
Abstract
Background:
Postoperative emergency department (ED) utilization significantly reduces patient satisfaction and increases health care spending.
Purpose:
To identify the incidence, risk factors, and reasons for ED visits within 90 days of Achilles tendon repair (ATR).
Study Design:
Case-control study; Level of evidence, 3
Methods:
This study utilized the PearlDiver database to identify all instances of primary ATR. Patient age, sex, Elixhauser comorbidity index (ECI), region, and insurance coverage were extracted. The incidence, timing, and primary diagnoses for those with an ED visit 90 days post-ATR were extracted. Also, the 90-day total cost was determined and compared for those with and without a postoperative ED visit. Welch t test and Pearson chi-square test were used to determine significant differences between groups. Multivariable logistic regressions were used to determine risk factors associated with ED utilization after ATR.
Results:
Of the 82,604 patients with an ATR identified in the database, 6939 (8.4%) had ≥1 ED visit. Of ED visits, 1506 (21.7%) occurred in the first week after ATR and 3587 (51.7%) occurred in the first 4 weeks after ATR. The mean 90-day cost for those with an ED visit was significantly greater than those without an ED visit ($7330 ± $13,383 vs $3515 ± $5787; P < .001). Independent risk factors associated with ED utilization within 90 days were younger age (odds ratio [OR], 1.02; P < .001), female sex (OR, 1.26; P < .001), higher ECI (OR, 1.17; P < .001), a history of tobacco use (OR, 1.57; P < .001), and having Medicaid insurance (OR, 1.73; P < .001). Most ED visits within the first 2 weeks after ATR were for surgical-site pain (53.6%), with 62.4% of diagnoses being directly related to the surgical site. After 2 weeks following ATR, pain persisted as the most common reason for ED utilization (20.9%).
Conclusion:
More than 8% of patients had ≥1 ED visit within 90 days of ATR, with over half occurring in the first 4 weeks. This markedly increased health care spending. Addressing regional disparities, improving Medicaid acceptance policies, and enhancing perioperative care plans, such as multimodal pain management and addressing the psychological aspects of pain, may reduce the incidence and economic burden of postoperative ED visits.
Keywords
Achilles tendon ruptures are among the most common tendon injuries, with an annual incidence of 40 ruptures per 100,000 people.2,28,46 These injuries occur most often in middle-aged men participating in recreational sports; however, as people remain more active with age, there has been an increased incidence in the elderly population.8,22,24 Patients with Achilles tendon ruptures can undergo surgical intervention or nonsurgical treatment depending on relevant contextual patient factors and surgeon preference.9,33,55,57 Patients who undergo surgical intervention have higher risks of infection, nerve injury, and deep vein thrombosis as compared with those treated nonoperatively.20,33 These complications can lead to greater health care utilization, including hospital admissions and emergency department (ED) visits.
Hospital readmissions have widely been studied as a quality metric after orthopaedic procedures, with ED visits gaining attention in recent years, especially considering that ED visits have been associated with lower patient satisfaction and markedly increased health care costs.16,21,26,47 For Achilles tendon repairs (ATRs), postoperative hospital admissions are very rare, occurring in <1% of cases within 30 days. 51 However, to our knowledge, there are no studies evaluating ED visits 90 days post-ATR. An understanding of the incidence, risk factors, and reasons for ED visits after ATR may inform efforts to reduce ED utilization and improve patient satisfaction after ATR. Thus, the purpose of this study was to identify the incidence, risk factors, and reasons behind ED visits within 90 days of ATR.
Methods
Approval from our local institutional review board was deemed exempt for this study as all study data were publicly available and did not contain identifiable patient information.
Data Source
This study utilized the M165Ortho data set within PearlDiver (PearlDiver), which contains deidentified information in compliance with the Health Insurance Portability and Accountability Act. Data from 2010 to the third quarter of 2022 were analyzed, while PearlDiver has data to 2022, it was excluded as it was not a full year of data. At the time of our study, the M165Ortho database contained information on approximately 165 million orthopaedic patients, with payer sources encompassing commercial, Medicare, Medicaid, government, and cash claims. 36 The PearlDiver database has been widely used in orthopaedic outcomes research and has been validated in multiple prior studies.4,11,14,15
Study Cohort
All patients who previously underwent ATR were identified with the Current Procedural Terminology (CPT) codes 27650 (Achilles tendon rupture surgery; primary repair) and 27652 (Achilles tendon rupture surgery; primary repair with graft). Only primary ATRs were included; therefore, patients with CPT 27654 (Achilles tendon rupture surgery; revision or secondary repair) were excluded. Patients were also excluded from the study if they did not have adequate 90-day follow-up within the database. Patients with concomitant excision of Haglund deformity (CPT 28120) were included and accounted for in the multivariable logistic regression. Additionally, patients with chronic rupture repairs, defined as an ATR 30 days after rupture diagnosis,27,40 were included and accounted for in the multivariable logistic regression. International Classification of Diseases, Ninth Revision (ICD-9), and ICD-10 codes were used to identify patients with a diagnosis of Achilles tendon rupture (Supplemental Table 1).
Age, sex, Elixhauser comorbidity index (ECI) score, region of the country (West, South, Midwest, Northeast), tobacco use history, and insurance plan (Medicare, Medicaid, and commercial) for each patient who underwent ATR was extracted from the database. ECI score is an individualized measure of a patient's comorbidities with a higher score indicating a higher comorbidity burden. This metric has been used in multiple studies evaluating resource utilization after orthopaedic surgeries.6,16,18,41
ED Visits
ED visits 90 days after ATR were identified and quantified using the CPT codes 99281, 99282, 99283, 99284, and 99285. These codes correspond to varying levels of ED care. The yearly and weekly incidence of ED visits after ATR was determined, and, for comparison, the cohort's baseline weekly ED visits was determined by the number of ED visits approximately 1 year at ATR (mean of weeks 50-55). Also, the number of patients with 1, 2, 3, or >3 ED visits 90 days after ATR was determined by the number of ED visit codes within 90 days for each patient. The total cost 90 days following ATR was determined for each patient and means for patients with an ED visit and without an ED visit were compared. Costs were determined using the PearlDiver TotalCost function, which reflects the total insurer-paid amounts associated with each patient's episode of care (inclusive of facility and provider services).
The reasons for ED visits were determined from the ICD-9 and -10 diagnosis codes. All primary diagnoses for ED visits were extracted for each patient. These codes were manually categorized into 1 of 2 groups; diagnoses directly related to the surgical site and diagnoses unrelated to the surgical site. Diagnoses directly related to the surgical site were further subcategorized into pain, swelling/effusion, surgical-site infection, and other surgical-site problems. Other surgical-site problems included diagnoses for “other orthopaedic aftercare,”“removal of surgical wound dressing,” and “adjustment of orthopaedic devices.” Diagnoses unrelated to the surgical site were further subcategorized into central nervous system or psychiatric, gastrointestinal, infection outside the surgical site, cardiovascular, other musculoskeletal, respiratory, genitourinary, or other.
Statistical Analysis
Patient characteristics with and without postoperative ED visits were compared with univariate analysis. Continuous variables such as age and ECI were compared using Welch t test. Categorical variables such as sex, region, and insurance plan were compared using Pearson chi-square tests. Multivariable logistic regression was used to determine the patient factors associated with 90-day ED utilization after ATR. All statistical analyses were performed using the PearlDiver system. Significance was defined as P < .05.
Results
Incidence of ED Visits
In total, 85,177 primary Achilles tendon repairs were documented within the PearlDiver M165Ortho dataset that occurred from 2010 to 2022. Of these, 2573 (3.0%) were excluded due to insufficient follow-up, leaving a sample of 82,604 for analysis. There were 6939 (8.4%) patients who had ≥1 ED visit 90 days after the initial procedure (Figure 1). There were 5404 patients with only 1 ED visit after ATR, 1076 with 2 visits, 264 with 3 visits, and 195 with ≥4 visits within 90 days. The mean number of ED visits was 1.3 ± 0.7.

Flowchart of the final study cohort. ATR, Achilles tendon repair; ED, emergency department.
There was a steady increase in the incidence of postoperative ED visits from 2010 to 2020 (6.6%-9.8%) then a slight decrease from 2020 to 2021 (9.8%-7.0%) (Figure 2). Over half of the ED visits occurred in the first 4 weeks following ATR (n = 3587; 51.7%), with 1506 (21.7%) visits occurring in the first week post-ATR. For comparison, the mean number of ED visits that occurred approximately 1 year after ATR (mean of weeks 50-55) was 159 ± 12 (Figure 3).
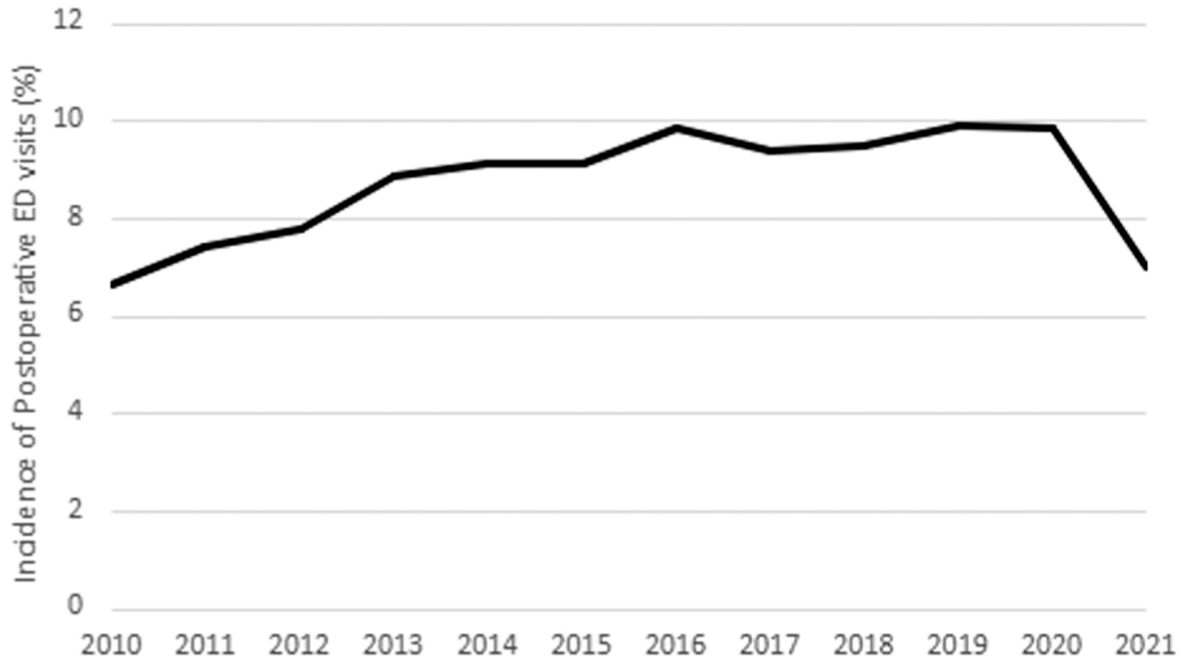
Yearly incidence of emergency department (ED) visits 90 days after Achilles tendon repair.

Emergency department (ED) visits per week after Achilles tendon repair. Weekly ED visit counts are shown for postoperative weeks 1-13, with the mean weekly ED visit rate during weeks 50-55 included as a baseline reference period.
The mean and median 90-day costs of care for those with a postoperative ED visit were $7330 ± $13,383 and $3805, respectively. For those without a postoperative ED visit, the mean and median 90-day costs were $3515 ± $5787 and $2235, respectively.
Factors Associated With 90-Day ED Visits. Detailed patient characteristics of the study cohort are summarized in Table 1. In this cohort, the mean age was 49.4 ± 13.9 years and consisted of a larger number of male compared with female patients (47,517 vs 35,087). The comorbidity burden of this cohort was low with a mean ECI of 2.7 ± 2.8. Upon univariate analysis, factors associated with increased utilization of the ED 90 days after ATR were younger age (P = .007), female sex (P < .001), higher ECI (P < .001), surgery performed in the Midwest (P < .001), and Medicaid insurance (P < .001) (Table 1).
Demographic Variables Compared Between Groups a

Data are presented as n (%) or mean ± SD. ECI, Elixhauser comorbidity index. The total number of patients in each region does not add to the total number of patients overall as some patients were classified as unknown and not listed on the table.
Upon multivariable logistic regression, female sex, higher ECI, a history of tobacco use, and having Medicaid insurance were independently associated with higher 90-day ED visits after ATR (Table 2), while younger age, surgery outside of the Midwest, diagnosis of an atraumatic as opposed to traumatic rupture, primary surgery done with a graft, and concomitant Haglund excision performed were associated with a lower number of ED visits 90 days after ATR (Table 2). An acute repair, defined as having an ATR within 30 days of an Achilles tendon rupture, was not associated with increased or decreased ED visits.
Multivariable Logistic Regression Results a

ATR, Achilles tendon repair; ECI, Elixhauser Comorbidity Index; OR, odds ratio. Bolded p value indicates statistical significance (p < 0.05).
Reasons for ED Visits
Within 2 weeks of ATR, 53.6% of ED visits were for pain in the lower leg and 62.4% were directly related to the surgery as categorized by pain, lower leg swelling, surgical-site infection, or other surgical-site issues (Figure 4). Cardiovascular, gastrointestinal, and respiratory categories had the largest number of patients outside of those categories directly related to the surgical site, and of these the most common diagnoses were chest pain, constipation, and shortness of breath, respectively. Deep vein thrombosis (DVT) comprised 34.3% of cardiovascular diagnosis, and 3.1% of total ED visits within 2 weeks.

Reasons for emergency department (ED) visits within 2 weeks of Achilles tendon repair (ATR). Orange lines are directly related to the surgical site, and blue lines are unrelated to the surgical site. CNS, central nervous system; CVS, cardiovascular system; GI, gastrointestinal; GU, genitourinary; MSK, musculoskeletal.
After 2 weeks following ATR, 39.1% of all ED visits were directly related to the surgical site. Pain of the surgical site persisted as the most common reason for an ED visit, encompassing 20.9% of all visits (Figure 5). Diagnoses classified as cardiovascular were the second most common reason, with 19.4% of all ED visits during this time. The most common cardiovascular diagnosis was chest pain (53.2% of all cardiovascular diagnoses). DVT made up 34.2% of all cardiovascular diagnoses and 6.5% of all ED visits after 2 weeks following ATR.

Reasons for emergency department (ED) visits 2 weeks after Achilles tendon repair (ATR). Orange lines are directly related to the surgical site, and blue lines are unrelated to the surgical site. CNS, central nervous system; CVS, cardiovascular system; GI, gastrointestinal; GU, genitourinary; MSK, musculoskeletal.
Discussion
The main findings of this study revealed that ED visits after ATR are a notable postoperative concern, with a rising incidence over time and occurring in 8.4% of patients throughout the study period. A large proportion of these visits occurred in the first 4 weeks postoperation, particularly within the first week, and were primarily for pain at the surgical site. This is largely consistent with prior literature evaluating the incidence of postoperative ED visits after other orthopaedic procedures.6,16,41 For example, Kammien et al 18 found that 8.3% of patients had ≥1 ED visit after anterior cruciate ligament reconstruction with 38% of those visits occurring in the first 2 weeks postoperatively, mostly for pain. Similarly, 11.5% of patients had ≥1 ED visit after ankle fracture surgery, with 33% of those visits occurring in the first 2 weeks postoperatively. 17 These findings demonstrate that the early postoperative period is a critical phase for patient recovery across various orthopaedic procedures. Moreover, our study identifies the incidence of ED visits over time, noting that their incidence after ATR has gradually increased from 2010 to 2020, with a slight decrease from 2020 to 2021. The reason for this is likely multifactorial. One contributing factor may be the increasing proportion of Medicaid patients, particularly following Medicaid expansion in 2010. 43 Because Medicaid coverage was independently associated with higher ED utilization in our study, the rise in Medicaid enrollment may partially explain the observed increase in ED visits over time. This remains concerning given the substantial cost burden of postoperative ED visits to both patients and the health care system.
Upon 90-day cost analysis, there was a substantial increase in costs associated with postoperative ED visits, emphasizing the economic burden associated with increased postoperative health care utilization. We found that the median 90-day cost for those with a postoperative ED visit was $3805, while the median cost for those without postoperative ED visit was $2235. This highlights the notable financial burden associated with ED utilization after ATR. Future efforts should focus on optimizing perioperative care and improving alternative care or follow-up care resources to help alleviate the increased burden on EDs.
This study identified multiple risk factors for postoperative ED utilization including younger age, female sex, and a higher comorbidity burden. Interestingly, older age has been associated with increased adverse outcomes after ATR, yet was associated with fewer ED visits.34,56 The reason for this discrepancy is likely multifactorial, involving factors such as overall health status, insurance status, or age-related differences in pain sensitivity. 32 Specifically, prior studies have found that older individuals report less overall pain postoperatively and may have been less likely to visit the ED for pain-related reasons in this study. 54 Female sex has previously been associated with poor outcomes after ATR, potentially explaining an increase in ED utilization after the procedure. 52 It was also found that regional differences and insurance coverage were predictors of ED utilization after ATR. Specifically, having surgery performed in the Midwest and Medicaid insurance were notable risk factors for increased ED utilization. The Midwest has previously been associated with increased ED utilization after other orthopaedic procedures including anterior cruciate ligament reconstruction and lumbar discectomy.18,42 This may be a result of reduced access to care. It has previously been reported that patients in rural areas have increased travel distances to primary care and notably longer wait times, potentially exacerbating ED utilization.25,30 Considering the Midwest has a large rural landscape, many patients may rely on the ED for timely access to care. 53 Furthermore, Medicaid patients often face barriers in accessing health care, potentially leading to an increased reliance on EDs for care.1,5 Wiznia et al, 58 for example, found that of the musculoskeletal urgent cares located in Connecticut, most did not accept Medicaid and were located in affluent neighborhoods. This is concerning considering musculoskeletal urgent cares have been shown to improve access to care, reduce health care costs for the patients, and reduce ED visits.3,35 Yet, the limited acceptance of Medicaid patients at these facilities disproportionately affects those most in need of accessible and affordable postoperative care. This suggests that addressing regional disparities in access to care and insurance acceptance policies may reduce the burden on EDs.
Along with several risk factors, we found that the vast majority of ED visits after ATR were for pain at the surgical site. This is similar to trends identified for other orthopaedic procedures including ankle fractures and total joint arthroplasty.16-19 This suggests there may be opportunity to improve pain management post-ATR, especially considering appropriate pain control not only benefits the well-being of the patient, but may also lead to earlier mobilization and faster rehabilitation.13,37,48 Several strategies to address postoperative pain after orthopaedic surgery have been extensively researched. Specifically, multimodal pain management, which combines various pharmacological and nonpharmacological interventions tailored to patients’ needs, has been shown to be particularly effective after common orthopaedic sports procedures. 29 Pharmacological interventions may include preoperative analgesics, nerve block catheters, and a postoperative pain regimen. 29 Nonpharmacological interventions may include appropriate progression to gradual weightbearing, which has shown to markedly improve tendon elasticity and strength as well as functional outcomes after ATR.7,12,45,50,38 Additionally, a person's psychological health may influence one's perception of pain. Pain catastrophizing, a negative cognitive-affective response to anticipated or actual pain, is common after orthopaedic surgery and results in worse pain-related outcomes.31,39 Kinesiophobia, or the fear of movement or reinjury, is also common and is linked to a higher perceived pain intensity. 23 After Achilles tendon rupture specifically, kinesiophobia was shown to prolongate return to sport and lead to increased pain at 6 months postoperatively. 49 Of note, Medicaid insurance and female sex has been associated with increased risk of pain catastrophizing.8,10 This may further explain an increased incidence of ED visits among these populations. Identifying and addressing psychological factors such as pain catastrophizing and kinesiophobia in postoperative care plans may improve pain management after ATR. Future research should look to investigate the effectiveness of interventions targeting the psychological factors of pain, such as cognitive-behavioral therapy and pain education, in reducing pain catastrophizing and kinesiophobia after ATR. 44
Strengths and Limitations
This study has several strengths. First, it represents the largest cohort to date evaluating ED utilization after Achilles tendon repair, with over 82,000 patients included. Second, the use of a national claims database allowed us to capture diverse patient demographics and payer types, improving the generalizability of our findings. Finally, by examining both patient-level risk factors and procedure-specific reasons for ED visits, our study provides actionable insights that may inform targeted perioperative interventions.
This study also has several limitations. As a retrospective database study, the study's accuracy is dependent on accurate administrative coding and aggregation of the data. In addition, because we relied on administrative diagnostic codes rather than full ED records, the precise clinical circumstances and management of each ED visit could not always be determined. Furthermore, complications that presented to outpatient settings such as primary care offices, walk-in clinics, or urgent care centers would not have been captured in this analysis, which may underestimate overall postoperative health care utilization. Cost analysis may be multifactorial and largely variable between patients regardless of the presence of a postoperative ED visit. The use of multivariable logistic regression can identify association but cannot prove causation despite accounting for a large number of covariates. Several important factors known to affect complications after ATR, such as surgical technique or anesthesia type, were unavailable in the database. We attempted to mitigate this by controlling for other operative factors that may influence outcomes such as the presence of a concomitant Haglund excision, acute versus chronic rupture repairs, and the use of a graft versus no graft. This study also did not evaluate specific comorbidities in influencing postoperative ED visits; rather, it used ECI as a proxy for the comorbidity burden of a patient. Furthermore, many diagnoses that may have been related to the surgery, such as constipation or pneumonia, were categorized as not being related, because observation-level information is not available in the database. Additionally, we were unable to control for laterality with both surgical and postoperative diagnoses, so we were ultimately unsure if ED visits for pain were related to the ipsilateral or contralateral leg. However, by stratifying ED diagnoses from 0 to 2 weeks and 2+ weeks, we were able to approximate the timing of these ED visits. Within the first 2 weeks after surgery, it is highly likely that many of the reasons for ED visits were related to the surgery. Despite these limitations, this study provides valuable insight into the incidence, risk factors, and reasons for postoperative ED visits after ATR.
Conclusion
More than 8% of patients had ≥1 ED visit within 90 days of ATR, with over half occurring in the first 4 weeks. This markedly increased health care spending and may contribute to the consumption of already limited ED resources. ED utilization increased among patients who were younger, female, had a higher comorbidity burden, had surgery in the Midwest, and had Medicaid insurance. Addressing regional disparities, improving Medicaid acceptance policies and enhancing perioperative care plans, such as multimodal pain management and the addressing of psychological aspects of pain, may reduce the incidence and economic burden of postoperative ED visits. In addition, improving patient education in the clinic, ensuring the availability of after-hours call services, and offering timely follow-up with providers or advanced practice providers may help redirect nonemergent issues away from the ED. Finally, future efforts should distinguish between ED visits for complications that require emergent intervention versus those for potentially preventable complaints, to optimize resource utilization and patient care pathways.
Footnotes
Appendix
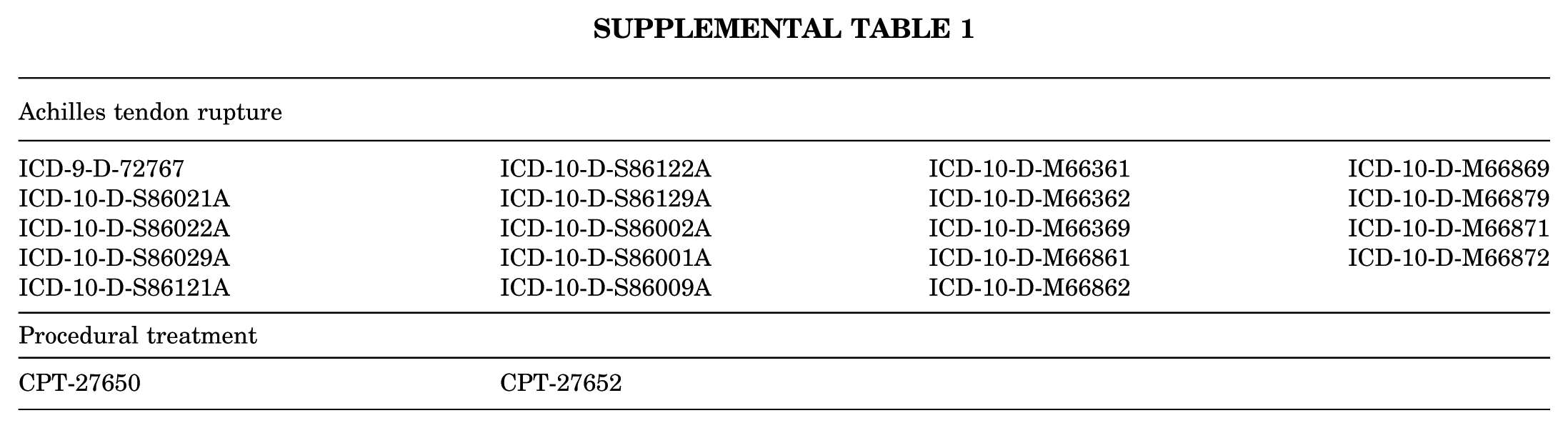
| Achilles tendon rupture | |||
|---|---|---|---|
| ICD-9-D-72767
ICD-10-D-S86021A ICD-10-D-S86022A ICD-10-D-S86029A ICD-10-D-S86121A |
ICD-10-D-S86122A
ICD-10-D-S86129A ICD-10-D-S86002A ICD-10-D-S86001A ICD-10-D-S86009A |
ICD-10-D-M66361
ICD-10-D-M66362 ICD-10-D-M66369 ICD-10-D-M66861 ICD-10-D-M66862 |
ICD-10-D-M66869
ICD-10-D-M66879 ICD-10-D-M66871 ICD-10-D-M66872 |
| Procedural treatment | |||
| CPT-27650 | CPT-27652 | ||
Final revision submitted October 11, 2025; accepted October 21, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Approval from the local institutional review board of Mayo Clinic was deemed exempt for this study, as all study data were publicly available and did not contain patient information.