocation
The maximal strain in the IGHL during dislocation, as measured by the transducer, was 19.9% ± 5.5% (range, 8.7%-26.1%), while the maximal strain in the anterior axillary pouch was 18.7% ± 7.5% (range, 9.5%-24.2%). During IGHL failure, 3 distinct phases were observed: (1) toe region, (2) elastic region, and (3) rupture region. 2 In the toe region, the collagen fibers of the ligament were lax and when a load was applied, these fibers gradually straightened and aligned in the direction of the tensile force. As the tensile load increased, the ligament showed a nearly linear response in the load-displacement curve, which likely corresponded to the elastic region described in the previous study 2 , where collagen fibers were thought to be fully straightened and the ligament behaved elastically. When the applied force exceeded the elastic limit, the ligament transitioned into the rupture region, where permanent deformation occurred. In this phase, the strain curve leveled off near the maximal load after dislocation, which may indicate the onset of plastic deformation and the development of microdamage and fiber disruption, as suggested by the previous study. 2 The graph in Figure 6 illustrates the strain-time curve for a representative shoulder specimen.

Representative strain-time curve of a single shoulder. I indicates the toe region, II indicates the elastic region, and III indicates the rupture region. The white arrow indicates the point where the ligament ruptured. AP, anterior axillary pouch; IGHL, inferior glenohumeral ligament.
Humeral Head Displacement
To standardize the humeral head displacement across specimens of varying body sizes, displacement values measured along the x-axis, y-axis, and z-axis were normalized to each specimen's humeral head diameter and then multiplied by the mean humeral head vertical diameter (46.8 mm). 10 The humeral head displacement at IGHL rupture, measured using the magnetic sensor, was anterior displacement (x-axis) of 5.7 ± 1.9 mm, lateral displacement (y-axis) of 3.8 ± 1.1 mm, and inferior displacement (z-axis) of 2.5 ± 1.8 mm. The total linear displacement of the humeral head in 3-dimensional space was 7.5 ± 2.5 mm in the anterolateral-inferior direction. Relative to the glenoid, the humeral head displaced approximately 19% anteriorly and 7% inferiorly.
Micro-CT Examination
Bankart lesions, which were detachments of the IGHL from the glenoid, were observed, but no defects at the glenoid rim were noted. The fragments of bony Bankart lesion were triangular in shape, containing cortical bone from the articular surface of the glenoid, with IGHL attached to these fragments (Figure 7). No signs of glenoid rim impaction or compression were observed. There were no bony abnormalities at the humeral head attachment site of the IGHL.

Micro–computed tomographic images. (A) Bankart lesion: detachment of the IGHL from the glenoid was observed. No bony injury was detected at the glenoid rim. (B) Bony Bankart lesion (arrowheads): a bony fragment was detached at the IGHL attachment site, corresponding precisely with the ligament's insertion. IGHL, inferior glenohumeral ligament.
Histological Analysis
Histological examination of the IGHL attachment to bone showed distinct differences between normal control and dislocated specimens. In the normal control specimen, IGHL fiber bundles were thick and densely packed, with a high internal fiber density. In contrast, the dislocated specimens exhibited thinner IGHL fiber bundles and a reduced internal fiber density, as shown in Figure 8. High-magnification histological images of the glenoid attachment, ligament midsubstance, and humeral head attachment (Figure 9) further revealed notable structural changes. The glenoid and humeral head attachment sites displayed fiber discontinuities and void spaces within the ligament. Additionally, some ligamentous fibers were torn, indicating structural damage. Compared with normal specimens, the midsubstance of the IGHL in dislocated specimens demonstrated lower fiber density and the presence of small fissures.

Histological images from the glenoid rim to the ligament midsubstance (Elastica-Masson staining, low magnification). (A) Normal specimen: the midsubstance of the ligament exhibited high fiber density. Near the glenoid rim attachment, the fiber density was lower. (B) Dislocated specimen: Bankart lesion was observed (white arrowheads). Compared with the normal specimen, the dislocated specimen showed decreased overall staining intensity, reduced ligament thickness, and fiber bundle ruptures (black arrowheads).

Histological images of the inferior glenohumeral ligament (Elastica-Masson staining; high magnification ×400). Normal specimen: (A) glenoid side, (B) midsubstance, (C) humeral side. Dislocated specimen: (D) glenoid side, (E) midsubstance, (F) humeral side. The central portion displayed uniform fiber orientation with no fissures. In the dislocated specimen, partial fiber ruptures were observed at the glenoid and humeral attachment sites. Small fissures were present in these regions. In the midsubstance, no fiber rupture was observed, but staining intensity was reduced, and small fissures were present.
Discussion
The IGHL became increasingly tense with greater horizontal extension and external rotation in a position of 60º abduction. The highest IGHL strain was observed at 30° of horizontal extension combined with maximal external rotation, with a mean strain of 4.7% ± 4.8%. During anterior dislocation, maximal IGHL strain reached 19.9% ± 5.5%, while the anterior axillary pouch strain was 18.7% ± 7.5%. Histological analysis revealed fiber discontinuities and void spaces at both the glenoid and the humeral head attachment sites, with some fibers showing partial rupture. Additionally, the fiber bundle density in the ligament midsubstance was lower than in normal shoulders, with small fissures scattered throughout. Micro-CT examination demonstrated that bony Bankart lesion fragments were triangular and included cortical bone from the articular surface of the glenoid, with IGHL attached to these fragments.
This study found that maximal IGHL strain reached 19.9% ± 5.5% during anterior shoulder dislocation. In contrast, Bigliani et al 1 reported a maximal IGHL strain of 27% for the entire ligament. In their study, 16 fresh cadaveric shoulders (mean age, 72 years) were used, and the IGHL was harvested with its bony attachments to the glenoid and humerus for tensile testing along the ligament fibers. The maximal strain in the ligament midsubstance was reported as 10.9% ± 5.5%, which was approximately half the value observed in this study (10.9% ± 5.5%). Other biomechanical studies have also investigated IGHL strain: Stefko et al 19 conducted a tensile failure experiment using 13 fresh cadaveric shoulders (mean age, 71 years) in the abducted and externally rotated position and reported a maximal strain of 7.23% ± 2.25% in the ligament midsubstance. Ticker et al. 22 performed tensile testing on isolated IGHL specimens and found a maximal strain of 16.8% ± 4.6%. Two factors likely contributed to the differences between the present study and previous reports: (1) Differences in experimental setup; previous studies applied tension along the ligament fibers but did not reproduce actual dislocation, leading to differences in mechanical loading. (2) Measurement locations; some studies measured overall IGHL strain, while others focused only on the midsubstance. In the present study, both the glenoid attachment site and the midsubstance were assessed, which may explain the higher strain values compared with the midsubstance strain reported by Bigliani et al (11%). In contrast, the maximal strain observed in our study was slightly lower than the 27% strain they reported for the entire IGHL. Furthermore, whereas previous biomechanical studies primarily investigated IGHL strain at failure, the present study is the first to quantify IGHL strain in a shoulder dislocation model that replicates actual dislocation.
After anterior dislocation, 2 out of 8 shoulders had a Bankart lesion, while 4 shoulders had a bony Bankart lesion. The use of elderly cadaveric specimens was considered to have resulted in a higher incidence of capsular tears and bony Bankart lesions instead of Bankart lesions. The total incidence of Bankart lesions, including bony Bankart lesions, was 75%, which is comparable with the 87% to 100% incidence reported in clinical studies.3,16 This study used a dislocation method validated in previous research 7 , which reported an 87% incidence of Bankart lesions, closely matching the present findings. These results suggest that the dislocation method used in this study closely replicates clinically observed anterior dislocations.
Previous studies using transducers in fresh-frozen cadaveric shoulders measured IGHL strain at different abduction angles (0°, 30°, 45°, and 60°) and internal/external rotations in 10° increments. 24 These studies have reported that IGHL strain increases with abduction and external rotation. In this study, we confirmed increased strain with external rotation angle and additionally demonstrated that strain increased with horizontal extension angle. Taken together with previous reports, these findings suggest 3 key motion components related to IGHL tension: (1) abduction, (2) external rotation, and (3) horizontal extension. These findings suggest that Bankart lesions may occur in positions other than abduction and external rotation. For example, clinical observations have reported that in head-first sliding injuries, maximal flexion and external rotation can lead to Bankart lesions. In rugby tackles, even at lower abduction angles, forced maximal external rotation and horizontal extension may induce dislocation and Bankart lesions.
In normal specimens, the midsubstance of the IGHL appeared dense, with uniformly organized fiber bundles. However, the glenoid and humeral attachments of the IGHL were relatively loose and structurally heterogeneous. Previous studies have similarly reported that IGHL has a consistent thickness at both its bony attachment and the midsubstance. 21 While the midsubstance is densely structured, the bony attachment regions exhibit greater fiber heterogeneity. 22 Histological findings in dislocated specimens revealed minimal structural changes in the ligament midsubstance. On the other hand, thinning and partial fiber rupture were observed near the glenoid attachment. These results suggest that IGHL strain and mechanical stress are concentrated near the glenoid attachment during dislocation. This study represents the first histological analysis of dislocated IGHL specimens.
The transducer used in this study measured strain at the central portion of a 15-mm width. Because the total length of the IGHL ranges from a mean of 37.1 to 44.4 mm,13,21 it was necessary to carefully determine the placement location. In this study, the transducer was not positioned at the midportion of the ligament but rather near the glenoid attachment site and extending toward the midportion. There were 2 main reasons for this placement. The first reason is a biomechanical one. A finite element model study that simulated anterior dislocation and analyzed the strain distribution of the IGHL demonstrated that strain was concentrated at the glenoid attachment site. 6 Based on these findings, it was inferred that strain is greatest at the glenoid attachment, leading to the decision to place the transducer at this location. This interpretation is also supported by the findings of Bigliani et al, 1 who reported that the midsubstance strain was smaller than the overall strain of the ligament. The second reason is a histological one. The denser the fiber structure of a ligament, the less strain it undergoes under stress. A more uniform fiber structure provides greater tensile strength along the fiber direction. 2 Although the IGHL has a similar thickness in both the midsubstance and at the bony attachment sites, 21 it has been reported that the fiber structure is heterogeneous near the bony attachment but uniform and dense near the midsubstance. 22 The histological findings of normal ligament specimens in the present study showed a similar pattern. This suggests that, compared with the midsubstance, the glenoid attachment site is structurally weaker and more prone to strain. Previous studies using mechanical traction tests on IGHL specimens with their humeral and glenoid bone attachments intact have reported that overall ligament strain until failure ranged from 16.5% to 27%, while midsubstance strain was only 7.2% to 10.9%.1,19,21,22 These findings indicate that most of the strain occurs at the bony attachment sites, which likely contributes to IGHL detachment from the glenoid. To avoid underestimating strain measurements, the measurement region should include the area near the glenoid attachment rather than just the ligament midsubstance. Based on these considerations, in this study, the transducer was positioned at the central width of the IGHL, starting 3 mm from the glenoid attachment site and extending along the ligament fibers toward the midregion. Regarding the transducer placement for the anterior axillary pouch, anatomically, the ideal placement would be at the 6-o’clock position directly below the glenoid. However, due to the structure of the transducer, changes in the range of motion caused interference with soft tissues, making accurate measurements difficult. For this reason, the placement was adjusted to the 5-o’clock position, corresponding to the lower border of the IGHL.
Limitations
This study has several limitations. First, it was conducted as a time-zero condition and therefore does not account for any potential healing of the IGHL that could occur clinically. Second, a small capsular incision was made to vent the shoulder joint for intra-articular inspection before the experiment, which may have affected the strain patterns of the IGHL. The third limitation is that the mean age of the cadaveric shoulders used in this study was 81 years, which is considerably older than the younger population in whom shoulder dislocations occur more frequently. The injury patterns and postdislocation morphology may differ from those seen in younger individuals. In addition, capsular and ligamentous tissue in older specimens is typically stiffer, which may have influenced the observed strain patterns. However, obtaining cadaveric shoulders from younger individuals is not practically feasible, which remains a limitation of this study. The fourth limitation is that the dislocation maneuver was performed manually, meaning that the speed of dislocation and the force applied to the humeral head may not fully replicate actual dislocations. If a higher velocity or greater force had been applied, the results might have been different. The fifth limitation is that soft tissues such as the deltoid muscle were removed, and the scapula was completely immobilized, meaning that compensatory scapular movements were not replicated. Therefore, it was not possible to evaluate the potential contribution of the removed soft tissues to anterior shoulder stability or the effect that scapular motion might have on the strain experienced by the IGHL under physiological conditions. The sixth limitation is that dynamic stabilizers such as the rotator cuff muscles, which resist dislocation, were not replicated; therefore, their influence could not be taken into account. Finally, although the present study revealed that the IGHL undergoes approximately 20% strain during dislocation, this value cannot yet be directly applied in surgical practice. Clarifying the relationship between this strain and the amount of capsular plication remains a future challenge.
Conclusion
The IGHL became increasingly strained with greater external rotation and horizontal extension, reaching a maximal strain of approximately 5%. The IGHL experienced a maximal strain of approximately 20% during an anterior dislocation. Histological examination revealed that IGHL sustained greater damage at its glenoid and humeral attachments than in the ligament midsubstance.
Footnotes
Acknowledgements
We thank the staff of the Department of Anatomy for their assistance with specimen preparation, the technicians who created the pathological specimens, and Dr. Sato for valuable advice on the pathological findings.
Final revision submitted September 1, 2025; accepted September 18, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
The study was approved by the institutional ethics committee (#2022-1-121).